Kerion Celsi Caused by Microsporum Gypseum: Report of Two Cases and Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fungal Infections from Human and Animal Contact
Journal of Patient-Centered Research and Reviews Volume 4 Issue 2 Article 4 4-25-2017 Fungal Infections From Human and Animal Contact Dennis J. Baumgardner Follow this and additional works at: https://aurora.org/jpcrr Part of the Bacterial Infections and Mycoses Commons, Infectious Disease Commons, and the Skin and Connective Tissue Diseases Commons Recommended Citation Baumgardner DJ. Fungal infections from human and animal contact. J Patient Cent Res Rev. 2017;4:78-89. doi: 10.17294/2330-0698.1418 Published quarterly by Midwest-based health system Advocate Aurora Health and indexed in PubMed Central, the Journal of Patient-Centered Research and Reviews (JPCRR) is an open access, peer-reviewed medical journal focused on disseminating scholarly works devoted to improving patient-centered care practices, health outcomes, and the patient experience. REVIEW Fungal Infections From Human and Animal Contact Dennis J. Baumgardner, MD Aurora University of Wisconsin Medical Group, Aurora Health Care, Milwaukee, WI; Department of Family Medicine and Community Health, University of Wisconsin School of Medicine and Public Health, Madison, WI; Center for Urban Population Health, Milwaukee, WI Abstract Fungal infections in humans resulting from human or animal contact are relatively uncommon, but they include a significant proportion of dermatophyte infections. Some of the most commonly encountered diseases of the integument are dermatomycoses. Human or animal contact may be the source of all types of tinea infections, occasional candidal infections, and some other types of superficial or deep fungal infections. This narrative review focuses on the epidemiology, clinical features, diagnosis and treatment of anthropophilic dermatophyte infections primarily found in North America. -

Estimated Burden of Fungal Infections in Oman
Journal of Fungi Article Estimated Burden of Fungal Infections in Oman Abdullah M. S. Al-Hatmi 1,2,3,* , Mohammed A. Al-Shuhoumi 4 and David W. Denning 5 1 Department of microbiology, Natural & Medical Sciences Research Center, University of Nizwa, Nizwa 616, Oman 2 Department of microbiology, Centre of Expertise in Mycology Radboudumc/CWZ, 6500 Nijmegen, The Netherlands 3 Foundation of Atlas of Clinical Fungi, 1214GP Hilversum, The Netherlands 4 Ibri Hospital, Ministry of Health, Ibri 115, Oman; [email protected] 5 Manchester Fungal Infection Group, Manchester Academic Health Science Centre, The University of Manchester, Manchester M13 9PL, UK; [email protected] * Correspondence: [email protected]; Tel.: +968-25446328; Fax: +968-25446612 Abstract: For many years, fungi have emerged as significant and frequent opportunistic pathogens and nosocomial infections in many different populations at risk. Fungal infections include disease that varies from superficial to disseminated infections which are often fatal. No fungal disease is reportable in Oman. Many cases are admitted with underlying pathology, and fungal infection is often not documented. The burden of fungal infections in Oman is still unknown. Using disease frequencies from heterogeneous and robust data sources, we provide an estimation of the incidence and prevalence of Oman’s fungal diseases. An estimated 79,520 people in Oman are affected by a serious fungal infection each year, 1.7% of the population, not including fungal skin infections, chronic fungal rhinosinusitis or otitis externa. These figures are dominated by vaginal candidiasis, followed by allergic respiratory disease (fungal asthma). An estimated 244 patients develop invasive aspergillosis and at least 230 candidemia annually (5.4 and 5.0 per 100,000). -

Effect of Rutaceae Plant's Essential Oils and Leaf Extracts on Dermatophytic Fungal Cell Morphology
Effect of Rutaceae plant’s essential oils and leaf extracts on dermatophytic fungal cell morphology: a hope for the development of an effective antifungal from natural origin Submitted in fulfillment of the academic requirements for the degree of DOCTOR OF PHILOSOPHY By OLUFUNKE OMOWUMI FAJINMI Research Centre for Plant Growth and Development School of Life Sciences College of Agriculture, Engineering and Science University of KwaZulu-Natal, Pietermaritzburg May 2016 Pictures sourced from google A healthy, glowing, beautiful skin….the pride of every woman i . Table of Contents STUDENT DECLARATION ................................................................................................... v DECLARATION BY SUPERVISORS ....................................................................................... vi COLLEGE OF AGRICULTURE ENGINEERING & SCIENCE DECLARATION 1- PLAGIARISM ........ vii ACKNOWLEDGEMENTS .................................................................................................. viii COLLEGE OF AGRICULTURE ENGINEERING & SCIENCE DECLARATION 2- PUBLICATIONS ....... x LIST OF FIGURES .............................................................................................................. xi LIST OF TABLES ............................................................................................................... xii LIST OF ABBREVIATIONS ................................................................................................ xiv ABSTRACT ..................................................................................................................... -

