Scholars Journal of Medical Case Reports
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Effect of Rutaceae Plant's Essential Oils and Leaf Extracts on Dermatophytic Fungal Cell Morphology
Effect of Rutaceae plant’s essential oils and leaf extracts on dermatophytic fungal cell morphology: a hope for the development of an effective antifungal from natural origin Submitted in fulfillment of the academic requirements for the degree of DOCTOR OF PHILOSOPHY By OLUFUNKE OMOWUMI FAJINMI Research Centre for Plant Growth and Development School of Life Sciences College of Agriculture, Engineering and Science University of KwaZulu-Natal, Pietermaritzburg May 2016 Pictures sourced from google A healthy, glowing, beautiful skin….the pride of every woman i . Table of Contents STUDENT DECLARATION ................................................................................................... v DECLARATION BY SUPERVISORS ....................................................................................... vi COLLEGE OF AGRICULTURE ENGINEERING & SCIENCE DECLARATION 1- PLAGIARISM ........ vii ACKNOWLEDGEMENTS .................................................................................................. viii COLLEGE OF AGRICULTURE ENGINEERING & SCIENCE DECLARATION 2- PUBLICATIONS ....... x LIST OF FIGURES .............................................................................................................. xi LIST OF TABLES ............................................................................................................... xii LIST OF ABBREVIATIONS ................................................................................................ xiv ABSTRACT ..................................................................................................................... -

Diversity of Geophilic Dermatophytes Species in the Soils of Iran; the Significant Preponderance of Nannizzia Fulva
Journal of Fungi Article Diversity of Geophilic Dermatophytes Species in the Soils of Iran; The Significant Preponderance of Nannizzia fulva Simin Taghipour 1, Mahdi Abastabar 2, Fahimeh Piri 3, Elham Aboualigalehdari 4, Mohammad Reza Jabbari 2, Hossein Zarrinfar 5 , Sadegh Nouripour-Sisakht 6, Rasoul Mohammadi 7, Bahram Ahmadi 8, Saham Ansari 9, Farzad Katiraee 10 , Farhad Niknejad 11 , Mojtaba Didehdar 12, Mehdi Nazeri 13, Koichi Makimura 14 and Ali Rezaei-Matehkolaei 3,4,* 1 Department of Medical Parasitology and Mycology, Faculty of Medicine, Shahrekord University of Medical Sciences, Shahrekord 88157-13471, Iran; [email protected] 2 Invasive Fungi Research Center, Department of Medical Mycology and Parasitology, School of Medicine, Mazandaran University of Medical Sciences, Sari 48157-33971, Iran; [email protected] (M.A.); [email protected] (M.R.J.) 3 Infectious and Tropical Diseases Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz 61357-15794, Iran; [email protected] 4 Department of Medical Mycology, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz 61357-15794, Iran; [email protected] 5 Allergy Research Center, Mashhad University of Medical Sciences, Mashhad 91766-99199, Iran; [email protected] 6 Medicinal Plants Research Center, Yasuj University of Medical Sciences, Yasuj 75919-94799, Iran; [email protected] Citation: Taghipour, S.; Abastabar, M.; 7 Department of Medical Parasitology and Mycology, School of Medicine, Infectious Diseases and Tropical Piri, F.; Aboualigalehdari, E.; Jabbari, Medicine Research Center, Isfahan University of Medical Sciences, Isfahan 81746-73461, Iran; M.R.; Zarrinfar, H.; Nouripour-Sisakht, [email protected] 8 S.; Mohammadi, R.; Ahmadi, B.; Department of Medical Laboratory Sciences, Faculty of Paramedical, Bushehr University of Medical Sciences, Bushehr 75187-59577, Iran; [email protected] Ansari, S.; et al. -

