First Case of Periprosthetic Joint Infection Due to Clostridioides Difficile in China Yang Song1, Hong Yi Shao1, Xiang Cheng2 and Yu Guo2*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
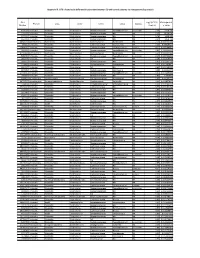
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I
ISSN 0026-2617, Microbiology, 2008, Vol. 77, No. 4, pp. 497–503. © Pleiades Publishing, Ltd., 2008. Original Russian Text © I.A. Beleneva, 2008, published in Mikrobiologiya, 2008, Vol. 77, No. 4, pp. 558–565. EXPERIMENTAL ARTICLES Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I. A. Beleneva1 Zhirmunskii Institute of Marine Biology, Far East Division, Russian Academy of Sciences, ul. Pal’chevskogo, 17, Vladivostok 690041, Russia Received May 28, 2007 Abstract—Bacilli of the species Bacillus subtilis, B. pumilus, B. mycoides, B. marinus and B. licheniformis (a total of 53 strains) were isolated from 15 invertebrate species and the water of the Vostok Bay, Peter the Great Bay, Sea of Japan. Bacilli were most often isolated from bivalves (22.7%) and sea cucumbers (18.9%); they occurred less frequently in sea urchins and starfish (13.2 and 7.5%, respectively). Most of bacilli strains were isolated from invertebrates inhabiting silted sediments. No Bacillus spp. strains were isolated from invertebrates inhabiting stony and sandy environments. The species diversity of bacilli isolated from marine objects under study was low. Almost all bacterial isolates were resistant to lincomycin. Unlike B. pumilus, B. subtilis isolates were mostly resistant to benzylpenicillin and ampicillin. Antibiotic sensitivity of B. licheniformis strains was variable (two strains were resistant to benzylpenicillin and oxacillin, while one was sensitive). A significant fraction of isolated bacilli contained pigments. Pigmented strains were more often isolated from seawater sam- ples, while colorless ones predominated within hydrobionts. B. subtilis colonies had the broadest range of co- lors. -

Probiotic Lactic Acid Bacteria Vs. Bacilli: Pros and Cons ARTHUR C
Probiotic lactic acid bacteria vs. bacilli: pros and cons ARTHUR C. OUWEHAND1*, SOFIA FORSSTEN1, MARKUS LEHTINEN1, ELIZABETH GALBRAITH2, ELLEN DAVIS2 *Corresponding author 1. Active Nutrition, DuPont Nutrition & Health, Sokeritehtaantie 20, 02460 Kantvik, Finland Arthur C. Ouwehand 2. Animal and Environmental Applications, DuPont Nutrition & Health, W227 N752 Westmound Drive, Waukesha, WI 53186, USA KEYWORDS: probiotic, lactic acid bacteria, Lactobacillus, Bifidobacterium, Bacillus, spores ABSTRACT: Both lactic acid bacteria (LAB) and bacilli are commercialised as probiotics; LAB are mainly utilised as live and active or dormant cells, while bacilli are utilised as spores. Belonging to very different genera, they have different technological properties. LAB have a longer history of use as probiotics and therefore have a broader base as far as health efficacy documentation is concerned. The question therefore sometimes arises; strains from which of these groups make better probiotics? Considering the fact that probiotics, by definition, have to be viable in sufficient numbers and have to have documented health benefits, this is not a relevant question. Any microbial strain has to fulfil these criteria in order to qualify as a probiotic. The current paper reviews and compares the available data for both groups of organisms. Pre - Probiotics INTRODUCTION In order to supply consumers with products that provide meaningful levels of probiotics, several requirements have There is no legal description of probiotics. However, the most to be fulfilled by probiotic strains selected for industrial commonly accepted definition is from a FAO/WHO working production. Quality-control must be vigilantly performed, group: “Live microorganisms which when administered in assuring identity, viability and absence of contaminants. -

