Non-Sporing Anaerobes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Relations Between Anemia and Female Adolescent's Dysmenorrhea
Universitas Ahmad Dahlan International Conference on Public Health The Relations Between Anemia and Female Adolescent’s Dysmenorrhea Paramitha Amelia Kusumawardani, Cholifah Diploma Program of Midwifery, Health Science Faculty , University of Muhammadiyah Sidoarjo Article Info ABSTRACT Keyword: Dysmenorrhea described as painful cramps in the lower abdomen that Anemia, occur during menstruation and the infection indications, pelvic disease Dysmenorrhea, moreover in the severe cases it caused fainted. The women who Female adolescents. complained dysmenorrhea problems mostly are who experience menstruation at any age. That means there is no limits age and usually dysmenorrhea often occur with dizziness, cold sweating, even fainted. In some countries the dysmenorrhea problem happens quite high as happened in the United States found 60-91% while in Indonesia amounted to 64.25%. as many as 45-75% of female adolescent experienced dysmenorrhea with the chronic or severe pain that effected to their everyday activities The number of teenagers who experience dysmenorrhea is due to high cases of anemia, irregular exercise, and lack of knowledge of nutritional status. In the previous study there are 85% of female adolescent experience dysmenorrhea. The method of this study is a correlational method with cross sectional approach. The data collecting method examining Hb levels. The population and sample of this study was 40 female adolescent The result showed that the female adolescent who had dysmenorrhea with anemia was 26 (92.4%). From the calculation by Exact Fisher the correlation between anemia and dysmenorrhea cases among female adolescent P <0.05 and p = 0.003, there was significant correlation between adolescent’s dysmenorrhea. Based on the result of statistic analysis, it can be concluded that the anemia can be categorized as one of dysmenorrhea causes. -
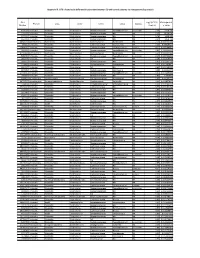
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Endometritis Caused by Chlamydia Trachomatis
Br J Vener Dis 1981; 57:191-5 Endometritis caused by Chlamydia trachomatis P-A MARDH,* B R M0LLER,t H J INGERSELV,* E NUSSLER,* L WESTROM,§ AND P W0LNER-HANSSEN§ From the *Institute of Medical Microbiology, University of Lund, Sweden; the tlnstitute of Medical Microbiology, University of Aarhus, Denmark; the *Department of Obstetrics and Gynaecology, Municipal Hospital, Aarhus, Denmark; and the §Department of Obstetrics and Gynaecology, University Hospital, Lund, Sweden SUMMARY Chlamydia trachomatis was found to be the aetiological agent of endometritis in three women with concomitant signs of salpingitis. All patients developed a significant antibody response to the organism. Chlamydia were recovered from aspirated uterine contents of two patients and darkfield examination of histological sections showed chlamydial inclusions in endometrial cells in one patient. Thus, C trachomatis can be recovered from the endometrium of patients in whom the cervical culture result is negative. In one patient curettage showed endometritis with a characteristic plasma-cell infiltration. The occurrence of chlamydial endometritis may explain why irregular bleeding is a common finding in patients with salpingitis. It also suggests a canalicular spread of chlamydia from the cervix to the Fallopian tubes. Introduction hominis and Ureaplasma urealyticum by cotton- tipped wooden sticks. Specimens for the isolation of Chlamydia trachomatis has been associated with N gonorrhoeae from the cervix and rectum were cervicitis' and salpingitis,2 and perihepatitis may collected with cotton-tipped wooden swabs treated occur in women with chlamydial genital infection.3 with charcoal. Salpingitis caused by chlamydia4 and gonococci5 are histologically similar. Gonococcal salpingitis is an Endometrial contents endosalpingitis and the infection spreads to the For the collection of end6metrial contents, a plastic Fallopian tubes from the cervix via the tube (armoured with a mandrin) was introduced endometrium.5 Experimental salpingitis in monkeys through the cervical canal. -

Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I
ISSN 0026-2617, Microbiology, 2008, Vol. 77, No. 4, pp. 497–503. © Pleiades Publishing, Ltd., 2008. Original Russian Text © I.A. Beleneva, 2008, published in Mikrobiologiya, 2008, Vol. 77, No. 4, pp. 558–565. EXPERIMENTAL ARTICLES Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I. A. Beleneva1 Zhirmunskii Institute of Marine Biology, Far East Division, Russian Academy of Sciences, ul. Pal’chevskogo, 17, Vladivostok 690041, Russia Received May 28, 2007 Abstract—Bacilli of the species Bacillus subtilis, B. pumilus, B. mycoides, B. marinus and B. licheniformis (a total of 53 strains) were isolated from 15 invertebrate species and the water of the Vostok Bay, Peter the Great Bay, Sea of Japan. Bacilli were most often isolated from bivalves (22.7%) and sea cucumbers (18.9%); they occurred less frequently in sea urchins and starfish (13.2 and 7.5%, respectively). Most of bacilli strains were isolated from invertebrates inhabiting silted sediments. No Bacillus spp. strains were isolated from invertebrates inhabiting stony and sandy environments. The species diversity of bacilli isolated from marine objects under study was low. Almost all bacterial isolates were resistant to lincomycin. Unlike B. pumilus, B. subtilis isolates were mostly resistant to benzylpenicillin and ampicillin. Antibiotic sensitivity of B. licheniformis strains was variable (two strains were resistant to benzylpenicillin and oxacillin, while one was sensitive). A significant fraction of isolated bacilli contained pigments. Pigmented strains were more often isolated from seawater sam- ples, while colorless ones predominated within hydrobionts. B. subtilis colonies had the broadest range of co- lors. -

Probiotic Lactic Acid Bacteria Vs. Bacilli: Pros and Cons ARTHUR C
Probiotic lactic acid bacteria vs. bacilli: pros and cons ARTHUR C. OUWEHAND1*, SOFIA FORSSTEN1, MARKUS LEHTINEN1, ELIZABETH GALBRAITH2, ELLEN DAVIS2 *Corresponding author 1. Active Nutrition, DuPont Nutrition & Health, Sokeritehtaantie 20, 02460 Kantvik, Finland Arthur C. Ouwehand 2. Animal and Environmental Applications, DuPont Nutrition & Health, W227 N752 Westmound Drive, Waukesha, WI 53186, USA KEYWORDS: probiotic, lactic acid bacteria, Lactobacillus, Bifidobacterium, Bacillus, spores ABSTRACT: Both lactic acid bacteria (LAB) and bacilli are commercialised as probiotics; LAB are mainly utilised as live and active or dormant cells, while bacilli are utilised as spores. Belonging to very different genera, they have different technological properties. LAB have a longer history of use as probiotics and therefore have a broader base as far as health efficacy documentation is concerned. The question therefore sometimes arises; strains from which of these groups make better probiotics? Considering the fact that probiotics, by definition, have to be viable in sufficient numbers and have to have documented health benefits, this is not a relevant question. Any microbial strain has to fulfil these criteria in order to qualify as a probiotic. The current paper reviews and compares the available data for both groups of organisms. Pre - Probiotics INTRODUCTION In order to supply consumers with products that provide meaningful levels of probiotics, several requirements have There is no legal description of probiotics. However, the most to be fulfilled by probiotic strains selected for industrial commonly accepted definition is from a FAO/WHO working production. Quality-control must be vigilantly performed, group: “Live microorganisms which when administered in assuring identity, viability and absence of contaminants. -