Geophilic Dermatophytes and Other Keratinophilic Fungi in the Nests of Wetland Birds
ACTA MyCoLoGICA Vol. 46 (1): 83–107 2011 Geophilic dermatophytes and other keratinophilic fungi in the nests of wetland birds Teresa KoRnIŁŁoWICz-Kowalska1, IGnacy KIToWSKI2 and HELEnA IGLIK1 1Department of Environmental Microbiology, Mycological Laboratory University of Life Sciences in Lublin Leszczyńskiego 7, PL-20-069 Lublin, [email protected] 2Department of zoology, University of Life Sciences in Lublin, Akademicka 13 PL-20-950 Lublin, [email protected] Korniłłowicz-Kowalska T., Kitowski I., Iglik H.: Geophilic dermatophytes and other keratinophilic fungi in the nests of wetland birds. Acta Mycol. 46 (1): 83–107, 2011. The frequency and species diversity of keratinophilic fungi in 38 nests of nine species of wetland birds were examined. nine species of geophilic dermatophytes and 13 Chrysosporium species were recorded. Ch. keratinophilum, which together with its teleomorph (Aphanoascus fulvescens) represented 53% of the keratinolytic mycobiota of the nests, was the most frequently observed species. Chrysosporium tropicum, Trichophyton terrestre and Microsporum gypseum populations were less widespread. The distribution of individual populations was not uniform and depended on physical and chemical properties of the nests (humidity, pH). Key words: Ascomycota, mitosporic fungi, Chrysosporium, occurrence, distribution INTRODUCTION Geophilic dermatophytes and species representing the Chrysosporium group (an arbitrary term) related to them are ecologically classified as keratinophilic fungi. Ke- ratinophilic fungi colonise keratin matter (feathers, hair, etc., animal remains) in the soil, on soil surface and in other natural environments. They are keratinolytic fungi physiologically specialised in decomposing native keratin. They fully solubilise na- tive keratin (chicken feathers) used as the only source of carbon and energy in liquid cultures after 70 to 126 days of growth (20°C) (Korniłłowicz-Kowalska 1997). -

Antifungal Susceptibility of Japanese Isolates of Nannizia Fulva (Formerly Microsporum Fulvum)
Med. Mycol. J. Vol.Med. 60, Mycol.23-25, 2019 J. Vol. 60 (No. 1) , 2019 23 ISSN 2185-6486 Short Report Antifungal Susceptibility of Japanese Isolates of Nannizia fulva (Formerly Microsporum fulvum) Rui Kano1, Karin Oshimo1, Teru Fukutomi2 and Hiroshi Kamata1 1 Department of Veterinary Pathobiology, Nihon University College of Bioresouce Sciences School of Veterinary Medicine 2 Bright Pet Clinic ABSTRACT Human and animal dermatophytoses are most commonly treated with systemic antifungal drugs such as itraconazole (ITZ) and terbinafine (TRF). The antifungal susceptibility of Nannizia fulva, however, remains poorly documented. In the present study, we investigated the in vitro susceptibility of N. fulva to ITZ and TRFusing the CLSI M38-A2 test. The mean MICs for the 12 tested strains were 0.6542 mg/L (range: 0.0625-1 mg/L) for ITZ and 0.15625 mg/L (range: < 0.003125-0.5 mg/L) for TRF. These results indicate that ITZ and TRFat standard veterinary doses should be efficacious against N. fulva. Key words : Antifungal susceptibility, geophilic dermatophyte, itraconazole, Nannizia fulva, terbinafine Members of the Microsporum gypseum complex are (Table 1). geophilic dermatophytes with worldwide distribution and The isolates of N. fulva examined in this study are listed in occasionally have been isolated as infectious agents in humans Table 1. These isolates were obtained from normal rabbit hair and animals1-3). The teleomorphs of the complex consist of and soils in rabbit hutches in public primary schools in Nannizia fulva (formerly Microsporum fulvum and Yokohama, Japan6). Arthroderma fulvum), N. gypsea,andNannizia. incurvata1, 4). The isolates were maintained on diluted Sabouraud’s In 1982, Hironaga et al. -

The New Species Concept in Dermatophytes—A Polyphasic Approach
Mycopathologia DOI 10.1007/s11046-008-9099-y The New Species Concept in Dermatophytes—a Polyphasic Approach Yvonne Gra¨ser Æ James Scott Æ Richard Summerbell Received: 15 October 2007 / Accepted: 30 January 2008 Ó Springer Science+Business Media B.V. 2008 Abstract The dermatophytes are among the most among these are the cosmopolitan bane of nails and frequently observed organisms in biomedicine, yet feet, Trichophyton rubrum, and the endemic African there has never been stability in the taxonomy, agent of childhood tinea capitis, Trichophyton identification and naming of the approximately 25 soudanense, which are effectively inseparable in all pathogenic species involved. Since the identification analyses. The molecular data require some reinter- of these species is often epidemiologically and pretation of results seen in conventional phenotypic ethically important, the difficulties in dermatophyte tests, but in most cases, phylogenetic insight is identification are a fruitful topic for modern molec- readily integrated with current laboratory testing ular biological investigation, done in tandem with procedures. renewed investigation of phenotypic characters. Molecular phylogenetic analyses such as multilocus Keywords Dermatophytes Á Taxonomy Á sequence typing have had to be tailored to accom- Molecular identification Á modate differing the mechanisms of speciation that Morphological identification Á Species concept have produced the dermatophytes that are commonly seen today. Even so, some biotypes that were unambiguously considered species in the past, based Introduction: Why Dermatophyte Biosystematics on profound differences in morphology and pattern of and Identification are Important (Medical infection, appear consistently not to be distinct and Scientific Aspects) species in modern molecular analyses. Most notable The dermatophytes belong to the small category of disease organisms that almost every human alive will Y. -

