PNC Registration For
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Licensure Examiantio
Pakistan Nursing Council, Islamabad. Licensing Examination for BSN Examination 2015-2 ARMED FORCE POST GRADUATE MEDICAL ISNTITUTE (AFPGMI) S.NO. Name Father Name CNIC No. Remarks Centre Attempt No DD No Amount Bashir Ahmed 1 Abberaha Naz 42401-2618603-2 Islamabad 792957 2000 Shahid 2 Farzana Taufiq Mirza 16202-2930865-6 Islamabad 79303 2000 500 fee 3 Sumera Yasmin sahasar khan 37203-4673615-4 needed Islamabad 70706 1500 SHIFA COLLEGE OF NURSING ISLAMABAD Remarks Centre S.NO. Name Father Name CNIC No. Attempt No DD No Amount Islamabad 4 Abdullah Sultanat Khan 15101-8207671-1 1008908 2000 Islamabad 5 Abdur Rehman Abdul Latif 17301-6589898-7 1st 8031008428 2,000 Mohammad Islamabad 6 Abid Ali 15602-0668939-5 1008908 2000 Ismail Islamabad Ahsan Amir Amir 7 1st 8031008430 2,000 Muhammad Muhammad 38403-3581739-3 Islamabad 8 Anila Anjum Sabab Khan 71402-6658390-6 1st 8031008477 2,000 2nd 9 Anwar Iqbal Sabir Khan 15602-4829339-9 79556 2000 Islamabad attempt Islamabad 10 Aqeel Abbas Allah Ditta 37202-8201118-7 1008908 2000 Islamabad 11 Asif Akbar Fazal Akbar 16202-9802737-3 1008908 2000 Islamabad 12 Asif Gill Younas Gill 38403-7740542-9 1st 8031008420 2,000 Islamabad 13 Atif Mehmood Ishtiaq Ahmad 37201-4030497-5 1008908 2000 Islamabad 14 Barnabass llyas Shaker 36502-2600676-7 1008908 2000 Gul Jehan Islamabad 15 Bilal Ahmad 1st 8031008429 2,000 Said 15705-8233767-7 Islamabad 16 Daniyal Siddiqi Zaheer Siddiqi 61101-5165094-7 1008908 2000 Islamabad 17 Ele Moses Robin Dean 36104-4913461-7 1008908 2000 Islamabad 18 Farah Riasat Riasat Ali 37405-5982626-2 -
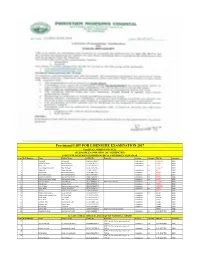
Provisional LIST for LISENSURE EXAMINATION 2017
Provisional LIST FOR LISENSURE EXAMINATION 2017 PAKISTAN NURSING COUNCIL LICENSURE EXAMINATION 2017 GENERIC BSN INSTITUTE OF NURSING KHYBER MEDICAL UNIVERSITY PESHAWAR Sr no Roll Number Name Father Name CNIC No. Remarks Centre Attempt DD No Amount 1 Irfanullah Rahmat Ali 15602-3994101-9 Isalamabad No 15435753 2000 2 Syed Afzal Shah Abdul Ghafoor 17101-1705973-7 Isalamabad 90635 2000 3 Afrooz Bibi Bakht Sherawan 15602-6846449-2 Isalamabad 1st 90636 2000 4 Shazad Aman-E-Room Sher Bahadar 15302-9095234-5 15086719 2000 5 Abbas Ali Khan Badshah 15306-3594812-1 Isalamabad 1st 90577 2000 6 Afzal Akber Muhammad Ishaq 15705-9827246-1 Islamabad 90638 2000 7 Muhammad Ayaz Muhammad Khitab 17301-5471894-1 Islamabad 1st 90575 2000 8 Muhammad Faizan Muhammad Sharif 17301-1655450-1 Islamabad 1st 90579 2000 9 Muhammad Uzair Akhtar Muhammad Akhtar 17301-5064391-1 Islamabad 1st 90576 2000 10 Parveen Akhtar Abdul Ghani 17101-5484531-4 Internship required Islamabad 1212582 2000 11 Riaz Ahmad Ahmad Sahib 15601-3703290-1 Islamabad 1st 90578 2000 12 Siraj-Ul-Haq Muhammad Anwar Shah 15303-9296087-5 Islamabad 15435757 2000 13 Wiqar Ullah Hassan Wali Khan 15701-3952070-7 Islamabad 1st 90573 2000 14 Shaista Muhammad Shah Khan 15605-0565468-6 99637 2000 15 Muhammad Zakaria Fazal Rahman 15302-9139655-5 Islamabad 1st 30729 2000 16 Muhammad Yaseen Khan Yar Min Khan 21201-4177450-5 Islamabad 30686 2000 17 Shah Faisal Taza Khan 21201-7956505-7 Islamabad 30694 2000 18 Shafi Ullah Sher Zada 15602-2637949-5 Islamabad 30687 2000 19 Tasleem Tahir Muhammad Tahir 15101-7887650-4 Islamabad 30690 2000 20 Naseem Bibi Bacha Zada 15101-1230463-0 Islamabad 30688 2000 21 Nusrat Bibi Sulaiman 15101-3072593-2 Islamabad 30689 2000 22 Sehrish Bibi Syed Rehmat Shah 13302-7576063-8 Original Internship required 30707 2000 23 Mumtaz Ali Khan Muhammad Shafiq 15601-0489893-7 Islamabad 1st C-04-2017-702 2000 ALLAMA IQBAL MEDICAL COLLEGE OF NURSING LAHORE S.NO Roll Number Name Father Name CNIC No. -

