Uhm Med 527 R.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Changing Views, Cultural Survival Knowledge and Power in the Marshall Islands
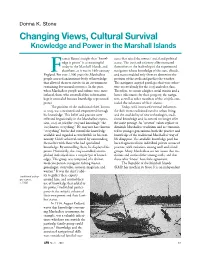
Donna K. Stone Changing Views, Cultural Survival Knowledge and Power in the Marshall Islands rancis Bacon’s insight that “knowl- sures that raised the owners’ social and political edge is power” is as meaningful status. The irooj and citizenry alike entrusted today in the Marshall Islands, and themselves to the leadership of the experienced elsewhere, as it was in 16th-century navigators whose knowledge of the stars, clouds, England.F For over 2,500 years the Marshallese and waves enabled only them to determine the people accrued an immense body of knowledge position of the atolls and predict the weather. that allowed them to survive in an environment The navigator enjoyed privileges that were other- containing few natural resources. In the past, wise reserved only for the irooj and ruler class. when Marshallese people and culture were more Therefore, to ensure a higher social station and a isolated, those who controlled this information better inheritance for their progeny, the naviga- kept it concealed because knowledge represented tors, as well as other members of the nitijela, con- power. cealed the substance of their science. The position of the traditional chief, known Today, with increased external influences, as irooj, was sanctioned and empowered through the shift from traditional rural to urban living, his knowledge. This belief and practice were and the availability of new technologies, tradi- reflected linguistically in the Marshallese expres- tional knowledge and its control no longer offer sion, irooj im jela (the irooj and knowing); “the the same prestige. As “western” values replace or irooj knows everything.” He may not have known diminish Marshallese traditions and are transmit- “everything” but he did control the knowledge ted to younger generations, both the practice and available and regarded as worthwhile in his com- knowledge of the traditional Marshallese way of munity. -

Marshallese Foodways and Culture in Springdale, Arkansas Diana Kay Chen University of Arkansas, Fayetteville
University of Arkansas, Fayetteville ScholarWorks@UARK Theses and Dissertations 5-2018 Got Breadfruit? Marshallese Foodways and Culture in Springdale, Arkansas Diana Kay Chen University of Arkansas, Fayetteville Follow this and additional works at: http://scholarworks.uark.edu/etd Part of the Social and Cultural Anthropology Commons Recommended Citation Chen, Diana Kay, "Got Breadfruit? Marshallese Foodways and Culture in Springdale, Arkansas" (2018). Theses and Dissertations. 2825. http://scholarworks.uark.edu/etd/2825 This Dissertation is brought to you for free and open access by ScholarWorks@UARK. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of ScholarWorks@UARK. For more information, please contact [email protected], [email protected]. Got Breadfruit? Marshallese Foodways and Culture in Springdale, Arkansas A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Environmental Dynamics by Diana Chen Colorado State University Bachelor of Science in BioAgricultural Sciences and Pest Management, 2002 University of Arkansas Master of Science in Crop, Soil, and Environmental Sciences, 2009 May 2018 University of Arkansas This dissertation is approved for recommendation to the Graduate Council. ______________________________ Justin Nolan, Ph.D. Dissertation Director ______________________________ ________________________________ Jamie Baum, Ph.D. Peter Ungar, Ph.D. Committee Member Committee Member ABSTRACT Understanding human food choices -