Horizontal Gene Flow Into Geobacillus Is Constrained by the Chromosomal Organization of Growth and Sporulation
bioRxiv preprint doi: https://doi.org/10.1101/381442; this version posted August 2, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Horizontal gene flow into Geobacillus is constrained by the chromosomal organization of growth and sporulation Alexander Esin1,2, Tom Ellis3,4, Tobias Warnecke1,2* 1Molecular Systems Group, Medical Research Council London Institute of Medical Sciences, London, United Kingdom 2Institute of Clinical Sciences, Faculty of Medicine, Imperial College London, London, United Kingdom 3Imperial College Centre for Synthetic Biology, Imperial College London, London, United Kingdom 4Department of Bioengineering, Imperial College London, London, United Kingdom *corresponding author ([email protected]) 1 bioRxiv preprint doi: https://doi.org/10.1101/381442; this version posted August 2, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Abstract Horizontal gene transfer (HGT) in bacteria occurs in the context of adaptive genome architecture. As a consequence, some chromosomal neighbourhoods are likely more permissive to HGT than others. Here, we investigate the chromosomal topology of horizontal gene flow into a clade of Bacillaceae that includes Geobacillus spp. Reconstructing HGT patterns using a phylogenetic approach coupled to model-based reconciliation, we discover three large contiguous chromosomal zones of HGT enrichment. -

Multi-Product Lactic Acid Bacteria Fermentations: a Review
fermentation Review Multi-Product Lactic Acid Bacteria Fermentations: A Review José Aníbal Mora-Villalobos 1 ,Jéssica Montero-Zamora 1, Natalia Barboza 2,3, Carolina Rojas-Garbanzo 3, Jessie Usaga 3, Mauricio Redondo-Solano 4, Linda Schroedter 5, Agata Olszewska-Widdrat 5 and José Pablo López-Gómez 5,* 1 National Center for Biotechnological Innovations of Costa Rica (CENIBiot), National Center of High Technology (CeNAT), San Jose 1174-1200, Costa Rica; [email protected] (J.A.M.-V.); [email protected] (J.M.-Z.) 2 Food Technology Department, University of Costa Rica (UCR), San Jose 11501-2060, Costa Rica; [email protected] 3 National Center for Food Science and Technology (CITA), University of Costa Rica (UCR), San Jose 11501-2060, Costa Rica; [email protected] (C.R.-G.); [email protected] (J.U.) 4 Research Center in Tropical Diseases (CIET) and Food Microbiology Section, Microbiology Faculty, University of Costa Rica (UCR), San Jose 11501-2060, Costa Rica; [email protected] 5 Bioengineering Department, Leibniz Institute for Agricultural Engineering and Bioeconomy (ATB), 14469 Potsdam, Germany; [email protected] (L.S.); [email protected] (A.O.-W.) * Correspondence: [email protected]; Tel.: +49-(0331)-5699-857 Received: 15 December 2019; Accepted: 4 February 2020; Published: 10 February 2020 Abstract: Industrial biotechnology is a continuously expanding field focused on the application of microorganisms to produce chemicals using renewable sources as substrates. Currently, an increasing interest in new versatile processes, able to utilize a variety of substrates to obtain diverse products, can be observed. -

