Periodontal Microbiology 2 Alexandrina L
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Group a Streptococcus Produce Pilus-Like Structures Containing Protective Antigens and Lancefield T Antigens
Group A Streptococcus produce pilus-like structures containing protective antigens and Lancefield T antigens Marirosa Mora*†, Giuliano Bensi*†, Sabrina Capo*, Fabiana Falugi*, Chiara Zingaretti*, Andrea G. O. Manetti*, Tiziana Maggi*, Anna Rita Taddei‡, Guido Grandi*, and John L. Telford*§ *Chiron Vaccines, Via Fiorentina 1, 53100 Siena, Italy; and ‡Centro Interdipartimentale di Microscopia Elettronica, University of Tuscia, 01100 Viterbo, Italy Communicated by Rino Rappuoli, Chiron Corporation, Siena, Italy, September 8, 2005 (received for review July 29, 2005) Although pili have long been recognized in Gram-negative patho- extensively characterized and despite five decades of study, there gens as important virulence factors involved in adhesion and is still very little known about the structure and variability of T invasion, very little is known about extended surface organelles in antigens, although a gene of unknown function has been shown Gram-positive pathogens. Here we report that Group A Strepto- to code for the antigen recognized by T6 sera (9). Here we show coccus (GAS), a Gram-positive human-specific pathogen that that four of the 20 T antigens correspond to trypsin-resistant pili causes pharyngitis, impetigo, invasive disease, necrotizing fasciitis, composed of putative adhesion proteins and that recombinant and autoimmune sequelae has long, surface-exposed, pilus-like pilus proteins confer protection against lethal GAS challenge in structures composed of members of a family of extracellular a mouse model of infection and invasive disease. matrix-binding proteins. We describe four variant pili and show that each is recognized by a specific serum of the Lancefield Materials and Methods T-typing system, which has been used for over five decades to Bacterial Strains, Media, and Growth Conditions. -

Microbiology of Endodontic Infections
Scient Open Journal of Dental and Oral Health Access Exploring the World of Science ISSN: 2369-4475 Short Communication Microbiology of Endodontic Infections This article was published in the following Scient Open Access Journal: Journal of Dental and Oral Health Received August 30, 2016; Accepted September 05, 2016; Published September 12, 2016 Harpreet Singh* Abstract Department of Conservative Dentistry & Endodontics, Gian Sagar Dental College, Patiala, Punjab, India Root canal system acts as a ‘privileged sanctuary’ for the growth and survival of endodontic microbiota. This is attributed to the special environment which the microbes get inside the root canals and several other associated factors. Although a variety of microbes have been isolated from the root canal system, bacteria are the most common ones found to be associated with Endodontic infections. This article gives an in-depth view of the microbiology involved in endodontic infections during its different stages. Keywords: Bacteria, Endodontic, Infection, Microbiology Introduction Microorganisms play an unequivocal role in infecting root canal system. Endodontic infections are different from the other oral infections in the fact that they occur in an environment which is closed to begin with since the root canal system is an enclosed one, surrounded by hard tissues all around [1,2]. Most of the diseases of dental pulp and periradicular tissues are associated with microorganisms [3]. Endodontic infections occur and progress when the root canal system gets exposed to the oral environment by one reason or the other and simultaneously when there is fall in the body’s immune when the ingress is from a carious lesion or a traumatic injury to the coronal tooth structure.response [4].However, To begin the with, issue the if notmicrobes taken arecare confined of, ultimately to the leadsintra-radicular to the egress region of pathogensIn total, and bacteria their by-productsdetected from from the the oral apical cavity foramen fall into to 13 the separate periradicular phyla, tissues. -
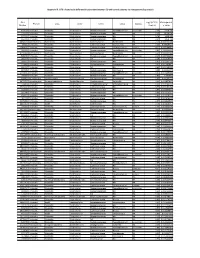
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Pathological and Therapeutic Approach to Endotoxin-Secreting Bacteria Involved in Periodontal Disease
toxins Review Pathological and Therapeutic Approach to Endotoxin-Secreting Bacteria Involved in Periodontal Disease Rosalia Marcano 1, M. Ángeles Rojo 2 , Damián Cordoba-Diaz 3 and Manuel Garrosa 1,* 1 Department of Cell Biology, Histology and Pharmacology, Faculty of Medicine and INCYL, University of Valladolid, 47005 Valladolid, Spain; [email protected] 2 Area of Experimental Sciences, Miguel de Cervantes European University, 47012 Valladolid, Spain; [email protected] 3 Area of Pharmaceutics and Food Technology, Faculty of Pharmacy, and IUFI, Complutense University of Madrid, 28040 Madrid, Spain; [email protected] * Correspondence: [email protected] Abstract: It is widely recognized that periodontal disease is an inflammatory entity of infectious origin, in which the immune activation of the host leads to the destruction of the supporting tissues of the tooth. Periodontal pathogenic bacteria like Porphyromonas gingivalis, that belongs to the complex net of oral microflora, exhibits a toxicogenic potential by releasing endotoxins, which are the lipopolysaccharide component (LPS) available in the outer cell wall of Gram-negative bacteria. Endotoxins are released into the tissues causing damage after the cell is lysed. There are three well-defined regions in the LPS: one of them, the lipid A, has a lipidic nature, and the other two, the Core and the O-antigen, have a glycosidic nature, all of them with independent and synergistic functions. Lipid A is the “bioactive center” of LPS, responsible for its toxicity, and shows great variability along bacteria. In general, endotoxins have specific receptors at the cells, causing a wide immunoinflammatory response by inducing the release of pro-inflammatory cytokines and the production of matrix metalloproteinases. -