Destination: Marshall Islands. Video Guide. INSTITUTION Peace Corps, Washington, DC
DOCUMENT RESUME ED 354 198 SO 022 829 TITLE Destination: Marshall Islands. Video Guide. INSTITUTION Peace Corps, Washington, DC. Office of World Wise Schools. PUB DATE Jan 92 NOTE 82p.; For related documents, see SO 022 828-832. Accompanying videotape available from the producer; videotapes will be sent to the school librarian or media specialist. AVAILABLE FROM Peace Corps of the United States of America, Office of World Wise Schools, 1990 K Street, N.W., Washington, DC 20526. PUB TYPE Guides Classroom Use Teaching Guides (For Teacher)(052) EDRS PRICE MF01/PC04 Plus Postage. DESCRIPTORS Area Studies; Elementary Secondary Education; *Geographic Concepts; *Geography Instruction; *Multicultural Education; Social Studies; Thematic Approach; Videotape Recordings IDENTIFIERS Global Education; *Marshall Islands; *Peace Corps ABSTRACT This video guide was developed by the Peace Corps' Office of World Wise Schools. Activities that the guide describes are for use in a 3- to 5-day unit on one of the nations of Oceania, the Republic of the Marshall Islands. The activities are designed to provide students with opportunities to:(1) compr.re and contrast Marshallese and U.S. culture; and (2) relate the fundamental geographic themes of location, place, and movement with the history and culture of the Marshall Islands. Included in the guide are Level A, for grades three through five, Level B, for grades six through nine, and Level C, for grades 10 through 12. Each level includes worksheets and suggestions for using them. Fifty-seven references and a list of organizations that provided information are included. (LBG) *********************************************************************** Reproductions supplied by EDRS are the best that can be made from the original document. -

Marshall Islands Fifth National Report Convention on Biological Diversity
Republic of the Marshall Islands Fifth National Report Convention on Biological Diversity Office of Environmental Planning Policy Coordination Majuro, Republic of the Marshall Islands February 2017 1 Executive Summary This 5th National Report for the Republic of the Marshall Islands provides an update on the biodiversity status and trends, as well as progress towards the implementation of the Strategic Plan for Biodiversity 2011-2020 including the Aichi Biodiversity Target 2020. The report is divided into three main parts with part one focusing on the importance of biodiversity to the people, the state and threats to biodiversity and the implications of changes to biodiversity; part two focuses on the actions and implementation of the national biodiversity strategy and action plan; and part three focuses on alignment of national targets to the Aichi Biodiversity Targets. This report is the end product of a consultative process undertaken through the development of the national blueprint for conservation areas plan and the 2016 State of Environment report for RMI. The value of biodiversity to the wellbeing of Marshallese remains critical and it continues to inspire communities and the government to actively pursue actions and policies in order to safeguard it for future generations. Biodiversity is the cornerstone for economic opportunities and development of the country. It strengthens cultural ties of the current population to their fore-parents and through this connection provides the knowledge for community to instill good practices for the conservation of resources. Some major key drivers continue to cause significant impacts to RMI’s biodiversity and environment. Old challenges such as the fallout from nuclear testing and bombing of atolls combined with climate change and associated extreme weather events (severe and increasingly frequent typhoon events and drought) are seriously challenging the viability of communities in many of the atolls in RMI. -

IOM Policy Brief Series Issue 1 | Vol. 5
Migration, Environment and Climate Change: ISSN 2410-4930 Issue 1 | Vol. 5 Policy Brief Series July 2019 Aerial view of Aur Atoll of the Marshall Islands. © 2017/Kees VAN DER GEEST Marshallese perspectives on migration Kees van der Geest in the context of climate change Maxine Burkett Juno Fitzpatrick Mark Stege Brittany Wheeler Introduction Marshall Islands is a nation of widely dispersed, low-lying (Owen et al., 2016). As climate change causes sea levels coral atolls and islands, with approximately 70 mi2 of to rise and weather patterns to shift, the Marshall Islands land area scattered across 750,000 mi2 of ocean (Bureau face flooding, heat stress and drought that damages of East Asian and Pacific Affairs, 2015). Average elevation agriculture, livelihoods, homes and infrastructure for the Marshall Islands is approximately 2 m. above (Keener et al., 2012; Marra et al., 2017). mean sea level, and many islands and atolls are lower PUB2019/014/EL Migration, Environment and Climate Change: Policy Brief Series 2 Issue 1 | Vol. 5 | July 2019 When the frequency and intensity of climate-related Methods hazards increases, residents may have to make the difficult choice of whether to leave their home islands in The research team conducted fieldwork with the the hope of a more stable future. Marshallese migrants Marshallese in both the Marshall Islands and in move within the country to larger islands or to the destination States within the United States. The study United States of America where the Compact of Free used innovative social science methods to assess Association allows them to live and work under a special local perceptions of climate change, ecosystem status (Graham, 2008; McElfish, 2016). -