36 Non-Sporing Anaerobes
Non-Sporing Anaerobes MODULE Microbiology 36 NON-SPORING ANAEROBES Notes 36.1 INTRODUCTION Anaerobic bacteria are widespread and very important. They do not require oxygen for growth, which is often toxic for them. They lack the enzymes superoxide dismutase, peroxidase and/or catalase, which makes them susceptible to oxygen derived free radicals. These organisms obtain energy from fermentation process. These bacteria form the commensal flora of mouth and oropharynx, gastrointestinal tract and genitourinary tract. OBJECTIVES After reading this lesson, you will be able to: z classify the non-sporing anaerobes. z describe their pathogenic potential. z explain the laboratory diagnosis of the important pathogenic species. 36.2 NON-SPORING ANAEROBES The anaerobic bacteria can be sporogenous (eg. Clostridium species) or non- sporing (eg Bacteroides species). Non-sporing anaerobes constitute an important cause of human infections. Even in seemingly anaerobic conditions as the mouth and the skin, anaerobic bacteria are ten to thirty times more frequent than aerobes. These bacteria differ widely in the degree of anaerobiosis required for their growth. MICROBIOLOGY 331 MODULE Non-Sporing Anaerobes Microbiology (a) Facultative anaerobes - Can grow in the presence or absence of oxygen. Obtain energy by both respiration and fermentation. Oxygen not toxic, – 2- some use nitrate (NO3 ) or sulphate (SO4 ) as a terminal electron acceptor under anaerobic conditions. E.g. Peptostreptococcus. (b) Obligate (strict) anaerobes - Oxygen is toxic to these organisms, do not use oxygen as terminal electron acceptor. E.g Bacteriodes. Notes (c) Microaerophilic organisms - require low levels of oxygen for growth, but cannot tolerate the levels present in the atmosphere. E.g. -

Use of the Diagnostic Bacteriology Laboratory: a Practical Review for the Clinician
148 Postgrad Med J 2001;77:148–156 REVIEWS Postgrad Med J: first published as 10.1136/pmj.77.905.148 on 1 March 2001. Downloaded from Use of the diagnostic bacteriology laboratory: a practical review for the clinician W J Steinbach, A K Shetty Lucile Salter Packard Children’s Hospital at EVective utilisation and understanding of the Stanford, Stanford Box 1: Gram stain technique University School of clinical bacteriology laboratory can greatly aid Medicine, 725 Welch in the diagnosis of infectious diseases. Al- (1) Air dry specimen and fix with Road, Palo Alto, though described more than a century ago, the methanol or heat. California, USA 94304, Gram stain remains the most frequently used (2) Add crystal violet stain. USA rapid diagnostic test, and in conjunction with W J Steinbach various biochemical tests is the cornerstone of (3) Rinse with water to wash unbound A K Shetty the clinical laboratory. First described by Dan- dye, add mordant (for example, iodine: 12 potassium iodide). Correspondence to: ish pathologist Christian Gram in 1884 and Dr Steinbach later slightly modified, the Gram stain easily (4) After waiting 30–60 seconds, rinse with [email protected] divides bacteria into two groups, Gram positive water. Submitted 27 March 2000 and Gram negative, on the basis of their cell (5) Add decolorising solvent (ethanol or Accepted 5 June 2000 wall and cell membrane permeability to acetone) to remove unbound dye. Growth on artificial medium Obligate intracellular (6) Counterstain with safranin. Chlamydia Legionella Gram positive bacteria stain blue Coxiella Ehrlichia Rickettsia (retained crystal violet). -

