HRH Profile for Punjab 2012.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

HEALTH Sep 31St, 2013 - Volume:1, Issue: 4
HEALTH Sep 31st, 2013 - Volume:1, Issue: 4 Epidemic control: Dengue counters set up at LGH IN THIS BULLETIN Seven more dengue patients confirmed in Mayo Hospital Lahore Punjab health department put on alert over Congo fever Health News 2-11 Dengue on the rise in Punjab Polio eradication: Provinces endorse three-year plan Healt deartments and Monitoring 12-13 Swat Declares Health Emergency Over Dengue bodies Publications WHO rings alarm over measles Anti –Measles drive delayed due to finance ministry stubbornness Balochistan EQ 2013 - Potentially 14 58m have no access to safe drinking water Affected Health Facilities Contamination risks: Think twice before you take a sip of your tap water Govt committed to making Pakistan polio-free: PM Health Response by Humanitarian 15-18 Precautionary measures: Health officials prepare to tackle Congo virus Post-natal screening: Sindh Assembly passes ‘newborn screening bill’ Partners in Awaran EQ - Balochistan PM lauds Bill Gates’ support on polio eradication in Pakistan LHC rebukes health DG in measles case District Health Profile Peshawar 19 Micro plan NID polio round from Sept Polio virus: BA voices fear Pakistanis might face travelling ban Urdu News 20-23 Meeting with PM: Donors share anguish over polio campaign First sexual health curriculum launched in Pakistan Health Maps 24-27 Balochistan Health department on high alert Pakistan lagging behind in child survival, maternal health development Health Directory 28-46 WHO polio chief in Pakistan honoured DRUG USE IN PAKISTAN 2013 KECH - POTENTIALLY -

Licensure Examiantio
Pakistan Nursing Council, Islamabad. Licensing Examination for BSN Examination 2015-2 ARMED FORCE POST GRADUATE MEDICAL ISNTITUTE (AFPGMI) S.NO. Name Father Name CNIC No. Remarks Centre Attempt No DD No Amount Bashir Ahmed 1 Abberaha Naz 42401-2618603-2 Islamabad 792957 2000 Shahid 2 Farzana Taufiq Mirza 16202-2930865-6 Islamabad 79303 2000 500 fee 3 Sumera Yasmin sahasar khan 37203-4673615-4 needed Islamabad 70706 1500 SHIFA COLLEGE OF NURSING ISLAMABAD Remarks Centre S.NO. Name Father Name CNIC No. Attempt No DD No Amount Islamabad 4 Abdullah Sultanat Khan 15101-8207671-1 1008908 2000 Islamabad 5 Abdur Rehman Abdul Latif 17301-6589898-7 1st 8031008428 2,000 Mohammad Islamabad 6 Abid Ali 15602-0668939-5 1008908 2000 Ismail Islamabad Ahsan Amir Amir 7 1st 8031008430 2,000 Muhammad Muhammad 38403-3581739-3 Islamabad 8 Anila Anjum Sabab Khan 71402-6658390-6 1st 8031008477 2,000 2nd 9 Anwar Iqbal Sabir Khan 15602-4829339-9 79556 2000 Islamabad attempt Islamabad 10 Aqeel Abbas Allah Ditta 37202-8201118-7 1008908 2000 Islamabad 11 Asif Akbar Fazal Akbar 16202-9802737-3 1008908 2000 Islamabad 12 Asif Gill Younas Gill 38403-7740542-9 1st 8031008420 2,000 Islamabad 13 Atif Mehmood Ishtiaq Ahmad 37201-4030497-5 1008908 2000 Islamabad 14 Barnabass llyas Shaker 36502-2600676-7 1008908 2000 Gul Jehan Islamabad 15 Bilal Ahmad 1st 8031008429 2,000 Said 15705-8233767-7 Islamabad 16 Daniyal Siddiqi Zaheer Siddiqi 61101-5165094-7 1008908 2000 Islamabad 17 Ele Moses Robin Dean 36104-4913461-7 1008908 2000 Islamabad 18 Farah Riasat Riasat Ali 37405-5982626-2 -

Diagnostic Centers'!A1 Laboratories!A1 Dental Centers'!A1 Ophthalmology Clinics'!A1 Medical Center'!A1 Diagnostic Centers