Introduction to Bacteriology and Bacterial Structure/Function
INTRODUCTION TO BACTERIOLOGY AND BACTERIAL STRUCTURE/FUNCTION LEARNING OBJECTIVES To describe historical landmarks of medical microbiology To describe Koch’s Postulates To describe the characteristic structures and chemical nature of cellular constituents that distinguish eukaryotic and prokaryotic cells To describe chemical, structural, and functional components of the bacterial cytoplasmic and outer membranes, cell wall and surface appendages To name the general structures, and polymers that make up bacterial cell walls To explain the differences between gram negative and gram positive cells To describe the chemical composition, function and serological classification as H antigen of bacterial flagella and how they differ from flagella of eucaryotic cells To describe the chemical composition and function of pili To explain the unique chemical composition of bacterial spores To list medically relevant bacteria that form spores To explain the function of spores in terms of chemical and heat resistance To describe characteristics of different types of membrane transport To describe the exact cellular location and serological classification as O antigen of Lipopolysaccharide (LPS) To explain how the structure of LPS confers antigenic specificity and toxicity To describe the exact cellular location of Lipid A To explain the term endotoxin in terms of its chemical composition and location in bacterial cells INTRODUCTION TO BACTERIOLOGY 1. Two main threads in the history of bacteriology: 1) the natural history of bacteria and 2) the contagious nature of infectious diseases, were united in the latter half of the 19th century. During that period many of the bacteria that cause human disease were identified and characterized. 2. Individual bacteria were first observed microscopically by Antony van Leeuwenhoek at the end of the 17th century. -