Stressors Affecting Nursing Students in Pakistan
This is a repository copy of Stressors affecting nursing students in Pakistan. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/121667/ Version: Accepted Version Article: Watson, R., Rehman, S. and Ali, P.A. orcid.org/0000-0002-7839-8130 (2017) Stressors affecting nursing students in Pakistan. International Nursing Review. ISSN 0020-8132 https://doi.org/10.1111/inr.12392 Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Stressors Affecting Nursing Students in Pakistan Professor Roger Watson Professor of Nursing Faculty of Health and Social Care University of Hull Cottingham Raod HU6 7RX Email: [email protected] Ms. Salma Rehman, MScN, RN, RM PhD Candidate Faculty of Health and Social Care University of Hull Cottingham Road Hull HU6 7RX [email protected] Dr. Parveen Azam Ali, PhD, MScN, BScN, FHEA Lecturer The School of Nursing and -

53502-Prospectus UOL.Pdf
PROSPECTUS 2016-17 DISCOVER YOURSELF INSPIRE POSTERITY WELCOME VISION We welcome you all to visit and become part of The University of Lahore aspires to become a nationally the fastest growing private sector multi-discipline and internationally recognized university that distinguishes itself as an imbedding center for outstanding ethical and chartered university of Pakistan. The University moral values, teaching quality, learning outcomes, and of Lahore was established in 1999 and receieved richness of the student experience. The University of Lahore its charter in 2002, since then, it has become the envisions a transformative impact on society through its continual innovation in education, creativity, research, and largest private sector University of Pakistan with entrepreneurship. more than 150 degree programs. The University offers a place for all who have the desire to learn the most contemporary programs available in Pakistan. MISSION The University holds a high international ranking The University of Lahore represents excellence in teaching, with largest international student body from across research, scholarship, creativity, and engagement. Its mission 15 countries. is to produce professionals outfitted with highest standards in creativity, transfer and application of knowledge dissemination to address issues of our time. The UOL sculpts its graduates to become future leaders in their fields to inspire the next generation and to advance ideas that benefit the world. ACCREDITATION Higher Education Commission - HEC Pakistan Engineering Council - PEC Pakistan Medical & Dental Council - PMDC Pakistan Bar Council - PBC Pakistan Nursing Council - PNC Pharmacy Council of Pakistan - PCP Pakistan Council of Architects & Town Planners - PCATP National Computing Education Accreditation Council - NCEAC Find Out More: www.uol.edu.pk National Business Education Accreditation Council - NBEAC Chairman Message Rector Message We know your time at university We take pride in ourselves on being shall make your future. -

Changing Dynamics of Higher Education