Diagnostic Centers'!A1 Laboratories!A1 Dental Centers'!A1 Ophthalmology Clinics'!A1 Medical Center'!A1 Diagnostic Centers L I S T O F A L L I A N Z E F U N E T W O R K D I S C O U N T D I A G N O S T I C C E N T R E S S.No Hospital Name Address Contact Contact Person Email Contact Number City Discount Category 021-35662052 Mr. Yousuf Poonawala 1 Burhani Diagnostic Centre Jaffer Plaza, Mansfield Street, Saddar, Karachi. 021-5661952 Karachi 10-15% Diagnostic Center 0336-0349355 (Administrator) [email protected] 02136626125-6 0334-3357471 [email protected] 2 Dr. Essa's Laboratory & Diagnostic Centre (Main Centre) B-122 (Blue Building) Block-H, Shahrah-e-Jahangir, Near Five Star, North Nazimabad. Mr. Shakeel / Ms. Shahida 021-36625149 Karachi 10-20% Diagnostic Center 0335-5755529 [email protected] 021-36312746 0335- 2.1 Ayesha Manzil Centre Ali Appartment, FB Area Karachi Karachi 10-20% Diagnostic Center 5755536 021-35862522 021- 2.2 Zamzama Centre Suite # 2, Plot 8-C (Beside Aijaz Boutique), 4th Zamzama Commercial Lane Karachi 10-20% Diagnostic Center 35376887 2.3 Medilink Centre Suite # 103, 1st Floor, The Plaza, 2 Talwar, Khayaban-e-Iqbal, Main Clifton Road, Karachi 021-35376071-74 Karachi 10-20% Diagnostic Center 2.4 Abdul Hassan Isphahani Centre A-1/3&4, Block-4, gulshan-e-Iqbal. Main Abdul Hassan Isphahani Road, Karachi 021-34968377-78 Karachi 10-20% Diagnostic Center 2.5 KPT Centre Karachi Port Trust Hospital Keemari, Karachi 021-34297786 Karachi 10-20% Diagnostic Center 021-34620176 021- 2.6 Gulistan-E-Johar Centre S -
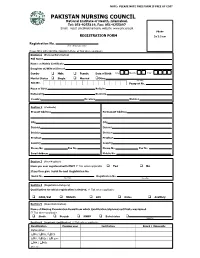
PNC Registration For
NOTE: PLEASE NOTE THIS FORM IS FREE OF COST PAKISTAN NURSING COUNCIL National Institute of Health, Islamabad. Tel: 051-9255119, Fax: 051-9255097 Email: [email protected], website: www.pnc.org.pk Photo REGISTRATION FORM 3x 3.5 cm Registration No. (For office use only) Please fill in with CAPITAL (BLOCK) letters. Tick where applicable Section 1 (Personal Information) Full Name Name on Matric Certificate Daughter of/Wife of/Son of Gender Male Female Date of Birth Day Month Year Marital Status Single Married Other (Specify) NIC No. Passport No. Place of Birth Religion Nationality Domicile Country Province Division Section 2 (Contacts) Present Address Permanent Address City City District District Division Division Province Province Country Country Phone No. Fax No. Phone No. Fax No. Email Address Mobile No. Section 3 (Ever Register) Have you ever registered with PNC? Tick where applicable Yes No If yes then give Serial No and Registration No. Serial No. Registration No. (Specify) (Specify) Section 4 (Registration Category) Qualification for which registration is desired. Tick where applicable NAID/Dai Midwife LHV Nurse Auxiliary Section 5 (Board Information) Name of Nursing Examination Board from which Qualification/diploma/certificate was issued. Tick where applicable Sindh Punjab NWFP Balochistan (Specify) Section 6 (Academic Qualification) Tick where applicable Qualification Passing year Institution Board / University Matriculation FA / FSc / ICS BA / BSc / B.com MA / MSc Other (s) Section 7 (Professional Qualification) -
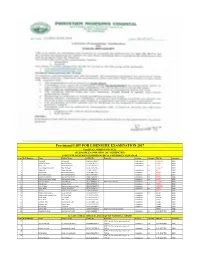
Provisional LIST for LISENSURE EXAMINATION 2017
Provisional LIST FOR LISENSURE EXAMINATION 2017 PAKISTAN NURSING COUNCIL LICENSURE EXAMINATION 2017 GENERIC BSN INSTITUTE OF NURSING KHYBER MEDICAL UNIVERSITY PESHAWAR Sr no Roll Number Name Father Name CNIC No. Remarks Centre Attempt DD No Amount 1 Irfanullah Rahmat Ali 15602-3994101-9 Isalamabad No 15435753 2000 2 Syed Afzal Shah Abdul Ghafoor 17101-1705973-7 Isalamabad 90635 2000 3 Afrooz Bibi Bakht Sherawan 15602-6846449-2 Isalamabad 1st 90636 2000 4 Shazad Aman-E-Room Sher Bahadar 15302-9095234-5 15086719 2000 5 Abbas Ali Khan Badshah 15306-3594812-1 Isalamabad 1st 90577 2000 6 Afzal Akber Muhammad Ishaq 15705-9827246-1 Islamabad 90638 2000 7 Muhammad Ayaz