Parents with Periodontitis Impact the Subgingival Colonization of Their Ofspring Mabelle Freitas Monteiro1, Khaled Altabtbaei2, Purnima S
www.nature.com/scientificreports OPEN Parents with periodontitis impact the subgingival colonization of their ofspring Mabelle Freitas Monteiro1, Khaled Altabtbaei2, Purnima S. Kumar3,4*, Márcio Zafalon Casati1, Karina Gonzales Silverio Ruiz1, Enilson Antonio Sallum1, Francisco Humberto Nociti‑Junior1 & Renato Corrêa Viana Casarin1,4 Early acquisition of a pathogenic microbiota and the presence of dysbiosis in childhood is associated with susceptibility to and the familial aggregation of periodontitis. This longitudinal interventional case–control study aimed to evaluate the impact of parental periodontal disease on the acquisition of oral pathogens in their ofspring. Subgingival plaque and clinical periodontal metrics were collected from 18 parents with a history of generalized aggressive periodontitis and their children (6–12 years of age), and 18 periodontally healthy parents and their parents at baseline and following professional oral prophylaxis. 16S rRNA amplicon sequencing revealed that parents were the primary source of the child’s microbiome, afecting their microbial acquisition and diversity. Children of periodontitis parents were preferentially colonized by Filifactor alocis, Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans, Streptococcus parasanguinis, Fusobacterium nucleatum and several species belonging to the genus Selenomonas even in the absence of periodontitis, and these species controlled inter‑bacterial interactions. These pathogens also emerged as robust discriminators of the microbial signatures of children of parents with periodontitis. Plaque control did not modulate this pathogenic pattern, attesting to the microbiome’s resistance to change once it has been established. This study highlights the critical role played by parental disease in microbial colonization patterns in their ofspring and the early acquisition of periodontitis‑related species and underscores the need for greater surveillance and preventive measures in families of periodontitis patients. -

Structural Changes in the Oral Microbiome of the Adolescent
www.nature.com/scientificreports OPEN Structural changes in the oral microbiome of the adolescent patients with moderate or severe dental fuorosis Qian Wang1,2, Xuelan Chen1,4, Huan Hu2, Xiaoyuan Wei3, Xiaofan Wang3, Zehui Peng4, Rui Ma4, Qian Zhao4, Jiangchao Zhao3*, Jianguo Liu1* & Feilong Deng1,2,3* Dental fuorosis is a very prevalent endemic disease. Although oral microbiome has been reported to correlate with diferent oral diseases, there appears to be an absence of research recognizing any relationship between the severity of dental fuorosis and the oral microbiome. To this end, we investigated the changes in oral microbial community structure and identifed bacterial species associated with moderate and severe dental fuorosis. Salivary samples of 42 individuals, assigned into Healthy (N = 9), Mild (N = 14) and Moderate/Severe (M&S, N = 19), were investigated using the V4 region of 16S rRNA gene. The oral microbial community structure based on Bray Curtis and Weighted Unifrac were signifcantly changed in the M&S group compared with both of Healthy and Mild. As the predominant phyla, Firmicutes and Bacteroidetes showed variation in the relative abundance among groups. The Firmicutes/Bacteroidetes (F/B) ratio was signifcantly higher in the M&S group. LEfSe analysis was used to identify diferentially represented taxa at the species level. Several genera such as Streptococcus mitis, Gemella parahaemolysans, Lactococcus lactis, and Fusobacterium nucleatum, were signifcantly more abundant in patients with moderate/severe dental fuorosis, while Prevotella melaninogenica and Schaalia odontolytica were enriched in the Healthy group. In conclusion, our study indicates oral microbiome shift in patients with moderate/severe dental fuorosis. -

Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I
ISSN 0026-2617, Microbiology, 2008, Vol. 77, No. 4, pp. 497–503. © Pleiades Publishing, Ltd., 2008. Original Russian Text © I.A. Beleneva, 2008, published in Mikrobiologiya, 2008, Vol. 77, No. 4, pp. 558–565. EXPERIMENTAL ARTICLES Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I. A. Beleneva1 Zhirmunskii Institute of Marine Biology, Far East Division, Russian Academy of Sciences, ul. Pal’chevskogo, 17, Vladivostok 690041, Russia Received May 28, 2007 Abstract—Bacilli of the species Bacillus subtilis, B. pumilus, B. mycoides, B. marinus and B. licheniformis (a total of 53 strains) were isolated from 15 invertebrate species and the water of the Vostok Bay, Peter the Great Bay, Sea of Japan. Bacilli were most often isolated from bivalves (22.7%) and sea cucumbers (18.9%); they occurred less frequently in sea urchins and starfish (13.2 and 7.5%, respectively). Most of bacilli strains were isolated from invertebrates inhabiting silted sediments. No Bacillus spp. strains were isolated from invertebrates inhabiting stony and sandy environments. The species diversity of bacilli isolated from marine objects under study was low. Almost all bacterial isolates were resistant to lincomycin. Unlike B. pumilus, B. subtilis isolates were mostly resistant to benzylpenicillin and ampicillin. Antibiotic sensitivity of B. licheniformis strains was variable (two strains were resistant to benzylpenicillin and oxacillin, while one was sensitive). A significant fraction of isolated bacilli contained pigments. Pigmented strains were more often isolated from seawater sam- ples, while colorless ones predominated within hydrobionts. B. subtilis colonies had the broadest range of co- lors. -