How Much Human Ringworm Is Zoophilic? Mcphee A, Cherian S, Robson J Adapted from Poster Produced for the Zoonoses Conference 25–26 July 2014 Brisbane
How much human ringworm is zoophilic? McPhee A, Cherian S, Robson J Adapted from poster produced for the Zoonoses Conference 25–26 July 2014 Brisbane Introduction Epidermophyton floccosum Humans Common Dermatophytes can be the cause of common infections in both Trichophyton rubrum [worldwide] Humans Very common humans and animals. The source of human infection may be Trichophyton rubrum [African] Humans Less common anthropophilic (human), geophilic (soil) or zoophilic (animal). Trichophyton interdigitale Anthropophilic Humans Common Zoophilic dermatophyte infections usually elicit a strong host [anthropophilic] response on the skin where there is contact with the infective Trichophyton tonsurans Humans Common animal or contaminated fomites. Table 1 illustrates the range of Trichophyton violaceum Humans Less common dermatophytes that are isolated from the mycology laboratory Microsporum audouinii Humans Less common and grouped by source of acquisition. Microsporum gypseum Soil Common Geophilic Microsporum nanum Soil/Pigs Rare Guinea pigs, Aim Trichophyton interdigitale [zoophilic] Common kangaroos To characterize and compare zoophilic with non-zoophilic Microsporum canis Cats Common dermatophyte human infections isolated at Sullivan Nicolaides Zoophilic Trichophyton verrucosum Cattle Rare Pathology (SNP) for the year 2013. Trichophyton equinum Horses Rare Microsporum nanum Soil/pigs Rare Method Table 1: Classification of dermatophytes according to source Superficial fungal cultures submitted in 2013 to Sullivan Nicolaides Pathology were reviewed. This laboratory services Queensland and extends into New South Wales as far south as Coffs Harbour. Specimens include skin scrapings, skin biopsies, nails and involved hair. All cutaneous samples (Figure 1) submitted for fungal culture receive direct examination using Calcofluor white/Evans Blue/ KOH/Glycerol under fluorescent and/or light microscopy (Figure 2) and cultured. -

Phylogeny of Dermatophytes with Genomic Character Evaluation of Clinically Distinct Trichophyton Rubrum and T
available online at www.studiesinmycology.org STUDIES IN MYCOLOGY 89: 153–175 (2018). Phylogeny of dermatophytes with genomic character evaluation of clinically distinct Trichophyton rubrum and T. violaceum P. Zhan1,2,3,4, K. Dukik3,4,D.Li1,5, J. Sun6, J.B. Stielow3,8,9, B. Gerrits van den Ende3, B. Brankovics3,4, S.B.J. Menken4, H. Mei1,W.Bao7,G.Lv1,W.Liu1*, and G.S. de Hoog3,4,8,9* 1Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College, Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, Nanjing, China; 2Dermatology Hospital of Jiangxi Provinces, Jiangxi Dermatology Institute, Nanchang, China; 3Westerdijk Fungal Biodiversity Institute, Utrecht, The Netherlands; 4Institute of Biodiversity and Ecosystem Dynamics, University of Amsterdam, Amsterdam, The Netherlands; 5Georgetown University Medical Center, Department of Microbiology and Immunology, Washington, DC, USA; 6Guangdong Provincial Institute of Public Health, Guangdong Provincial Center for Disease Control and Prevention, Guangzhou, China; 7Nanjing General Hospital of Nanjing Command, Nanjing, China; 8Thermo Fisher Scientific, Landsmeer, The Netherlands; 9Center of Expertise in Mycology of Radboudumc/Canisius Wilhelmina Hospital, Nijmegen, The Netherlands *Correspondence: W. Liu, [email protected]; G.S. de Hoog, [email protected] Abstract: Trichophyton rubrum and T. violaceum are prevalent agents of human dermatophyte infections, the former being found on glabrous skin and nail, while the latter is confined to the scalp. The two species are phenotypically different but are highly similar phylogenetically. The taxonomy of dermatophytes is currently being reconsidered on the basis of molecular phylogeny. Molecular species definitions do not always coincide with existing concepts which are guided by ecological and clinical principles. -

