Identification and Antimicrobial Susceptibility Testing of Anaerobic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Feed Safety 2016
Annual Report The surveillance programme for feed materials, complete and complementary feed in Norway 2016 - Mycotoxins, fungi and bacteria NORWEGIAN VETERINARY INSTITUTE The surveillance programme for feed materials, complete and complementary feed in Norway 2016 – Mycotoxins, fungi and bacteria Content Summary ...................................................................................................................... 3 Introduction .................................................................................................................. 4 Aims ........................................................................................................................... 5 Materials and methods ..................................................................................................... 5 Quantitative determination of total mould, Fusarium and storage fungi ........................................ 6 Chemical analysis .......................................................................................................... 6 Bacterial analysis .......................................................................................................... 7 Statistical analysis ......................................................................................................... 7 Results and discussion ...................................................................................................... 7 Cereals ..................................................................................................................... -

Gut Microbiota Differences Between Psoriatic Arthritis and Undifferentiated Arthritis Patients
Gut microbiota differences between psoriatic arthritis and undifferentiated arthritis patients Chung-Yuan Hsu Chang Gung Memorial Hospital Kaohsiung Branch Ho-Chang Kuo Chang Gung Memorial Hospital Kaohsiung Branch YU-JIH Su ( [email protected] ) Chang Gung Memorial Hospital Kaohsiung Branch https://orcid.org/0000-0002-7274-3458 Research article Keywords: Psoriatic arthritis, undifferentiated arthritis, enthesitis, dactylitis, microbiota Posted Date: February 28th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-15400/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/15 Abstract Introduction Psoriatic arthritis (PSA) is a form of immune-mediated inammatory arthritis. Studying the gut microbiota of PSA patients may offer new insights into the pathophysiology of this inammatory joint disease. We designed a prospective study to examine gut microbiome from patients with PSA, primarily with enthesitis and dactylitis, and compared the data with undifferentiated arthritis patients (NO PSA), without enthesitis or dactylitis. Methods We enrolled nine PSA patients and 10 NO PSA patients in this study. The fecal samples were investigated by using 16S rRNA amplicon sequencing, followed by bioinformatics and statistical analyses. Results None of the available objective clinical laboratory data could differentiate PSA from the NO PSA subgroup. The microbiota result shows that Family: XIII_AD3011 is signicantly higher in NO PSA patients than PSA patients’ stool samples (p=0.039). Megasphaera elsdenii in the PSA was 10000 times higher than in the NO PSA group. Conclusion Our results demonstrated high intra-group homogeneous and high inter-group heterogeneous microbiota. The clinical symptoms of either enthesitis or dactylitis link to the specic microbiota in the current study. -
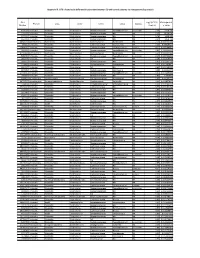
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia -

Clostridium Perfringens
CLOSTRIDIUM PERFRINGENS: SPORES & CELLS MEDIA & MODELING Promotor: prof. dr. ir. Frans M. Rombouts Hoogleraar in de levensmiddelenhygiëne en –microbiologie Co-promotor: dr. Rijkelt R. Beumer Universitair docent Leerstoelgroep levensmiddelenmicrobiologie Promotiecommissie: prof. dr. ir. Johan M. Debevere (Universiteit Gent, België) dr. ir. Servé H.W. Notermans (TNO Voeding, Zeist) prof. dr. Michael W. Peck (Institute of Food Research, Norwich, UK) prof. dr. ir. Marcel H. Zwietering (Wageningen Universiteit) CLOSTRIDIUM PERFRINGENS: SPORES & CELLS MEDIA & MODELING Aarieke Eva Irene de Jong Proefschrift ter verkrijging van de graad van doctor op gezag van de rector magnificus van Wageningen Universiteit, prof. dr. ir. L. Speelman, in het openbaar te verdedigen op dinsdag 21 oktober 2003 des namiddags te vier uur in de Aula A.E.I. de Jong – Clostridium perfringens: spores & cells, media & modeling – 2003 Thesis Wageningen University, Wageningen, The Netherlands – With summary in Dutch ISBN 90-5808-931-2 ABSTRACT Clostridium perfringens is one of the five major food borne pathogens in the western world (expressed in cases per year). Symptoms are caused by an enterotoxin, for which 6% of type A strains carry the structural gene. This enterotoxin is released when ingested cells sporulate in the small intestine. Research on C. perfringens has been limited to a couple of strains that sporulate well in Duncan and Strong (DS) medium. These abundantly sporulating strains in vitro are not necessarily a representation of the most dangerous strains in vivo. Therefore, sporulation was optimized for C. perfringens strains in general. None of the tested media and methods performed well for all strains, but Peptone-Bile- Theophylline medium (with and without starch) yielded highest spore numbers. -