The Role of Porphyromonas Gingivalis Virulence Factors in Periodontitis Immunopathogenesis
The Role of Porphyromonas gingivalis Virulence Factors in Periodontitis Immunopathogenesis (Peran Faktor Virulensi Porphyromonas Gingivalis pada Imunopatogenesis Periodontitis) Tienneke Riana Septiwidyati, Endang Winiati Bachtiar Department of Oral Biology, Faculty of Dentistry, Universitas Indonesia, Jakarta, Indonesia, Email: [email protected] Abstract Porphyromonas gingivalis is an anaerobic Gram-negative bacteria, often associated with the pathogenesis of periodontitis. Periodontitis is a chronic inflammation characterized by damage to the supporting tissues of the tooth. Porphyromonas gingivalis locally can invade periodontal tissue and avoid host defence mechanisms. Porphyromonas gingivalis have virulence factors that can interfere with host immune response and cause inflammation at host tissue. The aim of this article is to provide an overview of the role of Porphyromonas gingivalis virulence factors such as capsules, fimbriae, lipopolysaccharides, and gingipain in the pathogenesis of periodontitis. The data sources were taken from PubMed and Google Scholar within 10 years. The role of Porphyromonas gingivalis capsule is to suppress the host's immune response to bacteria by reducing phagocytosis so the bacteria can survive. The roles of Porphyromonas gingivalis fimbriaeare to facilitate adhesion and invasion of bacteria to host cells so the damage will occur in the periodontal tissue. One of the roles of Porphyromoas gingivalis lipopolysaccharide is to disrupt the host immune system by disrupting the distribution of leukocytes around bacterial colonization so the bacteria can survive. The role of the Porphyromonas gingivalis gingipain is to suppress inflammatory cytokines thereby reducing the host's response by manipulating the complement system and disrupting the response of T cells. Porphyromonas gingivalis expresses several virulence factors involved in the colonization of subgingival plaque, modulates the immune response of host cells, and damages the host tissue directly so it can cause periodontitis. -

Periodontal, Metabolic, and Cardiovascular Disease
Pteridines 2018; 29: 124–163 Research Article Open Access Hina Makkar, Mark A. Reynolds#, Abhishek Wadhawan, Aline Dagdag, Anwar T. Merchant#, Teodor T. Postolache*# Periodontal, metabolic, and cardiovascular disease: Exploring the role of inflammation and mental health Journal xyz 2017; 1 (2): 122–135 The First Decade (1964-1972) https://doi.org/10.1515/pteridines-2018-0013 receivedResearch September Article 13, 2018; accepted October 10, 2018. List of abbreviations Abstract: Previous evidence connects periodontal AAP: American Academy of Periodontology Max Musterman, Paul Placeholder disease, a modifiable condition affecting a majority of AGEs: Advanced glycation end products Americans,What withIs So metabolic Different and cardiovascular About morbidity AgP: Aggressive periodontitis and mortality. This review focuses on the likely mediation AHA: American Heart Association ofNeuroenhancement? these associations by immune activation and their anti-CL: Anti-cardiolipin potentialWas istinteractions so anders with mental am Neuroenhancement?illness. Future anti-oxLDL: Anti-oxidized low-density lipoprotein longitudinal, and ideally interventional studies, should AP: Acute periodontitis focus on reciprocal interactions and cascading effects, as ASCVD: Atherosclerotic cardiovascular disease wellPharmacological as points for effective and Mentalpreventative Self-transformation and therapeutic C. pneumoniae in Ethic : Chlamydia pneumoniae interventionsComparison across diagnostic domains to reduce CAL: Clinical attachment loss morbidity,Pharmakologische -