Tinea Capitis 2014 L.C
BJD GUIDELINES British Journal of Dermatology British Association of Dermatologists’ guidelines for the management of tinea capitis 2014 L.C. Fuller,1 R.C. Barton,2 M.F. Mohd Mustapa,3 L.E. Proudfoot,4 S.P. Punjabi5 and E.M. Higgins6 1Department of Dermatology, Chelsea & Westminster Hospital, Fulham Road, London SW10 9NH, U.K. 2Department of Microbiology, Leeds General Infirmary, Leeds LS1 3EX, U.K. 3British Association of Dermatologists, Willan House, 4 Fitzroy Square, London W1T 5HQ, U.K. 4St John’s Institute of Dermatology, Guy’s and St Thomas’ NHS Foundation Trust, St Thomas’ Hospital, Westminster Bridge Road, London SE1 7EH, U.K. 5Department of Dermatology, Hammersmith Hospital, 150 Du Cane Road, London W12 0HS, U.K. 6Department of Dermatology, King’s College Hospital, Denmark Hill, London SE5 9RS, U.K. 1.0 Purpose and scope Correspondence Claire Fuller. The overall objective of this guideline is to provide up-to- E-mail: [email protected] date, evidence-based recommendations for the management of tinea capitis. This document aims to update and expand Accepted for publication on the previous guidelines by (i) offering an appraisal of 8 June 2014 all relevant literature since January 1999, focusing on any key developments; (ii) addressing important, practical clini- Funding sources cal questions relating to the primary guideline objective, i.e. None. accurate diagnosis and identification of cases; suitable treat- ment to minimize duration of disease, discomfort and scar- Conflicts of interest ring; and limiting spread among other members of the L.C.F. has received sponsorship to attend conferences from Almirall, Janssen and LEO Pharma (nonspecific); has acted as a consultant for Alliance Pharma (nonspe- community; (iii) providing guideline recommendations and, cific); and has legal representation for L’Oreal U.K. -

Therapies for Common Cutaneous Fungal Infections
MedicineToday 2014; 15(6): 35-47 PEER REVIEWED FEATURE 2 CPD POINTS Therapies for common cutaneous fungal infections KENG-EE THAI MB BS(Hons), BMedSci(Hons), FACD Key points A practical approach to the diagnosis and treatment of common fungal • Fungal infection should infections of the skin and hair is provided. Topical antifungal therapies always be in the differential are effective and usually used as first-line therapy, with oral antifungals diagnosis of any scaly rash. being saved for recalcitrant infections. Treatment should be for several • Topical antifungal agents are typically adequate treatment weeks at least. for simple tinea. • Oral antifungal therapy may inea and yeast infections are among the dermatophytoses (tinea) and yeast infections be required for extensive most common diagnoses found in general and their differential diagnoses and treatments disease, fungal folliculitis and practice and dermatology. Although are then discussed (Table). tinea involving the face, hair- antifungal therapies are effective in these bearing areas, palms and T infections, an accurate diagnosis is required to ANTIFUNGAL THERAPIES soles. avoid misuse of these or other topical agents. Topical antifungal preparations are the most • Tinea should be suspected if Furthermore, subsequent active prevention is commonly prescribed agents for dermatomy- there is unilateral hand just as important as the initial treatment of the coses, with systemic agents being used for dermatitis and rash on both fungal infection. complex, widespread tinea or when topical agents feet – ‘one hand and two feet’ This article provides a practical approach fail for tinea or yeast infections. The pharmacol- involvement. to antifungal therapy for common fungal infec- ogy of the systemic agents is discussed first here. -