Muhammad Khitab 17301-5471894-1 Islamabad 1st 90575 2000 8 Muhammad Faizan Muhammad Sharif 17301-1655450-1 Islamabad 1st 90579 2000 9 Muhammad Uzair Akhtar Muhammad Akhtar 17301-5064391-1 Islamabad 1st 90576 2000 10 Parveen Akhtar Abdul Ghani 17101-5484531-4 Internship required Islamabad 1212582 2000 11 Riaz Ahmad Ahmad Sahib 15601-3703290-1 Islamabad 1st 90578 2000 12 Siraj-Ul-Haq Muhammad Anwar Shah 15303-9296087-5 Islamabad 15435757 2000 13 Wiqar Ullah Hassan Wali Khan 15701-3952070-7 Islamabad 1st 90573 2000 14 Shaista Muhammad Shah Khan 15605-0565468-6 99637 2000 15 Muhammad Zakaria Fazal Rahman 15302-9139655-5 Islamabad 1st 30729 2000 16 Muhammad Yaseen Khan Yar Min Khan 21201-4177450-5 Islamabad 30686 2000 17 Shah Faisal Taza Khan 21201-7956505-7 Islamabad 30694 2000 18 Shafi Ullah Sher Zada 15602-2637949-5 Islamabad 30687 2000 19 Tasleem Tahir Muhammad Tahir 15101-7887650-4 Islamabad 30690 2000 20 Naseem Bibi Bacha Zada 15101-1230463-0 Islamabad 30688 2000 21 Nusrat Bibi Sulaiman 15101-3072593-2 Islamabad 30689 2000 22 Sehrish Bibi Syed Rehmat Shah 13302-7576063-8 Original Internship required 30707 2000 23 Mumtaz Ali Khan Muhammad Shafiq 15601-0489893-7 Islamabad 1st C-04-2017-702 2000 ALLAMA IQBAL MEDICAL COLLEGE OF NURSING LAHORE S.NO Roll Number Name Father Name CNIC No. -

COHRED Paper Research to Action and Policy PAKISTAN Mary Hilderbrand, Jonathan Simon, and Adnan Hyder Pakistan Faces a Wide Arra
COHRED paper Research to Action and Policy PAKISTAN Mary Hilderbrand, Jonathan Simon, and Adnan Hyder Pakistan faces a wide array of health challenges, including communicable diseases and nutritional deficiencies connected with poverty and low levels of development, as well as non- communicable conditions more commonly associated with affluent countries. The former are major contributors to the national disease burden. The extent to which they continue to threaten and diminish the well-being of Pakistan’s children is of particular concern. Conquering them will require a wide range of resources and actions, some well beyond the concerns of health policy. But how effectively health policy and programs address the challenges remains critical, and health research can potentially be an important contributor to effective, efficient, and equitable policies and programs. Since at least 1953, with the founding of the Pakistan Medical Research Council (PMRC), Pakistan has officially recognized the importance of research in solving the health problems of the country. There have been repeated calls for more support for health research and for such research to be utilized more fully in policy. The 1990 and 1998 National Health Policies both mentioned research utilization as important and pledged to strengthen it (Government of Pakistan, Ministry of Health, 1990 and 1998). A process of defining an essential national health research agenda occurred in the early nineties and recently has been rejuvenated (COHRED 1999). We conducted a study to understand better the role that research plays in child health policy and programs in Pakistan.1 In open-ended, in-depth interviews, we asked informants about their views on health research and policy generally in Pakistan and about their own experience in linking research with policy. -

Health Bulletin July.Pdf