The Lolelaplap (Marshall Islands) in Us: Sailing West to East (Ralik→Ratak) to These Our Atolls (Aelon Kein Ad) Ad Jolet Je
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library | Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-18-2018 “The Lolelaplap (Marshall Islands) in Us: Sailing West to East (Ralik→Ratak) to These Our Atolls (Aelon Kein Ad) Ad Jolet Jen Anij (Our Blessed Inheritance from God)” Desmond N. Doulatram University of San Francisco, [email protected] Follow this and additional works at: https://repository.usfca.edu/capstone Part of the Cultural History Commons, Ethnic Studies Commons, Genealogy Commons, History of the Pacific slI ands Commons, Indigenous Education Commons, Indigenous Studies Commons, Linguistic Anthropology Commons, Linguistics Commons, Oral History Commons, Pacific slI ands Languages and Societies Commons, Religious Thought, Theology and Philosophy of Religion Commons, and the Social and Cultural Anthropology Commons Recommended Citation Doulatram, Desmond N., "“The Lolelaplap (Marshall Islands) in Us: Sailing West to East (Ralik→Ratak) to These Our Atolls (Aelon Kein Ad) Ad Jolet Jen Anij (Our Blessed Inheritance from God)”" (2018). Master's Projects and Capstones. 725. https://repository.usfca.edu/capstone/725 This Project/Capstone is brought to you for free and open access by the Theses, Dissertations, Capstones and Projects at USF Scholarship: a digital repository @ Gleeson Library | Geschke Center. It has been accepted for inclusion in Master's Projects and Capstones by an authorized administrator of USF Scholarship: a digital repository @ Gleeson Library | Geschke Center. For more information, please contact [email protected]. 0 “THE LOLELAPLAP (MARSHALL ISLANDS) IN US: SAILING WEST TO EAST (RALIKà RATAK) TO THESE OUR ATOLLS (AELON KEIN AD) AD JOLET JEN ANIJ (OUR BLESSED INHERITANCE FROM GOD)” Desmond Narain Doulatram APS 698: Masters in Asia Pacific Studies (MAPS) CAPSTONE March 12, 2018 1 AcknowledgementsàIen Kammolol (Gratitude) The first person I would like to thank that I always forget out of humility is myself. -

Exploring Goals of Marshallese Adolescents
Running head: EXPLORING GOALS OF MARSHALLESE ADOLESCENTS Exploring Goals of Marshallese Adolescents in a Non-Academic West Hawai‘i Youth Development Program A thesis submitted to the Graduate Division of the University of Hawai‘i at Mānoa in partial fulfillment of the requirements for the degree of Master of Education in Educational Psychology December 2019 Kamela T. Souza Thesis Committee: Lois Yamauchi, Chairperson Nicole Lewis Katherine Ratliffe EXPLORING GOALS OF MARSHALLESE ADOLESCENTS Acknowledgments I am grateful to have been given the opportunity to conduct a project in my beloved West Hawai‘i, and it would not have been possible without all the support I received. I would like to thank the members of my thesis committee and all my professors in the Educational Psychology Department. I would also like to thank the Department as well as The Learning Coalition for granting me a graduate assistantship to fund my work throughout this project. The Learning Coalition was also instrumental in helping me determine a research direction by introducing me to people in HIDOE who helped me select and complete this research project. Very many thanks to the staff I worked with from the housing complex and the summer program for helping me so much throughout the process and allowing me the chance to serve the community at the same time. I also appreciate the community partners who gave their time, knowledge, and resources to our pilot summer program. And, of course, I am also grateful to the wonderful students that I got to know over those few short weeks. Lastly, I want to acknowledge the friends and family here and abroad who supported me throughout. -