Dermatophytosis Caused by Microsporum Gypseum in Infants: Report of Four Cases and Review of the Literature*
CASE REPORT 823 s Dermatophytosis caused by Microsporum gypseum in infants: report of four cases and review of the literature* Beatriz da Silva Souza1 Débora Sarzi Sartori2 Carin de Andrade3 Edna Weisheimer4 Ana Elisa Kiszewski1 DOI: http://dx.doi.org/10.1590/abd1806-4841.20165044 Abstract: Dermatophytosis caused by Microsporum gypseum is rare, especially in infants, with few published cases. Diagnosis in this age group is frequently delayed. We review the literature and report 4 new cases of tinea of glabrous skin caused by M. gypseum mimicking eczema in infants. Considering new and previously reported cases, half of patients were exposed to sand, emphasizing the importance of this transmission vehicle in this age group. In conclusion, although rare, dermatophytosis by M. gypseum should be part of the differential diagnosis of inflammatory dermatosis in infants. A clinical suspicion and the availability of culture are keys to the diagnosis. Keywords: Infant; Microsporum; Tinea INTRODUCTION Three of four patients (patients 1, 2 and 4) received the Microsporum gypseum is a geophilic fungus that has a world- wrong diagnosis of infected atopic dermatitis, and one patient wide distribution and rarely causes disease in humans. This fungus (patient 3), of diaper dermatitis. All were mistakenly treated with may be found in dogs and cats (which can be asymptomatic car- topical steroids prescribed by the pediatrician. Scales and pustule riers), in sick human beings, and especially in contaminated soil.1- contents were collected for direct mycological examination (DME). 4 Dermatophytosis caused by M. gypseum usually manifests as an Microscopy was performed after clarification with KOH solution inflammatory mycosis that typically affects the glabrous skin and 20%. -

Superficial Mycoses in Dogs and Cats 16
Superficial Mycoses 2 in Dogs and Cats ESCCAP Guideline 02 Fourth Edition – February 2019 1 ESCCAP Malvern Hills Science Park, Geraldine Road, Malvern, Worcestershire, WR14 3SZ, United Kingdom First Edition Published by ESCCAP in March 2008 © ESCCAP 2008–2019 All rights reserved This publication is made available subject to the condition that any redistribution or reproduction of part or all of the contents in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise is with the prior written permission of ESCCAP. This publication may only be distributed in the covers in which it is first published unless with the prior written permission of ESCCAP. A catalogue record for this publication is available from the British Library. ISBN: 978-1-907259-73-9 2 TABLE OF CONTENTS INTRODUCTION 5 1. CONSIDERATION OF PET HEALTH AND LIFESTYLE FACTORS 6 2. CONTROL OF DERMATOPHYTOSIS IN DOGS AND CATS 8 2.1. Diagnosis 8 2.2. Treatment Procedures 10 2.3. Prevention 11 3. ENVIRONMENTAL CONTROL OF DERMATOPHYTE TRANSMISSION 12 4. CONTROL OF MALASSEZIA DERMATITIS IN DOGS AND CATS 12 4.1 Diagnosis 12 4.2. Treatment Procedures 13 5. OWNER CONSIDERATIONS IN PREVENTING ZOONOTIC DISEASES 14 6. STAFF, PET OWNER AND COMMUNITY EDUCATION 14 APPENDIX 1 – BACKGROUND 17 Superficial Mycoses 2 in Dogs and Cats ESCCAP Guideline 02 Fourth Edition – February 2019 3 TABLES Table 1: Characteristics of major dermatophyte species infecting dogs and cats in Europe 14 Table 2: Characteristics of Malassezia species recovered from the skin of animals -