Diversity of Geophilic Dermatophytes Species in the Soils of Iran; the Significant Preponderance of Nannizzia Fulva
Journal of Fungi Article Diversity of Geophilic Dermatophytes Species in the Soils of Iran; The Significant Preponderance of Nannizzia fulva Simin Taghipour 1, Mahdi Abastabar 2, Fahimeh Piri 3, Elham Aboualigalehdari 4, Mohammad Reza Jabbari 2, Hossein Zarrinfar 5 , Sadegh Nouripour-Sisakht 6, Rasoul Mohammadi 7, Bahram Ahmadi 8, Saham Ansari 9, Farzad Katiraee 10 , Farhad Niknejad 11 , Mojtaba Didehdar 12, Mehdi Nazeri 13, Koichi Makimura 14 and Ali Rezaei-Matehkolaei 3,4,* 1 Department of Medical Parasitology and Mycology, Faculty of Medicine, Shahrekord University of Medical Sciences, Shahrekord 88157-13471, Iran; [email protected] 2 Invasive Fungi Research Center, Department of Medical Mycology and Parasitology, School of Medicine, Mazandaran University of Medical Sciences, Sari 48157-33971, Iran; [email protected] (M.A.); [email protected] (M.R.J.) 3 Infectious and Tropical Diseases Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz 61357-15794, Iran; [email protected] 4 Department of Medical Mycology, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz 61357-15794, Iran; [email protected] 5 Allergy Research Center, Mashhad University of Medical Sciences, Mashhad 91766-99199, Iran; [email protected] 6 Medicinal Plants Research Center, Yasuj University of Medical Sciences, Yasuj 75919-94799, Iran; [email protected] Citation: Taghipour, S.; Abastabar, M.; 7 Department of Medical Parasitology and Mycology, School of Medicine, Infectious Diseases and Tropical Piri, F.; Aboualigalehdari, E.; Jabbari, Medicine Research Center, Isfahan University of Medical Sciences, Isfahan 81746-73461, Iran; M.R.; Zarrinfar, H.; Nouripour-Sisakht, [email protected] 8 S.; Mohammadi, R.; Ahmadi, B.; Department of Medical Laboratory Sciences, Faculty of Paramedical, Bushehr University of Medical Sciences, Bushehr 75187-59577, Iran; [email protected] Ansari, S.; et al. -
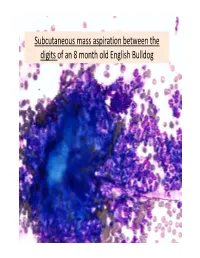
Subcutaneous Mass Aspiration Between the Digits of an 8 Month Old English Bulldog Marked Inflammation: Neutrophils & Macrophages
Subcutaneous mass aspiration between the digits of an 8 month old English Bulldog Marked inflammation: neutrophils & macrophages Hair fragment Macrophages What is this structure? Degenerate Neutrophils Abundant amount of keratin with similar structures The structures are ~ 2‐3 micron in size, blue to occasionally dark purple, oval to round in shape and have a thin clear capsule, consistent with fungal organisms The fungi are seen also in neutrophils and free in the background Growth of Microsporum canis was diagnosed on fungal culture • Microsporum canis is a dermatophyte that frequently causes infection of the superficial layers of skin, hair and nails (dermtophytoses). 1,2 • Microsporum canis, Microsporum gypseum and Trichophyton mentagrophytes are the main etiologic agents of clinical dermatophytosis. 3 • Dermatophytes affect the hair shafts, stratum corneum and nails or claws of animals and people. 2 • The typical lesions include focal alopecia, broken hair shafts, crusts scales and erythema on the head, feet and tail of dogs and cats. 1 • The structures seen in this cytology were Microsporum arthroconidia, which should be differentiated from other similar fungal yeast bodies seen in Candidiasis, Histoplasmosis, Aspergillosis/Penicillosis and Sporotrichosis. 2,4 Kerion • Less commonly dermatophytosis causes raised or dermal nodules called kerions or nodular dermatophytosis. 1,3 • These lesions are formed when the infected hair follicle ruptures and both the fungi and keratin spill in the dermis eliciting an intense inflammatory response. 1 • This may develop in any species but is most commonly reported in dogs. 3 • M. canis is the most common cause of kerion in dogs. 3 • Most common locations were the head, neck and limbs. -