ADVERTISEMENT SUPPLEMENT DAWN WEDNESDAY JUNE 13, 2012 01 CHANGING DYNAMICS OF HIGHER EDUCATION Atta-ur-Rahman, FRS Javaid R. Laghari, Chairperson, HEC Pirzada Qasim, VC, Ziauddin University Seema Mughal, VC, Greenwhich University The rapid transformation of China, Korea Universities are the most important produc- Emergence of ‘Knowledge Society’ is per- Failure is not the falling down, but staying and Brazil into robust economies through ers of knowledge, which is the driving force of haps the most significant development of the down. Time and again, nations have turned investments in science, technology and innova- prosperity and contributes to upward econom- twenty first century. All levels of education, their fortunes around by investing in their tion illustrate the new role that universities are ic mobility and increasing the standard of liv- whether global or local are bound to respond to future, by providing higher education to their playing today as engines for socio-economic ing. The modern university, with its mix of this change, with Higher Education sector youth. And now, more than ever, we find our- development. Pakistan has undergone a dra- teaching, innovation and research, is different being no exception. It rather has additional selves at a unique juncture. matic positive change in the higher education sector in the last from the universities of the yesteryears, which only served as responsibility of a catalyst for such changing dynamics that decade. This is illustrated by an increase in university enrol- teaching grounds. -

The Medical Tribunal Act, 2020
REGISTERID No.]4:f92 L.-7G6 9 @cGstdc d $g[fffir EXTRAORDINARY PUBLISHED BY AUTHORITY ISLAMABAD, THURSDAY, Sf,PTf,MBER 24, 202O PART I AcLi, Ordinences, Prcaident's Orders atrd RegulatioDs NATIONAI ASSf, MBLY SECRETARIAT hlanabad, the 2rd Septenber, 2020 No. F. 22(39y20r9-L€gis.-Tho following Act of Majlis-e-Shooro (Parliament) received the assent ofthe Prcsident on the 22nd September, 2020 is hereby published for general information.- AcrNo. XXXIV OF 2020 to provide.for the setting up af specrul j udiciol tribunal to elJicienrly and eryeditiously hear and decide disputcs utising o t of nattcrs prtdining to the medtcal and hcalth seclors WHtRuAs it is €xpedient ro provrde for the serting up for a special judicial Eibunal lo efficicntly and erpcditiously hear and decide disputes arising (635) Ptice. Rs. 10 00 [606i(2020YEx. Caz.l 536 THE GAZET]EOF PAKISTAN, EXTRA., SEPTEMBER 24,2)20 lPARl l ou t of matters p€rt ining to the actions of a uthonties formed to regul are d iffere nt arc&s of the medical sector in Pakistan and to provide cost effoctile rdjudication of such disputes; It is hereby enacted as under: L Short title rnd conmeoc€Eetrt- (I) This Act shall I)e called thc Medical Tribunal Act, 2020. (2) It shall come into forc€ at onca 2. Dcfiritiotrs.- ln this Act, unless there is anlhing repngnant in the subject or context,- (a) sBench" means bench as constituted by thc Chairman ofth€ Mcdical Tribunal: (b) "ChsirmcE" means Chairman ofthe Medical Tri:unall (c) 'membeE" means mernbers of the Medical Tribr nall (d) "pr6cribed" means prescrihd rules o..egulrtions madc underthis Act, as the case may bc; (e) "Ragiltrar" means the rcgistrar of the Medical fribunal anc includes any other person authorized by the 'Irjbunal t( perform the functions ofthe Registrar under this 1\ct: (0 ®ulatioDs" means regulations made under this Act; (g) "rules" means rules made under this Acl; and (h) "Tribunal'means Medical Tribunal established undertiis Act 3. -
Final List 1.Pdf