July, 2014 - Volume: 2, Issue: 7 IN THIS BULLETIN HIGHLIGHTS: Polio spread feared over mass displacement 02 English News 2-7 Dengue: Mosquito larva still exists in Pindi 02 Lack of coordination hampering vaccination of NWA children 02 Polio Cases Recorded 8 Delayed security nods affect polio drives in city 02 Combating dengue: Fumigation carried out in rural areas 03 Health Profile: 9-11 U.A.E. polio campaign vaccinates 2.5 million children in 21 areas in Pakistan 03 District Multan Children suffer as Pakistan battles measles epidemic 03 Health dept starts registering IDPs to halt polio spread 04 CDA readies for dengue fever season 05 Maps 12,14,16 Ulema declare polio immunization Islamic 05 Polio virus detected in Quetta linked to Sukkur 05 Articles 13,15 Deaths from vaccine: Health minister suspends 17 officials for negligence 05 Polio vaccinators return to Bara, Pakistan, after five years 06 Urdu News 17-21 Sewage samples polio positive 06 Six children die at a private hospital 06 06 Health Directory 22-35 Another health scare: Two children infected with Rubella virus in Jalozai Camp Norwegian funding for polio eradication increased 07 MULTAN HEALTH FACILITIES ADULT HEALTH AND CARE - PUNJAB MAPS PATIENTS TREATED IN MULTAN DIVISION MULTAN HEALTH FACILITIES 71°26'40"E 71°27'30"E 71°28'20"E 71°29'10"E 71°30'0"E 71°30'50"E BUZDAR CLINIC TAYYABA BISMILLAH JILANI Rd CLINIC AMNA FAMILY il BLOOD CLINIC HOSPITAL Ja d M BANK R FATEH MEDICAL MEDICAL NISHTER DENTAL Legend l D DENTAL & ORAL SURGEON a & DENTAL STORE MEDICAL COLLEGE A RABBANI n COMMUNITY AND HOSPITAL a CLINIC R HOSPITALT C HEALTH GULZAR HOSPITAL u "' Basic Health Unit d g CENTER NAFEES MEDICARE AL MINHAJ FAMILY MULTAN BURN UNIT PSYCHIATRIC h UL QURAN la MATERNITY HOME CLINIC ZAFAR q op Blood Bank N BLOOD BANK r ishta NIAZ CLINIC R i r a Rd X-RAY SIYAL CLINIC d d d SHAHAB k a Saddiqia n R LABORATORY FAROOQ k ÷Ó o Children Hospital d DECENT NISHTAR a . -

Missed Immunization Opportunities Among Children Under 5 Years of Age Dwelling in Karachi City Asif Khaliq Aga Khan University, [email protected]
eCommons@AKU Department of Paediatrics and Child Health Division of Woman and Child Health October 2017 Missed immunization opportunities among children under 5 years of age dwelling In Karachi city Asif Khaliq Aga Khan University, [email protected] Sayeeda Amber Sayed Aga Khan University Syed Abdullah Hussaini Alberta Health Service Kiran Azam Ziauddin Medical University, Karachi Mehak Qamar Institute of Business Management, Karachi Follow this and additional works at: https://ecommons.aku.edu/ pakistan_fhs_mc_women_childhealth_paediatr Part of the Immunology and Infectious Disease Commons, and the Pediatrics Commons Recommended Citation Khaliq, A., Sayed, S., Hussaini, S., Azam, K., Qamar, M. (2017). Missed immunization opportunities among children under 5 years of age dwelling In Karachi city. Journal of Ayub Medical College, Abbottabad : JAMC, 29(4), 645-649. Available at: https://ecommons.aku.edu/pakistan_fhs_mc_women_childhealth_paediatr/388 J Ayub Med Coll Abbottabad 2017;29(4) ORIGINAL ARTICLE MISSED IMMUNIZATION OPPORTUNITIES AMONG CHILDREN UNDER 5 YEARS OF AGE DWELLING IN KARACHI CITY Asif Khaliq, Sayeeda Amber Sayed*, Syed Abdullah Hussaini**, Kiran Azam***, Mehak Qamar*** Department of Paediatrics and Child Health, The Aga Khan University Hospital, Karachi, *Alberta Health Services, Calgary-Zone- Canada, **Ziauddin Medical University, Karachi, ***Department of Health and Hospital Management, Institute of Business Management, Karachi-Pakistan Background: Immunization is the safest and effective measure for preventing and eradicating various communicable diseases. A glaring immunization gap exists between developing and industrialized countries towards immunization, because the developing countries including Pakistan are still striving to provide basic immunization to their children. The purpose of this study was to access the prevalence and factors of missing immunization among under 5-year children of Karachi. -