Geophilic Dermatophytes and Other Keratinophilic Fungi in the Nests of Wetland Birds
ACTA MyCoLoGICA Vol. 46 (1): 83–107 2011 Geophilic dermatophytes and other keratinophilic fungi in the nests of wetland birds Teresa KoRnIŁŁoWICz-Kowalska1, IGnacy KIToWSKI2 and HELEnA IGLIK1 1Department of Environmental Microbiology, Mycological Laboratory University of Life Sciences in Lublin Leszczyńskiego 7, PL-20-069 Lublin, [email protected] 2Department of zoology, University of Life Sciences in Lublin, Akademicka 13 PL-20-950 Lublin, [email protected] Korniłłowicz-Kowalska T., Kitowski I., Iglik H.: Geophilic dermatophytes and other keratinophilic fungi in the nests of wetland birds. Acta Mycol. 46 (1): 83–107, 2011. The frequency and species diversity of keratinophilic fungi in 38 nests of nine species of wetland birds were examined. nine species of geophilic dermatophytes and 13 Chrysosporium species were recorded. Ch. keratinophilum, which together with its teleomorph (Aphanoascus fulvescens) represented 53% of the keratinolytic mycobiota of the nests, was the most frequently observed species. Chrysosporium tropicum, Trichophyton terrestre and Microsporum gypseum populations were less widespread. The distribution of individual populations was not uniform and depended on physical and chemical properties of the nests (humidity, pH). Key words: Ascomycota, mitosporic fungi, Chrysosporium, occurrence, distribution INTRODUCTION Geophilic dermatophytes and species representing the Chrysosporium group (an arbitrary term) related to them are ecologically classified as keratinophilic fungi. Ke- ratinophilic fungi colonise keratin matter (feathers, hair, etc., animal remains) in the soil, on soil surface and in other natural environments. They are keratinolytic fungi physiologically specialised in decomposing native keratin. They fully solubilise na- tive keratin (chicken feathers) used as the only source of carbon and energy in liquid cultures after 70 to 126 days of growth (20°C) (Korniłłowicz-Kowalska 1997). -

Therapies for Common Cutaneous Fungal Infections
MedicineToday 2014; 15(6): 35-47 PEER REVIEWED FEATURE 2 CPD POINTS Therapies for common cutaneous fungal infections KENG-EE THAI MB BS(Hons), BMedSci(Hons), FACD Key points A practical approach to the diagnosis and treatment of common fungal • Fungal infection should infections of the skin and hair is provided. Topical antifungal therapies always be in the differential are effective and usually used as first-line therapy, with oral antifungals diagnosis of any scaly rash. being saved for recalcitrant infections. Treatment should be for several • Topical antifungal agents are typically adequate treatment weeks at least. for simple tinea. • Oral antifungal therapy may inea and yeast infections are among the dermatophytoses (tinea) and yeast infections be required for extensive most common diagnoses found in general and their differential diagnoses and treatments disease, fungal folliculitis and practice and dermatology. Although are then discussed (Table). tinea involving the face, hair- antifungal therapies are effective in these bearing areas, palms and T infections, an accurate diagnosis is required to ANTIFUNGAL THERAPIES soles. avoid misuse of these or other topical agents. Topical antifungal preparations are the most • Tinea should be suspected if Furthermore, subsequent active prevention is commonly prescribed agents for dermatomy- there is unilateral hand just as important as the initial treatment of the coses, with systemic agents being used for dermatitis and rash on both fungal infection. complex, widespread tinea or when topical agents feet – ‘one hand and two feet’ This article provides a practical approach fail for tinea or yeast infections. The pharmacol- involvement. to antifungal therapy for common fungal infec- ogy of the systemic agents is discussed first here. -
Tinea Capitis: Current Concepts in Clinical Practice
CONTINUING MEDICAL EDUCATION Tinea Capitis: Current Concepts in Clinical Practice Matthew J. Trovato, MD; Robert A. Schwartz, MD, MPH; Camila K. Janniger, MD GOAL To understand tinea capitis to better treat patients with the condition OBJECTIVES Upon completion of this activity, dermatologists and general practitioners should be able to: 1. Describe the etiology of tinea capitis. 2. Recognize and diagnose tinea capitis. 3. Effectively treat tinea capitis. CME Test on page 88. This article has been peer reviewed and is accredited by the ACCME to provide continuing approved by Victor B. Hatcher, PhD, Professor of medical education for physicians. Medicine, Albert Einstein College of Medicine. Albert Einstein College of Medicine designates Review date: January 2006. this educational activity for a maximum of 1 This activity has been planned and implemented category 1 credit toward the AMA Physician’s in accordance with the Essential Areas and Policies Recognition Award. Each physician should of the Accreditation Council for Continuing Medical claim only that credit that he/she actually spent Education through the joint sponsorship of Albert in the activity. Einstein College of Medicine and Quadrant This activity has been planned and produced in HealthCom, Inc. Albert Einstein College of Medicine accordance with ACCME Essentials. Drs. Trovato, Schwartz, and Janniger report no conflict of interest. The authors discuss off-label use of fluconazole, itraconazole, ketoconazole, and terbinafine. Dr. Hatcher reports no conflict of interest. Tinea capitis is a common infection, particularly seen in Europe and many other countries, which among young children in urban regions. The emit a green fluorescence. However, T tonsurans, infection often is seen in a form with mild scaling like other fungi, also may less often produce an and little hair loss, a result of the prominence of intense inflammatory reaction, which is sugges- Trichophyton tonsurans (the most frequent cause tive of an acute bacterial infection. -