Pakistan Nursing Council, Islamabad. Exam: Licensing Examination for GBSN Year 2015 Jinnah College of Nursing Karachi S.NO Name Centre Attempt Roll Number Amount . Father Name CNIC No. Remarks No DD NO 1 2015020001 Dilshad Masih B.M Akhtar 34601-1294024-9 Karachi 1st 1235428 2000 2 2015020002 Fayaz Ahmed Hasan Khan 15602-6579227-1 Karachi 1st 9832242 2000 3 2015020003 Fazal Elahi Fazal Subhan 15602-2229336-9 Karachi 1st 10018795 2000 4 2015020004 Ibrar Ul Islam Muhammad Tahir 15705-6769644-5 Karachi 1st 9832243 2000 5 2015020005 Ismail Khan Ali Khan 16101-4594797-9 Islamabad 1st 69785 2000 6 2015020006 Merub Bramuel Brameul Karamat 42301-1522790-4 Karachi 1st 71966 2000 7 2015020007 Naeem George Aslam Awan 42101-6043031-3 Karachi 1st 612590 2000 Obaid Jerald George Walter Karachi 1st 2000 8 2015020008 Timothy Timothy 42201-4350662-7 12436226 9 2015020009 Richard Ejaz Joseph Ejaz 42101-2020642-1 Karachi 1st 69775 2000 10 2015020010 Salman Shah Ibrahim Murad shah 42401-6109800-9 Karachi 1st 65981 2000 11 2015020011 Zakir Ullah Ali Rehman 15601-5490238-7 Islamabad 2nd 69769 2000 Saeeda Waheed College of Nursing S.NO Centre Attempt Roll Number Name Amount . Father Name CNIC No. Remarks No DD No 12 2015020012 Adeela Qayum Abdul Qayyum 32102-4425945-2 Islamabad 2nd 72761 2000 Amna Younis Islamabad 2nd 2000 13 2015020013 Muhammad Younus 35201-5364896 69667 14 2015020014 Beenish Ilyas Ilyas Masih 35202-2679435-6 Islamabad 63394 2000 15 2015020015 Chanda Riaz Riaz Masih 33103-5210961-4 Islamabad 2nd 68449 2000 16 2015020016 Irfana Kausar Mummad -

History of Nursing Education in Pakistan Sarfraz Masih
History of Nursing Education in Pakistan Sarfraz Masih RN, DDC, Post RN BScN, MScN Principal Karachi Kings’ College of Nursing, Karachi Sarfraz Masih, KKCON, Karachi 1 Agenda of Talk History of Nursing Education in Pakistan Prior to partition After partition Developments over the decades Establishment of hospitals and School of Nursing The development of college of nursing federal and provincial University programs for nursing The rise of specialization The role of Pakistan Nursing Council The role of Pakistan Nursing Federation Curriculum revision for Basic Nursing programs Sarfraz Masih, KKCON, Karachi 2 Education Education is a process of providing desirable knowledge and experience to the child (learner) so as to develop his inner powers to the maximum possible extent. (Bassanthappa, 2009) Sarfraz Masih, KKCON, Karachi 3 Education An act or process of imparting or acquiring general knowledge, developing the powers of reasoning and judgment, and generally of preparing oneself or others intellectually for mature life. (http://www.helium.com/knowledge/ 4999-the-definition-of-education) Sarfraz Masih, KKCON, Karachi 4 History of Nursing Education in Pakistan Prior Partition Mostly nurses were English or from other parts of sub-continent Sarfraz Masih, KKCON, Karachi 5 History of Nursing Education in Pakistan After Partition Mostly trained nurses left Pakistan Scarcity of trained nurses from Pakistani population No need of training of nurses Less educated & less paid Recruitment of Christian girls & girls from poor families Nurses are from low socio-economic class Few nursing institutions, e.g. JPMC SON, Karachi Myo Hospital SON, Lahore PNC, 1948 Sarfraz Masih, KKCON, Karachi 6 Developments Over The Decades 1951 – 1960 The Pakistan Nurses Act, 1951 JPMC, CON, 1956 Start of Diploma in Ward Administration and Teaching (combination) at JPMC, CON, in 1956, 1961 – 1970 Diploma in Ward Administration and Teaching Administration separately at JPMC, CON, in 1962 Leading position (Principal) by Pakistani Nurse, 1966 Ms. -

Current Situation and Challenges Concerning Nursing Education in Pakistan T