Indigenous Knowledge and Navigating the Rising Tides of Climate Change and Other Existential Threat Revista Latinoamericana De Etnomatemática, Vol
Revista Latinoamericana de Etnomatemática ISSN: 2011-5474 [email protected] Universidad de Nariño Colombia Lipka, Jerry Indigenous Knowledge and Navigating the Rising Tides of Climate Change and Other Existential Threat Revista Latinoamericana de Etnomatemática, vol. 13, no. 3, 2020, September-November, pp. 29-61 Universidad de Nariño Colombia Available in: https://www.redalyc.org/articulo.oa?id=274065861004 How to cite Complete issue Scientific Information System Redalyc More information about this article Network of Scientific Journals from Latin America and the Caribbean, Spain and Journal's webpage in redalyc.org Portugal Project academic non-profit, developed under the open access initiative Lipka, J. (2020). Indigenous Knowledge and Navigating the Rising Tides of Climate Change and Other Existential Threats. Revista Latinoamericana de Etnomatemática, 13(3), 29-61. DOI: 10.22267/relatem.20133.66 Artículo recibido el 12 de noviembre de 2020. Aceptado para publicación el 18 de diciembre de 2020 Indigenous Knowledge and Navigating the Rising Tides of Climate Change and Other Existential Threats Conocimiento Indígena y la navegación de crecientes mareas del cambio Climático y otros desafíos existenciales. Jerry Lipka1 Abstract Existential threats to Indigenous People’s lands, cultures, and languages are exacerbated and intensified by climate change and its effects, particularly to those groups deeply connected to natural systems. Through five case vignettes situated in Alaska, Yap State, and the Republic of the Marshall Islands, this paper describes adaptive responses at the intersection of Indigenous Knowledge (IK) and climate change. Though their locations, history, and customs vary, they share an underlying similarity in the urgency expressed for their Traditional Ecological Knowledge to be part of a response that leads to sustainability. -

Postcolonialism and the Marshallese Diaspora: Structural Violence and Health in the Marshallese Community in Springdale, Arkansas Alexander J
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by University of San Francisco The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library | Geschke Center Master's Theses Theses, Dissertations, Capstones and Projects Fall 12-2015 Postcolonialism and the Marshallese Diaspora: Structural Violence and Health in the Marshallese Community in Springdale, Arkansas Alexander J. Hirata University of San Francisco, [email protected] Follow this and additional works at: https://repository.usfca.edu/thes Part of the Inequality and Stratification Commons, International Public Health Commons, and the Place and Environment Commons Recommended Citation Hirata, Alexander J., "Postcolonialism and the Marshallese Diaspora: Structural Violence and Health in the Marshallese Community in Springdale, Arkansas" (2015). Master's Theses. 170. https://repository.usfca.edu/thes/170 This Thesis is brought to you for free and open access by the Theses, Dissertations, Capstones and Projects at USF Scholarship: a digital repository @ Gleeson Library | Geschke Center. It has been accepted for inclusion in Master's Theses by an authorized administrator of USF Scholarship: a digital repository @ Gleeson Library | Geschke Center. For more information, please contact [email protected]. Postcolonialism and the Marshallese Diaspora: Structural Violence and Health in the Marshallese Community in Springdale, Arkansas In Partial Fulfillment of the Requirements for the Degree MASTER OF ARTS in INTERNATIONAL STUDIES by Alexander James Hirata December 1, 2014 UNIVERSITY OF SAN FRANCISCO Under the guidance and approval of the committee, and approval by all the members, this thesis project has been accepted in partial fulfillment of the requirements for the degree. -

Ls Denver Museum of Nature & Science Annals
DENVER MUSEUM OF NATURE & SCIENCE & SCIENCE OF NATURE DENVER MUSEUM DENVER MUSEUM OF NATURE & SCIENCE ANNALS DENVER MUSEUM OF NATURE & SCIENCE ANNALS NUMBER 7, OCTOBER 11, 2018 WWW.DMNS.ORG/SCIENCE/MUSEUM-PUBLICATIONS Denver Museum of Nature & Science Annals (Print) ISSN 1948-9293 2001 Colorado Boulevard Denver, CO 80205, U.S.A. Denver Museum of Nature & Science Annals (Online) ISSN 1948-9307 ANNALS • NUMBER 7 • OCTOBER 11, 2018 • NUMBER 7 OCTOBER The Denver Museum of Nature & Science inspires curiosity and excites minds of all ages through scientific discovery and the presentation and preservation of the world’s unique treasures. Cover photo: Model Paopao (single-hull outrigger canoe) collected in Sāmoa before 1977 (DMNS A967.6). Model canoes are found all throughout the seafaring cultures of Oceania and within the walls of museums. Their presence in collections across the world continue to evince the relationship of Pacific Islanders to the sea and to each other. The Denver Museum of Nature & Science Annals is an Frank Krell, PhD, Editor-in-Chief Voyaging through the Oceanic Collection open-access, peer-reviewed scientific journal publishing EDITORIAL BOARD: original papers in the fields of anthropology, geology, at the Denver Museum of Nature & James Hagadorn, PhD (subject editor, Paleontology and paleontology, botany, zoology, space and planetary Science Geology) sciences, and health sciences. Papers are either authored Nicole Garneau, PhD (subject editor, Health Sciences) by DMNS staff, associates, or volunteers, deal with DMNS John Demboski, PhD (subject editor, Vertebrate Zoology) specimens or holdings, or have a regional focus on the Steve Lee, PhD (subject editor, Space Sciences) Rocky Mountains/Great Plains ecoregions. -