STUDIES on INVASIVE KERATINOPHILIC DERMATOPHYTES of HUMAN HAIR *Brajesh Kumar Jha1, S
Brajesh et al Journal of Drug Delivery & Therapeutics; 2013, 3(2), 70-74 70 Available online at http://jddtonline.info RESEARCH ARTICLE STUDIES ON INVASIVE KERATINOPHILIC DERMATOPHYTES OF HUMAN HAIR *Brajesh Kumar Jha1, S. Mahadeva Murthy2 1Research Scholar, Department of Microbiology, Yubraja College, Mysore, India 2Associate Professor, Department of Microbiology, Yubraja College, Mysore, India *Corresponding Author’s Email: [email protected] Phone: +977- 9845087892 ABSTRACT: Background: Tinea Capitis (TC) is a dermatophyte infection of the scalp hair follicles and intervening skin. TC is mainly caused by anthropohilic and zoophilic species of the genera Trichophyton and Microsporum. On the basis of the type of hair invasion, dermatophytes are also classified as endothrix, ectothrix or favus. Despite the availability of effective antifungal agents, dermatophytic infections continue to be one of the principal dermatological diseases in Mysore. Objectives: To study the genus and species variants, of fungus causing Tinea Capitis infection and epidemiological factors responsible for the disease in Central Mysore. Materials and methods: Clinically suspected 527 patients with dermatophytes infection cases were included in our study, where 58 cases were diagnosed and confirmed as a Tinea Capitis patients only selected for our study. Suspected lesion like scalp skin scraping and hair plucking samples were collected after disinfecting the site with 70% of ethyl alcohol. Samples were collected in a sterile thick black envelope, folded, labelled and brought to the laboratory for further processing according to slandered Mycological protocol. Results: A total of 527 patients with dermatophytes infection suspected cases were included in our study, where 58 cases (11.0%) were confirmed as a Tinea Capitis. -

Vulvar Majocchi Granuloma and Kerion Formation in an Immunocompetent Female
Volume 25 Number 9| September 2019| Dermatology Online Journal || Case Presentation 25(9):7 Vulvar Majocchi granuloma and kerion formation in an immunocompetent female Jessica G Labadie MD, Lauren M Guggina MD Affiliations: Department of Dermatology, Northwestern University Feinberg School of Medicine, 676 North St. Clair Street, Suite 1600, Chicago, Illinois, USA Corresponding Author: Jessica G. Labadie MD, 676 North St. Clair Street, Suite 1600, Chicago, IL 60611, Email: [email protected] vulva, noted after shaving with a razor. Initial Abstract treatment by the primary physician included two- We report a rare case of vulvar Majocchi granuloma weeks of systemic antifungal therapy, followed by a and kerion formation secondary to Trichophyton in an course of oral steroids, and oral metronidazole, immunocompetent woman. The patient responded which offered minimal relief. well to oral terbinafine and a short course of oral corticosteroids with a slow taper. Resolution of deep On initial examination in our clinic, the inguinal dermatophytosis requires prompt pathogen creases had scattered annular plaques studded with identification and treatment to avoid scarring and small 1-2mm pustules and the suprapubic area hair loss. Herein, we aim to increase clinical exhibited indurated perifollicular papules (Figure awareness and early recognition of this atypical 1A). Notably, her hands, feet, and nails were clear of presentation of a Majocchi granuloma with kerion abnormality. Initial punch biopsy revealed septate formation. hyphal forms in the stratum corneum and subcorneal pustules (Figure 1B). Hyphae were Keywords: kerion, Majocchi granuloma, vulva confirmed by DPAS and biopsy was consistent with tinea corporis. A superficial fungal culture was positive for Trichophyton species.