Guide to Turning an RDP File Into a Data Set
Guide to Turning an RDP File into a Data Set Berkley Shands, Patricio S. La Rosa, Elena Deych, William Shannon July 5, 2017 Below we will define the basic steps required to generate a data set from an RDP file 1. Take an RDP file such as this example: ;Root:1.0;Bacteria:1.0;Firmicutes:1.0;Bacilli:1.0;Bacillales:1.0;Staphylococcaceae:1.0; ;Root:1.0;Bacteria:1.0;Firmicutes:1.0;Bacilli:1.0;Lactobacillales:1.0;Carnobacteriaceae:0.8; ;Root:1.0;Bacteria:1.0;Bacteroidetes:1.0;Bacteroidia:1.0;Bacteroidales:1.0;Prevotellaceae:1.0; ;Root:1.0;Bacteria:1.0;Bacteroidetes:1.0;Bacteroidia:1.0;Bacteroidales:1.0;Prevotellaceae:1.0; ;Root:1.0;Bacteria:1.0;Bacteroidetes:1.0;Bacteroidia:1.0;Unclassified:0.5;Unclassified:0.5; 2. Take the first entry and seperate each level into its own row, while seper- ating levels by a period: Root, 1 Root.Bacteria, 1 Root.Bacteria.Firmicutes, 1 Root.Bacteria.Firmicutes.Bacilli, 1 Root.Bacteria.Firmicutes.Bacilli.Bacillales, 1 Root.Bacteria.Firmicutes.Bacilli.Bacillales.Staphylococcaceae, 1 3. Do the same with each following row, adding to the number at the end if it is the same: Root, 5 Root.Bacteria, 5 Root.Bacteria.Firmicutes, 2 Root.Bacteria.Firmicutes.Bacilli, 2 Root.Bacteria.Firmicutes.Bacilli.Bacillales, 1 Root.Bacteria.Firmicutes.Bacilli.Bacillales.Staphylococcaceae, 1 Root.Bacteria.Firmicutes.Bacilli.Lactobacillales, 1 Root.Bacteria.Firmicutes.Bacilli.Lactobacillales.Carnobacteriaceae, .8 Root.Bacteria.Bacteroidetes, 3 Root.Bacteria.Bacteroidetes.Bacteroidia, 3 Root.Bacteria.Bacteroidetes.Bacteroidia.Bacteroidales, 2 Root.Bacteria.Bacteroidetes.Bacteroidia.Bacteroidales.Prevotellaceae, 2 Root.Bacteria.Bacteroidetes.Bacteroidia.Unclassified, .5 Root.Bacteria.Bacteroidetes.Bacteroidia.Unclassified.Unclassified, .5 4. -

Non-Sporing Anaerobes
NON-SPORING ANAEROBES Dr. R.K.Kalyan Professor Microbiology KGMU, Lko Beneficial Role of Commensal non-sporing Anaerobes Part of normal flora, modulate physiological functions Compete with pathogenic bacteria Modulate host’s intestinal innate immune response‰ Production of vitamins like biotin, vit-B12 and K ‰Polysaccharide A of Bacteroides fragilis influences the normal development and function of immune system and protects against inflammatory bowel disease. Lactobacilli maintain the vaginal acidic pH which prevents colonization of pathogens. Non-sporing Anaerobes Causing Disease ‰Anaerobic infections occur when the harmonious relationship between the host and the bacteria is disrupted ‰Disruption of anatomical barrier (skin and mucosal barrier) by surgery, trauma, tumour, ischemia, or necrosis (all of which can reduce local tissue redox potentials) allow the penetration of many anaerobes, resulting in mixed infection Classification of non-sporing anaerobes Gram-positive cocci Gram-negative cocci • Peptostreptococcus •Veillonella • Peptococcus Gram-positive bacilli Gram-negative bacilli •Bifidobacterium • Bacteroides • Eubacterium • Prevotella • Propionibacterium • Porphyromonas • Lactobacillus • Fusobacterium •Actinomyces • Leptotrichia • Mobiluncus Spirochete • Treponema, Borrelia Anaerobes as a part of normal flora Anatomic Total Anaerobic/Aero Common anaerobic al Site bacteria/ bic Ratio Normal flora gm or ml MOUTH Saliva 108–109 1:1 Anaerobic cocci Actinomyces 10 11 Tooth 10 –10 1:1 Fusobacterium surface Bifidobacterium -

Prevotella Intermedia
The principles of identification of oral anaerobic pathogens Dr. Edit Urbán © by author Department of Clinical Microbiology, Faculty of Medicine ESCMID Online University of Lecture Szeged, Hungary Library Oral Microbiological Ecology Portrait of Antonie van Leeuwenhoek (1632–1723) by Jan Verkolje Leeuwenhook in 1683-realized, that the film accumulated on the surface of the teeth contained diverse structural elements: bacteria Several hundred of different© bacteria,by author fungi and protozoans can live in the oral cavity When these organisms adhere to some surface they form an organizedESCMID mass called Online dental plaque Lecture or biofilm Library © by author ESCMID Online Lecture Library Gram-negative anaerobes Non-motile rods: Motile rods: Bacteriodaceae Selenomonas Prevotella Wolinella/Campylobacter Porphyromonas Treponema Bacteroides Mitsuokella Cocci: Veillonella Fusobacterium Leptotrichia © byCapnophyles: author Haemophilus A. actinomycetemcomitans ESCMID Online C. hominis, Lecture Eikenella Library Capnocytophaga Gram-positive anaerobes Rods: Cocci: Actinomyces Stomatococcus Propionibacterium Gemella Lactobacillus Peptostreptococcus Bifidobacterium Eubacterium Clostridium © by author Facultative: Streptococcus Rothia dentocariosa Micrococcus ESCMIDCorynebacterium Online LectureStaphylococcus Library © by author ESCMID Online Lecture Library Microbiology of periodontal disease The periodontium consist of gingiva, periodontial ligament, root cementerum and alveolar bone Bacteria cause virtually all forms of inflammatory -