Cultural Diplomacy in the South Pacific
Cultural Diplomacy in the South Pacific Table of Contents: Cultural Diplomacy in the South Pacific 1. Introduction 2. Methodology 3. Contemporary Examples of Public Sector Sponsored Cultural Diplomacy in the South Pacific 3.1 Cook Islands 3.2 Guam 3.3 Kingdom of Tonga 3.4 Niue Island 3.5 Overseas Lands of French Polynesia 3.6 Papua New Guinea 3.7 Republic of Fiji 3.8 Republic of Palau 3.9 Republic of Marshall Islands 3.10 Republic of Vanuatu 4. Conclusion 5. References 1. Introduction Overview of the South Pacific Region The South Pacific is comprised of 20,000 to 30,000 islands which lie south of the Tropic of Cancer. The Pacific Island region covers 20 million square miles of ocean and 117,000 square miles of land, with a population of 8 million people. For the first time, the South Pacific region is facing urbanization, which has brought new challenges to this area. The rates of urban growth in the Solomon Islands and Vanuatu, both in excess of 6 per cent per annum, are among the highest in the world.1 The islands are commonly grouped into three different divisions; Melanesia, Micronesia and Polynesia. The inhabitants from each of these groups all differ by historical, geographical, language and physical characteristics. Polynesia is located in the south-eastern part of the region, Melanesia is found in the southwest, from the Arafura Sea to the western end of the Pacific Ocean and eastward to Fiji, whilst Micronesia lies in the north. The Pacific islands are classified into a high island group and a low island group. -

The Reemergence of Traditional Sailing Canoe
74496 ;3 9:7 673 9:7 77707797357 48 9736;9;4331 63;1;39 53347 4:;16;39 ;3 9:7 773:41;5 48 9:7 0376:311 ;613366 5:7;69;33 33;73 17:033 6ubmitted to the faculty of the :niversity 9raduate 6chool ;n partial fulfillment of the requirements for the degree 0aster of 1iberal 6tudies in the 5ollege of 1iberal 3rts and 6ciences of ;ndiana :niversity -uly $&&(P7$N&( P$*( 3ccepted by the 9raduate 8aculty ;ndiana :niversity in partial fulfillment of the requirements for the degree in the 0aster of 1iberal 6tudies 016 5ommittee js}6cott 7 6ernau 3h6 @~~ 7ebecca 1 9orstrick 3h6 6ate of 4ral 7xamination -uly 8or the students and teachers preserving the past in the 0arshall ;slands llo 0autiej 3elon 0ein 3d l $&KNOSL('*M(N76 ; wish to acknowledge the kqohikZpkZp lmata 0abua (3aramount 5hief) of the 0arshall ;sland for being so gracious as to allow me to conduct my research among his people and lands ; would also like to thank the dedicated staff at Baan 3elon in 0ajel whose thoughtful work in reviving traditional sailing canoe culture in the 0arshall ;slands has allowed a new generation of 0arshallese to take prjde in their past ;n particular ; wish to acknowledge 6ennis 3lessio 3lson 0elen -ill 1uciano and 0entil 1aik for allowing me access to their work site and publications that B30 has produced 0uch appreciation to :arry 3nien 0aster 5anoe builder who on 0ajikin ;sland 3amo 3toll allowed me to help him in the construction of a traditional sailing canoe and for the use of that boat 3lso to the late 0aster 3avigator 3lton who taught me about traditional