Nurse Education in Practice 41 (2019) 102638 Contents lists available at ScienceDirect Nurse Education in Practice journal homepage: www.elsevier.com/locate/nepr Guest Editorial Current situation and challenges concerning nursing education in Pakistan T ABSTRACT Despite the advancements in the nursing education and nursing education-based research worldwide, nursing remains an undervalued profession in Pakistan and the nursing education system is steadily evolving. The purpose of this discussion is two-fold: (i) to describe the nursing education system in Pakistan and (ii) to analyze the status, trends, and challenges in nursing education and nursing education-based research in comparison with the international nursing education standards. 1. Introduction visitors, which is offered by 86 institutions, (ii) one-year post basic diploma programs for nurses in specialized areas such as ward admin- Quality nursing education plays a crucial role in strengthening the istration and teaching administration which is offered by 39 nursing healthcare system (World Health Organization, 2015). Excellence in institutions, (iii) a two-year Post RN BSN (awarded to three year di- nursing education is a hallmark of knowledgeable, competent, and ploma holder nurses after two years of additional education), four-year committed nurses who can meet the challenges of complex nursing BSN and two-year Masters in Nursing program (MSN) offered by 62 practice and engage in nursing education-based research (World Health nursing institutions, and (iv) one-year licensed practical nurse program Organization, 2016a). Over the years, there has been considerable de- offered by 26 nursing institutions (Pakistan Nursing Council (PNC), velopment and progress in nursing education worldwide, which has 2017). -
All the Applicants Are Directed to Complete the Deficiences Before Issuing the Roll Numbers I.E. Wednesday 02 November 2016
All the Applicants are directed to complete the deficiences before issuing the Roll numbers i.e. wednesday 02 November 2016. Failure to compliance will lead to drropout from the list . Note: NOT ELIGIBLE candidates are directed to contact their parent institues for further Direction and follow the following link for Licnesure Examination Guidelines http://pnc.org.pk/admin/uploaded/Generic%20BSN%20Licensing%20Examination%20Guideline.pdf Fianl Provisonal List PAKISTAN NURSING COUNCIL LICENSURE EXAMINATION 2016 GENERIC BSN Examination 2016 INSTITUTE OF NURSING KHYBER MEDICAL UNIVERSITY PESHAWAR Sr no Roll Number Name Father Name CNIC No. Remarks Centre Attempt No DD No Amount 1 Hazrat Ali Shah Gul Dad Shah 15101-6773685-7 Islamabad 2nd 205169 2000 2 Ijaz Ali Umar Ali 15402-2011115-9 Islamabad 2nd 205170 2000 3 Nasir Ahmed Kamal Said 15101-7919650-3 Islamabad 2nd 205167 2000 4 Waheed Noor Said Noor 21103-7439768-7 Islamabad 2nd 87686 2000 ALLAMA IQBAL MEDICAL COLLEGE OF NURSING LAHORE Roll Number Name Father Name CNIC No. Remarks Centre Attempt No DD No Amount 5 Aqeela Shaheen Abdul Sattar Shaheen 35101-8076060-2 Islamabad 1st 15283041 2000 6 Asdia Aslam Muhammad Aslm 33100-1406790-0 Islamabad 1st 15133122 2000 7 Benish Imran Tahir Imran 35202-8780207-6 Islamabad 1st 15283891 2000 8 Fouzia Bashir Muhammad Bashir 35202-9279278-0 Islamabad 1st 15283002 2000 9 Hira Iman Tariq Mahmood 35403-7529519-4 Islamabad 2nd 14670312 2000 10 Iqra Adil Muhammad Akram Adil 35202-4028759-6 Islamabad 1st 15904267 2000 11 Iram Nazir Nazir Ahmad 35201-8216225-2 -