Horizontal Gene Flow Into Geobacillus Is Constrained by the Chromosomal Organization of Growth and Sporulation
bioRxiv preprint doi: https://doi.org/10.1101/381442; this version posted August 2, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Horizontal gene flow into Geobacillus is constrained by the chromosomal organization of growth and sporulation Alexander Esin1,2, Tom Ellis3,4, Tobias Warnecke1,2* 1Molecular Systems Group, Medical Research Council London Institute of Medical Sciences, London, United Kingdom 2Institute of Clinical Sciences, Faculty of Medicine, Imperial College London, London, United Kingdom 3Imperial College Centre for Synthetic Biology, Imperial College London, London, United Kingdom 4Department of Bioengineering, Imperial College London, London, United Kingdom *corresponding author ([email protected]) 1 bioRxiv preprint doi: https://doi.org/10.1101/381442; this version posted August 2, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Abstract Horizontal gene transfer (HGT) in bacteria occurs in the context of adaptive genome architecture. As a consequence, some chromosomal neighbourhoods are likely more permissive to HGT than others. Here, we investigate the chromosomal topology of horizontal gene flow into a clade of Bacillaceae that includes Geobacillus spp. Reconstructing HGT patterns using a phylogenetic approach coupled to model-based reconciliation, we discover three large contiguous chromosomal zones of HGT enrichment. -

Assessing Lyme Disease Relevant Antibiotics Through Gut Bacteroides Panels
Assessing Lyme Disease Relevant Antibiotics through Gut Bacteroides Panels by Sohum Sheth Abstract: Lyme borreliosis is the most prevalent vector-borne disease in the United States caused by the transmission of bacteria Borrelia burgdorferi harbored by the Ixodus scapularis ticks (Sharma, Brown, Matluck, Hu, & Lewis, 2015). Antibiotics currently used to treat Lyme disease include oral doxycycline, amoxicillin, and ce!riaxone. Although the current treatment is e"ective in most cases, there is need for the development of new antibiotics against Lyme disease, as the treatment does not work in 10-20% of the population for unknown reasons (X. Wu et al., 2018). Use of antibiotics in the treatment of various diseases such as Lyme disease is essential; however, the downside is the development of resistance and possibly deleterious e"ects on the human gut microbiota composition. Like other organs in the body, gut microbiota play an essential role in the health and disease state of the body (Ianiro, Tilg, & Gasbarrini, 2016). Of importance in the microbiome is the genus Bacteroides, which accounts for roughly one-third of gut microbiome composition (H. M. Wexler, 2007). $e purpose of this study is to investigate how antibiotics currently used for the treatment of Lyme disease in%uences the Bacteroides cultures in vitro and compare it with a new antibiotic (antibiotic X) identi&ed in the laboratory to be e"ective against B. burgdorferi. Using microdilution broth assay, minimum inhibitory concentration (MIC) was tested against nine di"erent strains of Bacteroides. Results showed that antibiotic X has a higher MIC against Bacteroides when compared to amoxicillin, ce!riaxone, and doxycycline, making it a promising new drug for further investigation and in vivo studies. -

Multi-Product Lactic Acid Bacteria Fermentations: a Review
fermentation Review Multi-Product Lactic Acid Bacteria Fermentations: A Review José Aníbal Mora-Villalobos 1 ,Jéssica Montero-Zamora 1, Natalia Barboza 2,3, Carolina Rojas-Garbanzo 3, Jessie Usaga 3, Mauricio Redondo-Solano 4, Linda Schroedter 5, Agata Olszewska-Widdrat 5 and José Pablo López-Gómez 5,* 1 National Center for Biotechnological Innovations of Costa Rica (CENIBiot), National Center of High Technology (CeNAT), San Jose 1174-1200, Costa Rica; [email protected] (J.A.M.-V.); [email protected] (J.M.-Z.) 2 Food Technology Department, University of Costa Rica (UCR), San Jose 11501-2060, Costa Rica; [email protected] 3 National Center for Food Science and Technology (CITA), University of Costa Rica (UCR), San Jose 11501-2060, Costa Rica; [email protected] (C.R.-G.); [email protected] (J.U.) 4 Research Center in Tropical Diseases (CIET) and Food Microbiology Section, Microbiology Faculty, University of Costa Rica (UCR), San Jose 11501-2060, Costa Rica; [email protected] 5 Bioengineering Department, Leibniz Institute for Agricultural Engineering and Bioeconomy (ATB), 14469 Potsdam, Germany; [email protected] (L.S.); [email protected] (A.O.-W.) * Correspondence: [email protected]; Tel.: +49-(0331)-5699-857 Received: 15 December 2019; Accepted: 4 February 2020; Published: 10 February 2020 Abstract: Industrial biotechnology is a continuously expanding field focused on the application of microorganisms to produce chemicals using renewable sources as substrates. Currently, an increasing interest in new versatile processes, able to utilize a variety of substrates to obtain diverse products, can be observed. -