Response of Gut Microbiota to Serum Metabolome Changes in Intrahepatic Cholestasis of Pregnant Patients
World Journal of W J G Gastroenterology Submit a Manuscript: https://www.f6publishing.com World J Gastroenterol 2020 December 14; 26(46): 7338-7351 DOI: 10.3748/wjg.v26.i46.7338 ISSN 1007-9327 (print) ISSN 2219-2840 (online) ORIGINAL ARTICLE Case Control Study Response of gut microbiota to serum metabolome changes in intrahepatic cholestasis of pregnant patients Guo-Hua Li, Shi-Jia Huang, Xiang Li, Xiao-Song Liu, Qiao-Ling Du ORCID number: Guo-Hua Li 0000- Guo-Hua Li, Department of Reproductive Immunology, Shanghai First Maternity and Infant 0001-9643-3991; Shi-Jia Huang 0000- Hospital, Tongji University School of Medicine, Shanghai 200040, China 0002-0081-5539; Xiang Li 0000-0002- 5970-0576; Xiao-Song Liu 0000- Shi-Jia Huang, Xiang Li, Xiao-Song Liu, Qiao-Ling Du, Department of Obstetrics, Shanghai First 0002-0160-5699; Qiao-Ling Du 0000- Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai 200040, China 0003-2079-308X. Corresponding author: Qiao-Ling Du, PhD, Doctor, Department of Obstetrics, Shanghai First Author contributions: Du QL and Maternity and Infant Hospital, Tongji University School of Medicine, No. 2699 West Gaoke Li GH proposed and designed the Road, Shanghai 200040, China. [email protected] study; Li X, Liu XS and Huang SJ collected data; Li GH and Huang SJ analyzed and interpreted data; Li Abstract GH drafted the manuscript; Du QL BACKGROUND and Huang SJ reviewed and edited Intrahepatic cholestasis in pregnancy (ICP) is the most common liver disease the manuscript; Du QL provided during pregnancy, and its exact etiology and course of progression are still poorly administrative support and understood. -

Sporulation Evolution and Specialization in Bacillus
bioRxiv preprint doi: https://doi.org/10.1101/473793; this version posted March 11, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. Research article From root to tips: sporulation evolution and specialization in Bacillus subtilis and the intestinal pathogen Clostridioides difficile Paula Ramos-Silva1*, Mónica Serrano2, Adriano O. Henriques2 1Instituto Gulbenkian de Ciência, Oeiras, Portugal 2Instituto de Tecnologia Química e Biológica, Universidade Nova de Lisboa, Oeiras, Portugal *Corresponding author: Present address: Naturalis Biodiversity Center, Marine Biodiversity, Leiden, The Netherlands Phone: 0031 717519283 Email: [email protected] (Paula Ramos-Silva) Running title: Sporulation from root to tips Keywords: sporulation, bacterial genome evolution, horizontal gene transfer, taxon- specific genes, Bacillus subtilis, Clostridioides difficile 1 bioRxiv preprint doi: https://doi.org/10.1101/473793; this version posted March 11, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. Abstract Bacteria of the Firmicutes phylum are able to enter a developmental pathway that culminates with the formation of a highly resistant, dormant spore. Spores allow environmental persistence, dissemination and for pathogens, are infection vehicles. In both the model Bacillus subtilis, an aerobic species, and in the intestinal pathogen Clostridioides difficile, an obligate anaerobe, sporulation mobilizes hundreds of genes. -