Health Reform in Pakistan: a Call to Action
Series Health Transitions in Pakistan 4 Health reform in Pakistan: a call to action Sania Nishtar*, Zulfi qar A Bhutta*, Tazeen H Jafar, Abdul Ghaff ar, Tasleem Akhtar, Kaiser Bengali, Qazi Asmat Isa, Ejaz Rahim Pakistan’s enormous macroeconomic, internal, and human security challenges coexist alongside the opportunity Lancet 2013; 381: 2291–97 created by a huge desire for change. With democracy taking root and a new constitutionally ushered era in state Published Online governance, The Lancet Series about Pakistan and health focuses on health as a nation-building and social-welfare May 17, 2013 agenda at a time of unprecedented social upheaval and economic hardships in the country. We call for a unifi ed vision http://dx.doi.org/10.1016/ S0140-6736(13)60813-2 for the goal of universal and equitable health access. We provide recommendations for six objectives for policy and This is the fourth in a Series of action. Higher political priority for health, increased investments, a combination of targeted and universal approaches, four papers about health action in terms of the social determinants, institutionalisation of the right organisational network, and frameworks transitions in Pakistan for accountability are crucial for the attainment of the health goals in Pakistan. *Joint fi rst authors Heartfi le, Islamabad, Pakistan Introduction cover fi nancial support and the achievement of equity for (S Nishtar PhD); Government of Pakistan is a kaleidoscope of hope and despair, and the country’s diverse population in terms of sex, ethnic Pakistan, Islamabad, Pakistan obscurantism stymying progress, frequently manifest origin, and socioeconomic classes. We recommend six (S Nishtar); Division of Women and Child Health, Aga Khan in the courageous faces of young people who want objectives for policy and action that the federation and University, Karachi, Pakistan change. -

NURSING EDUCATION Bscn
CURRICULUM OF NURSING EDUCATION BScN (Revised 2006) HIG ISSION HER OMM EDUCATION C HIGHER EDUCATION COMMISSION ISLAMABAD & PAKISTAN NURSING COUNCIL ISLAMABAD 1 CURRICULUM DIVISION, HEC Prof. Dr. Syed Altaf Hussain Former Member (Acad/R&D) Prof. Dr. Altaf Ali G. Shaikh Former Adviser (Acad/R&D) Malik Ghulam Abbas Deputy Director Miss Ghayyur Fatima Deputy Director (Curri) Mr. M. Tahir Ali Shah Assistant Director Mr. Shafiullah Khan Assistant Director Composed by Mr. Zulfiqar Ali, HEC Islamabad 2 CONTENTS 1. Foreword by Registrar PNC 6 2. Background 7 3. Introduction 8 4. Curriculum for BScN 13 i) Rational 13 ii) Philosophy 15 iii) Framework for BScN Program 25 5. Course Outline 28 i) Year-1 a) Semester-1 28 b) Semester-2 54 ii) Year-2 a) Semester-3 91 b) Semester-4 126 iii) Year-3 a) Semester-5 162 b) Semester-6 210 iv) Year-4 a) Semester-7 238 b) Semester-8 267 6. General Recommendations 292 3 PREFACE Curriculum of a subject is said to be the throbbing pulse of a nation. By looking at the curriculum one can judge the state of intellectual development and the state of progress of the nation. The world has turned into a global village; new ideas and information are pouring in like a stream. It is, therefore, imperative to update our curricula regularly by introducing the recent developments in the relevant fields of knowledge. In exercise of the powers conferred by sub-section (1) of section 3 of the Federal Supervision of Curricula Textbooks and Maintenance of Standards of Education Act 1976, the Federal Government vide notification no.