36 Non-Sporing Anaerobes
Non-Sporing Anaerobes MODULE Microbiology 36 NON-SPORING ANAEROBES Notes 36.1 INTRODUCTION Anaerobic bacteria are widespread and very important. They do not require oxygen for growth, which is often toxic for them. They lack the enzymes superoxide dismutase, peroxidase and/or catalase, which makes them susceptible to oxygen derived free radicals. These organisms obtain energy from fermentation process. These bacteria form the commensal flora of mouth and oropharynx, gastrointestinal tract and genitourinary tract. OBJECTIVES After reading this lesson, you will be able to: z classify the non-sporing anaerobes. z describe their pathogenic potential. z explain the laboratory diagnosis of the important pathogenic species. 36.2 NON-SPORING ANAEROBES The anaerobic bacteria can be sporogenous (eg. Clostridium species) or non- sporing (eg Bacteroides species). Non-sporing anaerobes constitute an important cause of human infections. Even in seemingly anaerobic conditions as the mouth and the skin, anaerobic bacteria are ten to thirty times more frequent than aerobes. These bacteria differ widely in the degree of anaerobiosis required for their growth. MICROBIOLOGY 331 MODULE Non-Sporing Anaerobes Microbiology (a) Facultative anaerobes - Can grow in the presence or absence of oxygen. Obtain energy by both respiration and fermentation. Oxygen not toxic, – 2- some use nitrate (NO3 ) or sulphate (SO4 ) as a terminal electron acceptor under anaerobic conditions. E.g. Peptostreptococcus. (b) Obligate (strict) anaerobes - Oxygen is toxic to these organisms, do not use oxygen as terminal electron acceptor. E.g Bacteriodes. Notes (c) Microaerophilic organisms - require low levels of oxygen for growth, but cannot tolerate the levels present in the atmosphere. E.g. -

Use of the Diagnostic Bacteriology Laboratory: a Practical Review for the Clinician
148 Postgrad Med J 2001;77:148–156 REVIEWS Postgrad Med J: first published as 10.1136/pmj.77.905.148 on 1 March 2001. Downloaded from Use of the diagnostic bacteriology laboratory: a practical review for the clinician W J Steinbach, A K Shetty Lucile Salter Packard Children’s Hospital at EVective utilisation and understanding of the Stanford, Stanford Box 1: Gram stain technique University School of clinical bacteriology laboratory can greatly aid Medicine, 725 Welch in the diagnosis of infectious diseases. Al- (1) Air dry specimen and fix with Road, Palo Alto, though described more than a century ago, the methanol or heat. California, USA 94304, Gram stain remains the most frequently used (2) Add crystal violet stain. USA rapid diagnostic test, and in conjunction with W J Steinbach various biochemical tests is the cornerstone of (3) Rinse with water to wash unbound A K Shetty the clinical laboratory. First described by Dan- dye, add mordant (for example, iodine: 12 potassium iodide). Correspondence to: ish pathologist Christian Gram in 1884 and Dr Steinbach later slightly modified, the Gram stain easily (4) After waiting 30–60 seconds, rinse with [email protected] divides bacteria into two groups, Gram positive water. Submitted 27 March 2000 and Gram negative, on the basis of their cell (5) Add decolorising solvent (ethanol or Accepted 5 June 2000 wall and cell membrane permeability to acetone) to remove unbound dye. Growth on artificial medium Obligate intracellular (6) Counterstain with safranin. Chlamydia Legionella Gram positive bacteria stain blue Coxiella Ehrlichia Rickettsia (retained crystal violet). -