A Metagenomic Study of the Oral and Gut Microbiome in Crohn’S Disease Shijia Hu1* , Eileen Png2, Michelle Gowans3, David E
Hu et al. Gut Pathog (2021) 13:13 https://doi.org/10.1186/s13099-021-00409-5 Gut Pathogens RESEARCH Open Access Ectopic gut colonization: a metagenomic study of the oral and gut microbiome in Crohn’s disease Shijia Hu1* , Eileen Png2, Michelle Gowans3, David E. H. Ong3, Paola Florez de Sessions2, Jie Song2 and Niranjan Nagarajan2,4 Abstract Background: This study aims to characterize, the gut and oral microbiome in Asian subjects with Crohn’s disease (CD) using whole genome shotgun sequencing, thereby allowing for strain-level comparison. Methods: A case–control study with age, sex and ethnicity matched healthy controls was conducted. CD subjects were limited to well-controlled patients without oral manifestations. Fecal and saliva samples were collected for char- acterization of gut and oral microbiome respectively. Microbial DNA were extracted, libraries prepared and sequenced reads profled. Taxonomic diversity, taxonomic association, strain typing and microbial gene pathway analyses were conducted. Results: The study recruited 25 subjects with CD and 25 healthy controls. The oral microbe Streptococcus salivarius was found to be enriched and of concordant strains in the gut and oral microbiome of Crohn’s disease subjects. This was more likely in CD subjects with higher Crohn’s Disease Activity Index (184.3 2.9 vs 67.1 82.5, p 0.012) and active disease status (Diarrhoea/abdominal pain/blood-in-stool/fever and fatigue)± (p 0.016).± Gut species= found to be signifcantly depleted in CD compared to control (Relative abundance: Median[Range])= include: Faecalibacterium prausnitzii (0.03[0.00–4.56] vs 13.69[5.32–18.71], p 0.010), Roseburia inulinivorans (0.00[0.00–0.03] vs 0.21[0.01–0.53], p 0.010) and Alistipes senegalensis (0.00[0.00–0.00]= vs 0.00[0.00–0.02], p 0.029). -

Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I
ISSN 0026-2617, Microbiology, 2008, Vol. 77, No. 4, pp. 497–503. © Pleiades Publishing, Ltd., 2008. Original Russian Text © I.A. Beleneva, 2008, published in Mikrobiologiya, 2008, Vol. 77, No. 4, pp. 558–565. EXPERIMENTAL ARTICLES Distribution and Characteristics of Bacillus Bacteria Associated with Hydrobionts and the Waters of the Peter the Great Bay, Sea of Japan I. A. Beleneva1 Zhirmunskii Institute of Marine Biology, Far East Division, Russian Academy of Sciences, ul. Pal’chevskogo, 17, Vladivostok 690041, Russia Received May 28, 2007 Abstract—Bacilli of the species Bacillus subtilis, B. pumilus, B. mycoides, B. marinus and B. licheniformis (a total of 53 strains) were isolated from 15 invertebrate species and the water of the Vostok Bay, Peter the Great Bay, Sea of Japan. Bacilli were most often isolated from bivalves (22.7%) and sea cucumbers (18.9%); they occurred less frequently in sea urchins and starfish (13.2 and 7.5%, respectively). Most of bacilli strains were isolated from invertebrates inhabiting silted sediments. No Bacillus spp. strains were isolated from invertebrates inhabiting stony and sandy environments. The species diversity of bacilli isolated from marine objects under study was low. Almost all bacterial isolates were resistant to lincomycin. Unlike B. pumilus, B. subtilis isolates were mostly resistant to benzylpenicillin and ampicillin. Antibiotic sensitivity of B. licheniformis strains was variable (two strains were resistant to benzylpenicillin and oxacillin, while one was sensitive). A significant fraction of isolated bacilli contained pigments. Pigmented strains were more often isolated from seawater sam- ples, while colorless ones predominated within hydrobionts. B. subtilis colonies had the broadest range of co- lors. -