Adding It Up: Costs and Benefits of Meeting the Contraceptive and Maternal and Newborn Health Needs of Women in Pakistan
Adding It Up: Costs and Benefits Of Meeting the Contraceptive and Maternal and Newborn Health Needs of Women in Pakistan Aparna Sundaram, Rubina Hussain, Zeba Sathar, Sabahat Hussain, Emma Pliskin and Eva Weissman Key Points ■■ Modern contraceptive services and maternal and newborn health care are essential for protecting the health of Pakistani women, their families and communities. ■■ Based on data from 2017, women in Pakistan have an estimated 3.8 million unintended pregnancies each year, most of which result from unmet need for modern contraception. ■■ About 52% of married women of reproductive age (15–49) who want to avoid a pregnancy are not using a modern contraceptive method. If all unmet need for modern contraception were met, there would be 3.1 million fewer unintended pregnancies annually, 2.1 million fewer induced abortions and nearly 1,000 fewer maternal deaths. ■■ Pakistan is currently spending US$81 million per year on contraceptive services. Serving the full unmet need for modern contraception would require an additional US$92 million per year, for a total of US$173 million, based on public-sector health care costs. ■■ At current levels of contraceptive use, providing maternal and newborn health care to all women who have unintended pregnancies, at the standards recommended by the World Health Organization, would cost an estimated US$298 million. ■■ If all women wanting to avoid a pregnancy used modern contraceptives and all pregnant women and their newborns received the recommended care, the country would save US$152 million, compared with a scenario in which only maternal and newborn health care were increased. -

Calculus Renal Failure; a Study to Profile the Calculus Renal Failure and Its 1
CALCULUS RENAL FAILURE The Professional Medical Journal www.theprofesional.com ORIGINAL PROF-4941 DOI: 10.29309/TPMJ/18.4941 CALCULUS RENAL FAILURE; A STUDY TO PROFILE THE CALCULUS RENAL FAILURE AND ITS 1. MCPS (Surgery), FCPS (Urology) SIU Fellow Urology Nephrology MANAGEMENT STRATEGY Centre Mansoura Egypt Fellowship in Uro Oncology Assistant Professor of Urology Azfar Ali1, Ghulam Ghous2, Zakariya Rashid3, Nabeel Shafi4, Irshad Ali5, Department of Urology & Renal Muhammad Hassam Khalid6, Muhammad Safdar Khan7 Transplant AMC/PGMI/Lahore General Hospital ABSTRACT… Background: Urolithiasis is a common urological disease in Pakistan. Calculus Lahore. renal failure is a urological emergency that required immediate intervention to prevent further 2. FCPS Urology Senior Registrar Urology deterioration of renal function. Objectives: The purpose of this study is to present clinical profile SIMS/Services Hospital Lahore. of calculus renal failure patient and to report our experience of management of such patients. 3. FCPS, MRCS(Ed) Study Design: Descriptive Cross sectional study. Setting and Period: Department of urology Assistant Professor Surgery Aziz Fatima Medical & Dental Services Hospital from July 2015 to December 2016 were included. Materials and Methods: College Faisalabad. Patients of all ages of either sex who presented with calculus renal failure. The patients with 4. FCPS Urology obstructive uropathy due to causes other than stone disease were excluded. Demographic Senior Registrar Urology information along with detailed history recorded. Baseline investigations included Complete SIMS/Services Hospital Lahore. 5. MBBS blood counts, serum creatinine, serum electrolytes and ultrasound for KUB. For stone position Registrar Urology Xray KUB in every case & CT in selected cases performed. Functional status of individual kidney SIMS/Services Hospital Lahore. -