Effects of a Low-Fat Vegan Diet on Gut Microbiota in Overweight
nutrients Article Effects of a Low-Fat Vegan Diet on Gut Microbiota in Overweight Individuals and Relationships with Body Weight, Body Composition, and Insulin Sensitivity. A Randomized Clinical Trial Hana Kahleova 1,*, Emilie Rembert 1, Jihad Alwarith 1, Willy N. Yonas 1, Andrea Tura 2, Richard Holubkov 3, Melissa Agnello 4, Robynne Chutkan 5 and Neal D. Barnard 1,6 1 Physicians Committee for Responsible Medicine, Washington, DC 20016, USA; [email protected] (E.R.); [email protected] (J.A.); [email protected] (W.N.Y.); [email protected] (N.D.B.) 2 Metabolic Unit, CNR Institute of Neuroscience, 35127 Padua, Italy; [email protected] 3 School of Medicine, University of Utah, Salt Lake City, UT 84132, USA; [email protected] 4 uBiome Inc., San Francisco, CA 94103, USA; [email protected] 5 Department of Gastroenterology, Georgetown MedStar Hospital, Washington, DC 20007, USA; [email protected] 6 Adjunct Faculty, George Washington University School of Medicine and Health Sciences, Washington, DC 20052, USA * Correspondence: [email protected]; Tel.: +1-202-527-7379 Received: 24 August 2020; Accepted: 20 September 2020; Published: 24 September 2020 Abstract: Diet modulates gut microbiota and plays an important role in human health. The aim of this study was to test the effect of a low-fat vegan diet on gut microbiota and its association with weight, body composition, and insulin resistance in overweight men and women. We enrolled 168 participants and randomly assigned them to a vegan (n = 84) or a control group (n = 84) for 16 weeks. Of these, 115 returned all gut microbiome samples. -

Cervical Erosion As Result of Infectious Vaginitis
Available online a t www.pelagiaresearchlibrary.com Pelagia Research Library European Journal of Experimental Biology, 2012, 2 (5):1659-1663 ISSN: 2248 –9215 CODEN (USA): EJEBAU Cervical erosion as result of infectious vaginitis Sánchez A1, Rivera A 2* , Castillo F1 and Ortiz S1 1 Departamento de Biología Celular, Facultad de Medicina de la Benemérita Universidad Autónoma de Puebla, México. 2 Centro de Investigaciones en Ciencias Microbiológicas, Instituto de Ciencias de la Benemérita Universidad Autónoma de Puebla. _____________________________________________________________________________________________ ABSTRACT The vulvovaginitis can occur at any stage of life, being 90% of bacterial origin, parasitic and fungal agents such as Chlamydia trachomatis, Gardnerella vaginalis, Trichomonas vaginalis and Candida albicans causing erosion of cervical epithelium, so this study aims to demonstrate that vaginitis infectious agents cause erosion of the cervix of a total of 1033 patients who came to the Laboratorio de Biología Celular de la Facultad de Medicina de la Universidad Autónoma de Puebla, México in January 2001 to December 2009 the Cancer Screening Program which underwent Papanicolaou smears, the samples were stained by the modified Papanicolaou method and observed under a microscope. As for the results of 1033 patients, 378 showed vaginitis, of these, 301 were associated with infectious vaginitis and 77 without identified microorganisms but with signs of vaginitis (probably by irritation to some physical agent or vitamin A deficiency). The microorganisms found in 301 patients with vaginitis were as follows: 173 samples with abundant coccoid flora, 63 associated with flora coccoid and fungi, 37 fungi, 16 trichomonas, 3 coconuts associated with trichomonas, 3 fungi associated with Trichomonas, 2 with Trichomonas, fungi and coccoid, 2 with Gardnerella, 1 coccoid flora, and 1 Gardnerella associated with coconuts .