Catalase Test: Lab-3380
Standard Operating Procedure Subject Catalase Test Index Number Lab-3380 Section Laboratory Subsection Microbiology Category Departmental Contact Sarah Stoner Last Revised 9/18/2019 References Required document for Laboratory Accreditation by the College of American Pathologists (CAP), Centers for Medicare and Medicaid Services (CMS) and/or COLA. Applicable To Employees of Gundersen Health System Laboratory, Gundersen Tri-County, Gundersen St. Joseph, Gundersen Boscobel Hospital, and Gundersen Palmer Lutheran Hospital Laboratories. Detail PRINCIPLE: The breakdown of hydrogen peroxide into oxygen and water is mediated by the enzyme catalase. When a small amount of an organism that produces catalase is introduced into hydrogen peroxide, rapid elaboration of bubbles of oxygen, the gaseous product of the enzyme’s activity, is produced. CLINICAL SIGNIFICANCE: This test is used as an aid in distinguishing between Staphylococci and Streptococci. All members of the genus Staphylococcus are catalase (+), where as members of the genus Streptococcus are catalase (-). Listeria monocytogenes {catalase (+)} can be distinguished from beta-hemolytic streptococcus {catalase (-)}. Most Neisseria sp. are catalase (+). Catalase can also help distinguish Bacillus sp. {catalase (+)} from Clostridum sp. {mostly catalase (-)}. SPECIMEN: Isolates preferably grown on non-blood containing media not older than 24 hours old. REAGENTS AND MATERIALS: 1. 3% hydrogen peroxide (from stock bottle). Store 2o – 25o C. Do not freeze or overheat. Light sensitive, store in brown bottle. 2. Clean microscope slide or glass test tube 3. Wooden applicator stick EQUIPMENT/INSTRUMENTATION: N/A QUALITY CONTROL: Each new lot and shipment or once a month, perform QC on reagent with stock organisms of S aureus (positive) and Beta strep group A (negative). -