First Report on the Occurence of Dermatophytes of Microsporum
diversity Communication First Report on the Occurence of Dermatophytes of Microsporum Cookei Clade and Close Affinities to Paraphyton Cookei in the Harmanecká Cave (Vel’ká Fatra Mts., Slovakia) Rafał Ogórek 1,* , Agata Piecuch 1, Zuzana Viš ˇnovská 2, Magdalena Cal 1 and Katarzyna Nied´zwiecka 1 1 Department of Mycology and Genetics, Institute of Genetics and Microbiology, University of Wroclaw, Przybyszewskiego Street 63/77, 51-148 Wroclaw, Poland; [email protected] (A.P.); [email protected] (M.C.); [email protected] (K.N.) 2 State Nature Conservancy of the Slovak Republic, Slovak Caves Administration, Hodžova 11, 031-01 Liptovský Mikuláš, Slovakia; [email protected] * Correspondence: [email protected]; Tel.: +48-71-375-6291; Fax: +48-71-325-2151 Received: 2 October 2019; Accepted: 11 October 2019; Published: 13 October 2019 Abstract: Keratinolytic and keratinophilic fungi, such as dermatophytes, are frequently a cause of infections in humans and animals. Underground ecosystems are inhabited by various animals and are of interest for tourists. Therefore, the main goal of our research was the first evaluation of sediment and soil samples taken inside and outside the Harmanecká Cave in Slovakia for the occurrence of keratinolytic and keratinophilic fungi. Tests with Vanbreuseghema bait, as well as phenotyping and molecular methods, showed that all of the sampling sites contained ten isolates, all of the same species of keratinophilic fungi, belonging to the Microsporum cookei clade and with close affinities to Paraphyton cookei (Ajello) Y. Gräser, Dukik & de Hoog. Our research showed that, dependent on the medium, its mycelium varied in color and showed different growth rates. -
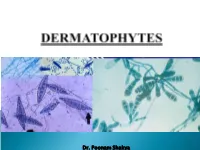
Dr. Poonam Shakya Fungi That Require and Use Keratin for Growth Confined to the Superficial Integument of the Skin, Nails, Claws & Hair of Animals and Man
Dr. Poonam Shakya Fungi that require and use keratin for growth Confined to the superficial integument of the skin, nails, claws & hair of animals and man Classical lesions- circular ( ringworm) Traditionally the dermatophytes are placed in the Deuteromycota or Fungi Imperfecti in 3 genera: Microsporum, Trichophyton Epidermophyton The Microsporum species tend to produce spindle shaped macroconidia Microsporum canis: spindle-shaped macroconidia. (LPCB, ×400) Microsporum gypseum: boat shaped macroconidia. (LPCB) Trichophyton mentagrophytes: cigar shaped numerous microconidia and a macroconidium. Microsporum nanum: round & two celled macroconidia. (LPCB) The geophilic (soil-loving) dermatophytes inhabit the soil and can exist there as free-living saprophytes. Example- Microsporum gypseum and M. nanum The zoophilic dermatophytes are obligate pathogens, primarily parasitizing animals but also capable of infecting humans. Humans are the main host for the anthropophilic dermatophytes and these very rarely cause ringworm in animals Some dermatophytes have become adapted for survival in the skin of specific host animals, for example: Microsporum canis: cats Microsporum persicolor: voles Trichophyton mentagrophytes var. mentagrophytes: rodents Trichophyton verrucosum: cattle. Trichophyton erinacei: muzzle alopecia in a terrier known to worry hedgehogs. Infective arthrospores germinate within 6 hours of adhering to keratinized structures. Minor trauma of the skin and dampness may facilitate infection. The ability of the dermatophytes -

8 Microsporum Alic
Boletín Micológico Vol. 22: 1 - 8 2007 ONYGENALES (EUROTIOMYCETES, ASCOMYCOTA) QUERATINOFILICOS EN SUELOS DE ESTABLECIMIENTOS EDUCACIONALES URBANOS Y RURALES DE LA V REGION, CHILE. Queratinophilic Onygenales (Eurotiomycetes, Ascomycota) in urban and rural soils of eduacational center of V Region, Chile) Toro, M.A., Ferrari, B., Pino, J., & Piontelli, E. Universidad de Valparaíso, Escuela de Medicina, Cátedra de Micología, Casilla 93 V, Valparaíso, Chile. email: [email protected] Palabras clave: Onygenales, hongos queratinofílicos, suelos urbanos-rurales, establecimientos educacionales. Key words: Onygenales, keratinophilic fungi, urbans-rural soils, educacional centers. RESUMEN ABSTRACT Con la finalidad de estudiar la presencia de With the purpose of studying the presence of Onygenales queratinofílicas potencialmente patógenas keratinophilic Onygenales that are potentially para el hombre y los animales, se analizaron mediante pathogenous for man and animal, urban and rural soils la técnica del anzuelo queratínico (Marzo – Diciembre, from educational centers in the V Region were examined 2006), suelos de establecimientos educacionales with the keratinic bait technique (march-december urbanos y rurales de la V Región, Chile. Se colectaron 2006). un total de 64 muestras, de las cuales, la mitad se A total of 64 samples were collected , 32 of them obtuvieron en Valparaíso-Viña del Mar (urbano) y la being from Valparaíso-Viña del Mar (urban) while the otra en Olmué-Limache (en zonas rurales). En zona rest in Olmué-Limache (in rural zones). One hundred and urbana se aislaron 112 cepas (7 géneros y 12 especies) twelve strains (7 genera and 12 species) were collected y en la rural 147 (11 géneros y 18 especies).