Investigation on the Prevalence of Leukaemia at a Tertiary Care Hospital, Lahore
INVESTIGATION ON THE PREVALENCE OF LEUKAEMIA AT A TERTIARY CARE HOSPITAL, LAHORE NIGHAT NASIM, KALIMUDDIN MALIK, NAUMAN A. MALIK SHAISTA MOBEEN, SAUD AWAN AND NAGHMANA MAZHAR Department of Pathology, PGMI / Lahore General Hospital, Lahore ABSTRACT Introduction: Cancer in all forms is causing about 12% deaths throughout the world. After recent advances and improvement in treatment and prevention in cardiovascular diseases, tumour is an important cause of morbidity and mortality. 1 The incidence of leukaemia across the world is 1 per 100,000 annually. It contributes to 25% of childhood cancers. 2 The study was designed to investi- gate the Prevalence of Leukemia subtypes at Lahore General Hospital / The Graduate Medical Insti- tute, Lahore and was carried out in the Bone Marrow Clinic. The study was cross – sectional pros- pective. The period of the study was two year from 01 June, 2010 to 30 June, 2012. Methodology: Complete blood counts, bone marrow aspiration and trephine biopsies were perfor- med according to standard methods. Results: In a total of 45 cases of leukaemia, acute leukemia was more prevalent than chronic leu- kaemia. The ratio of acute and chronic leukaemias was 4:1. Male to female ratio was 1.3: 1. Most of the patients (42%) were below the age of 15 years. ALL (49%) was more common than AML (31%). Among chronic leukaemias, CML (16%) was more common than CLL (2%) and CMML (2%). The study of acute leukaemia subtypes revealed that ALL – L2 was more common (77%) than L 1 (24%). In AML subtypes, M3 (57%) was most prevalent while M 2 (14%) and M 4 (14%) and M 1 (7%) and M 6 (7%) were less prevalent of leukaemia subtypes. -

Pakistanmamau Trainingstudyjun5 Al Edited Ah Ah
Reinvigorating the Postpartum IUCD Using a Low-Cost Simulation Model Overview Jhpiego Pakistan, in collaboration with Saving Lives at Birth, conducted a study trial of a new, portable, low-cost training simulation model called Mama-U. Designed in partnership with Laerdal Global Health, the Mama-U was developed specifically to train health care providers on the insertion of the postpartum intrauterine contraceptive device (PPIUCD). The main objectives of this study were to measure acceptability and appropriateness of the Mama-U, feasibility of this technology, confidence of providers during training and retention of provider skills associated with this new training simulation model. Given that the PPIUCD is new to family planning programs in Pakistan, the Mama-U was introduced to facilitate effective training of physicians, nurses and midwives to improve their insertion skills for placement of an IUCD after birth and to reduce the rate of expulsion. Eighty-eight health care providers—the majority of whom were physicians—participated in the study and were trained using the Mama-U model. Seventy clients were interviewed in a follow- up to the study. The key findings were: • 82% of the providers trained using the Mama-U model stated that they felt confident in providing PPIUCD services. Overall, 85% of providers could perform the procedure at two-month follow-up according to standards. • 78.6% of clients counseled using the simulation model said that seeing the model demonstration helped them decide to accept PPIUCD. • Of all the providers trained, 97% were in favor of the model and recommended using the Mama-U in future trainings, while 91% of clients would recommend PPIUCD to their families and others based on their experience.