Role of Anaerobes in Dental Infection-A Review
H.Sharanya et al /J. Pharm. Sci. & Res. Vol. 10(3), 2018, 547-548 Role of Anaerobes in Dental Infection-A Review H.Sharanya, Dr.Gopinath Saveetha Dental College And Hospitals Abstract: Aim:To make a review on role of anaerobes in dental infection. Objective:To secure knowledge about the role played by anaerobes in dental infections. Background :Anaerobic bacteria have been shown to play a role in infection of all types in humans.Anaerobes make up a significant part of the oral and dental indigenous and pathogenic flora. Common anaerobic isolates include Fusobacterium, Bacteroides, Actinomyces, Peptococcus, Peptostreptococcus, Selenomonas, Eubacterium, Propionibacterium, and Treponema.Their role in periodontal disease, root canal infections, infections of the hard and soft oral tissue, as well as their importance as foci for disseminated infectious disease is well established. Reason:To enumerate the part played by anaerobes in dental infection and to know how they are interacting towards the infection and to make the people aware of those anaerobes and causes in dental infection. INTRODUCTION : variety of microorganisms(12).There are soft and hard structures, Infections caused by anaerobic bacteria are common, and may be and certain,- areas show differences in oxygen tension and in serious and life-threatening. Anaerobes predominant in the nutrition. Some surfaces protect the organisms from friction and bacterial flora of normal human skin and mucous membranes, and the flow of oral secretions, whereas other surfaces do not . are a common cause of bacterial infections of endogenous origin. Infections due to anaerobes can evolve all body systems and ANAEROBIC INFECTIONS OF THE ORAL CAVITY sites(1).The predominate ones include: abdominal, pelvic, It may be appropriate to discuss these infections according to their respiratory, and skin and soft tissues infections. -
Mass Spectrometry-Based Microbiological Testing for Blood
Nomura et al. Clin Proteom (2020) 17:14 https://doi.org/10.1186/s12014-020-09278-7 Clinical Proteomics REVIEW Open Access Mass spectrometry-based microbiological testing for blood stream infection Fumio Nomura1* , Sachio Tsuchida1, Syota Murata2, Mamoru Satoh1 and Kazuyuki Matsushita2 Abstract Background: The most successful application of mass spectrometry (MS) in laboratory medicine is identifcation (ID) of microorganisms using matrix-assisted laser desorption ionization–time of fight mass spectrometry (MALDI-TOF MS) in blood stream infection. We describe MALDI-TOF MS-based bacterial ID with particular emphasis on the methods so far developed to directly identify microorganisms from positive blood culture bottles with MALDI-TOF MS including our own protocols. We touch upon the increasing roles of Liquid chromatography (LC) coupled with tandem mass spectrometry (MS/MS) as well. Main body: Because blood culture bottles contain a variety of nonbacterial proteins that may interfere with analysis and interpretation, appropriate pretreatments are prerequisites for successful ID. Pretreatments include purifcation of bacterial pellets and short-term subcultures to form microcolonies prior to MALDI-TOF MS analysis. Three commercial protocols are currently available: the Sepsityper® kit (Bruker Daltonics), the Vitek MS blood culture kit (bioMerieux, Inc.), and the rapid BACpro® II kit (Nittobo Medical Co., Tokyo). Because these commercially available kits are costly and bacterial ID rates using these kits are not satisfactory, particularly for Gram-positive bacteria, various home-brew protocols have been developed: 1. Stepwise diferential sedimentation of blood cells and microorganisms, 2. Combi- nation of centrifugation and lysis procedures, 3. Lysis-vacuum fltration, and 4. Centrifugation and membrane fltra- tion technique (CMFT). -

Role of Hydrogen Peroxide Vapor (HPV) for the Disinfection of Hospital Surfaces Contaminated by Multiresistant Bacteria
pathogens Review Role of Hydrogen Peroxide Vapor (HPV) for the Disinfection of Hospital Surfaces Contaminated by Multiresistant Bacteria Michele Totaro, Beatrice Casini , Sara Profeti, Benedetta Tuvo, Gaetano Privitera and Angelo Baggiani * Department of Translational Research and the New Technologies in Medicine and Surgery, University of Pisa, 56123 Pisa, Italy; [email protected] (M.T.); [email protected] (B.C.); [email protected] (S.P.); [email protected] (B.T.); [email protected] (G.P.) * Correspondence: [email protected]; Tel.: 050-221-3583; Fax: 050-221-3588 Received: 10 April 2020; Accepted: 22 May 2020; Published: 24 May 2020 Abstract: The emergence of multiresistant bacterial strains as agents of healthcare-related infection in hospitals has prompted a review of the control techniques, with an added emphasis on preventive measures, namely good clinical practices, antimicrobial stewardship, and appropriate environmental cleaning. The latter item is about the choice of an appropriate disinfectant as a critical role due to the difficulties often encountered in obtaining a complete eradication of environmental contaminations and reservoirs of pathogens. The present review is focused on the effectiveness of hydrogen peroxide vapor, among the new environmental disinfectants that have been adopted. The method is based on a critical review of the available literature on this topic Keywords: hydrogen peroxide vapor; multidrug-resistant bacteria; hospital disinfection 1. Introduction The disinfection of hospital surfaces is a complex operation aimed at reducing the pathogenic microorganism load. An ideal disinfectant must be safe for human health. It may have a good stability in the environment and may be free of toxic activity [1–4].