Probiotic Lactic Acid Bacteria Vs. Bacilli: Pros and Cons ARTHUR C
Probiotic lactic acid bacteria vs. bacilli: pros and cons ARTHUR C. OUWEHAND1*, SOFIA FORSSTEN1, MARKUS LEHTINEN1, ELIZABETH GALBRAITH2, ELLEN DAVIS2 *Corresponding author 1. Active Nutrition, DuPont Nutrition & Health, Sokeritehtaantie 20, 02460 Kantvik, Finland Arthur C. Ouwehand 2. Animal and Environmental Applications, DuPont Nutrition & Health, W227 N752 Westmound Drive, Waukesha, WI 53186, USA KEYWORDS: probiotic, lactic acid bacteria, Lactobacillus, Bifidobacterium, Bacillus, spores ABSTRACT: Both lactic acid bacteria (LAB) and bacilli are commercialised as probiotics; LAB are mainly utilised as live and active or dormant cells, while bacilli are utilised as spores. Belonging to very different genera, they have different technological properties. LAB have a longer history of use as probiotics and therefore have a broader base as far as health efficacy documentation is concerned. The question therefore sometimes arises; strains from which of these groups make better probiotics? Considering the fact that probiotics, by definition, have to be viable in sufficient numbers and have to have documented health benefits, this is not a relevant question. Any microbial strain has to fulfil these criteria in order to qualify as a probiotic. The current paper reviews and compares the available data for both groups of organisms. Pre - Probiotics INTRODUCTION In order to supply consumers with products that provide meaningful levels of probiotics, several requirements have There is no legal description of probiotics. However, the most to be fulfilled by probiotic strains selected for industrial commonly accepted definition is from a FAO/WHO working production. Quality-control must be vigilantly performed, group: “Live microorganisms which when administered in assuring identity, viability and absence of contaminants. -

Peri-Implantitis Review a Quarterly Review of the Latest Publications Related to the Study of Peri-Implant Inflammation and Bone Loss
12 Fall 2015 Aron J. Saffer DDS MS Diplomate of the American Board of Periodontology Peri-implantitis Review A quarterly review of the latest publications related to the study of Peri-implant inflammation and bone loss A service of Dr. Aron Saffer and the Jerusalem Perio Center to provide useful, up -to date information concerning one of the most complex and troubling problems facing dental professionals today. Peri-implantitis : Microbiology • Are the Bacteria of Peri-implantitis the same as Periodontal disease? • Are we treating the infection correctly? MICROBIAL METHODS EMPLOYED • Are screw-retained restorations better than cement IN THE DIAGNOSIS OF THE retained restorations at preventing peri-implantitis PERIODONTAL PATHOGEN: Bacterial Cultivation: a method in What Does the latest Literature say? You might be surprised which the bacteria taken from infected site and is allowed to multiply on a predetermined culture media. Using light Peri-implant mucositis and Peri-implantitis is an inflammatory response microscopy the bacteria is generally due to bacteriorly driven infections, affecting the mucosal tissue and identified. eventually the bone surrounding implants. The condition was traditionally regarded to be microbiologically similar to Periodontitis. Earlier research had demonstrated that the pathogens which were found in patients with periodontal disease had similar pathogens in the sulcus around infected implants. In fact, one hypothesis suggested that the infected gingiva was a resevoir for the bacteria that would eventually translocate and infect the mucosal crevice around implants. With newer microbiological identification techniques evidence is emerging . to suggest that the ecosystem around teeth and implants differ in many ways. Have we been taking “the easy way out” by lumping ALL gingival and mucosal infection together regardless whether it surrounds a human tooth or titanium metal.