Identification and Antimicrobial Susceptibility Testing of Anaerobic
antibiotics Review Identification and Antimicrobial Susceptibility Testing of Anaerobic Bacteria: Rubik’s Cube of Clinical Microbiology? Márió Gajdács 1,*, Gabriella Spengler 1 and Edit Urbán 2 1 Department of Medical Microbiology and Immunobiology, Faculty of Medicine, University of Szeged, 6720 Szeged, Hungary; [email protected] 2 Institute of Clinical Microbiology, Faculty of Medicine, University of Szeged, 6725 Szeged, Hungary; [email protected] * Correspondence: [email protected]; Tel.: +36-62-342-843 Academic Editor: Leonard Amaral Received: 28 September 2017; Accepted: 3 November 2017; Published: 7 November 2017 Abstract: Anaerobic bacteria have pivotal roles in the microbiota of humans and they are significant infectious agents involved in many pathological processes, both in immunocompetent and immunocompromised individuals. Their isolation, cultivation and correct identification differs significantly from the workup of aerobic species, although the use of new technologies (e.g., matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, whole genome sequencing) changed anaerobic diagnostics dramatically. In the past, antimicrobial susceptibility of these microorganisms showed predictable patterns and empirical therapy could be safely administered but recently a steady and clear increase in the resistance for several important drugs (β-lactams, clindamycin) has been observed worldwide. For this reason, antimicrobial susceptibility testing of anaerobic isolates for surveillance -

Bacteriology
SECTION 1 High Yield Microbiology 1 Bacteriology MORGAN A. PENCE Definitions Obligate/strict anaerobe: an organism that grows only in the absence of oxygen (e.g., Bacteroides fragilis). Spirochete Aerobe: an organism that lives and grows in the presence : spiral-shaped bacterium; neither gram-positive of oxygen. nor gram-negative. Aerotolerant anaerobe: an organism that shows signifi- cantly better growth in the absence of oxygen but may Gram Stain show limited growth in the presence of oxygen (e.g., • Principal stain used in bacteriology. Clostridium tertium, many Actinomyces spp.). • Distinguishes gram-positive bacteria from gram-negative Anaerobe : an organism that can live in the absence of oxy- bacteria. gen. Bacillus/bacilli: rod-shaped bacteria (e.g., gram-negative Method bacilli); not to be confused with the genus Bacillus. • A portion of a specimen or bacterial growth is applied to Coccus/cocci: spherical/round bacteria. a slide and dried. Coryneform: “club-shaped” or resembling Chinese letters; • Specimen is fixed to slide by methanol (preferred) or heat description of a Gram stain morphology consistent with (can distort morphology). Corynebacterium and related genera. • Crystal violet is added to the slide. Diphtheroid: clinical microbiology-speak for coryneform • Iodine is added and forms a complex with crystal violet gram-positive rods (Corynebacterium and related genera). that binds to the thick peptidoglycan layer of gram-posi- Gram-negative: bacteria that do not retain the purple color tive cell walls. of the crystal violet in the Gram stain due to the presence • Acetone-alcohol solution is added, which washes away of a thin peptidoglycan cell wall; gram-negative bacteria the crystal violet–iodine complexes in gram-negative appear pink due to the safranin counter stain.