TRAPEZIO-METACARPAL JOINT ARTHRITIS of the THUMB by Bruce Steinberg, M.D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -
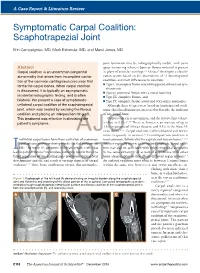
Symptomatic Carpal Coalition: Scaphotrapezial Joint
A Case Report & Literature Review E. Campaigniac et al Symptomatic Carpal Coalition: Scaphotrapezial Joint Erin Campaigniac, MD, Mark Eskander, MD, and Marci Jones, MD joint formation may be radiographically visible, with joint Abstract space narrowing wherein bone or fibrous material is present Carpal coalition is an uncommon congenital in place of articular cartilage.2,4 Minaar8 developed a classifi- abnormality that arises from incomplete cavita- cation system based on his observations of 12 lunotriquetral tion of the common cartilaginous precursor that coalitions and their differences in coalition: ◾ Type I, incomplete fusion resembling pseudarthrosis or syn- forms the carpal bones. When carpal coalition chondrosis is discovered, it is typically an asymptomatic ◾ Type II, proximal fusion with a distal notching incidental radiographic finding, and is often ◾ Type III, complete fusion, and bilateral. We present a case of symptomatic ◾ Type IV, complete fusion associated with other anomalies. unilateral carpal coalition of the scaphotrapezial Although these 4 types were based on lunotriquetral coali- joint, which was treated by excising the fibrous tions, this classification system is used to describe the coalition coalition and placing an interposition fat graft. of any carpal bone. This treatment was effective in alleviating the Carpal coalition is uncommon, and the reported prevalence 2,5,6,9 patient’s symptoms. is close to 0.1%. There is, however, an increase of up to 1.5% in patients of African descent, and 9.5% in the West Af- rican -

Trapezium Prosthetic Arthroplasty (Silicone, Artelon, Metal, and Pyrocarbon)
Trapezium Prosthetic Arthroplasty (Silicone, Artelon, Metal, and Pyrocarbon) Mark A. Vitale, MD, MPHa, Fraser Taylor, MB, BS, FRACSb,c, Mark Ross, MB, BS, FRACSb,c,d, Steven L. Moran, MDe,* KEYWORDS Thumb Trapezial-metacarpal (TM) joint Silicone Artelon Pyrocarbon Total joint arthroplasty KEY POINTS Trapezium prosthetic arthroplasty has been used to treat basal joint arthritis for nearly 5 decades. Implant arthroplasty seeks to preserve joint biomechanics, avoid metacarpal subsidence, and provide immediate stability. There has been rapid development of trapezial prosthetic implants, including synthetic interposition materials, metal total joint arthroplasties and pyrocarbon trapezial arthroplasties. While many recently available implants have been shown to have short-term success, determining the medium- to long-term outcomes require further study. INTRODUCTION method has specific advantages and disadvan- tages for the surgeon to consider. The basal joint of the thumb is the second most 1 In contrast to ablative resection and joint fusion commonly affected joint by arthritis. Degenerative procedures, which sacrifice function of the basal disease of this joint can result in significant pain, joint in an effort to provide pain relief, prosthetic ar- stiffness, weakness, and disability. Conservative throplasty offers the theoretic advantages of pres- measures, such as nonsteroidal anti-inflammatory ervation of normal anatomy and biomechanics. drugs, splinting, and intra-articular corticosteroid This could be accomplished without subsidence injections, can provide relief for some patients; for of the thumb metacarpal, with preservation of those with severe disease in whom nonoperative normal motion at the trapezialmetacarpal (TM) measures fail, many surgical methods are available, joint, prevention of metacarpophalangeal joint with successful outcomes reported in the literature. -

Trapeziectomy
Trapeziectomy What is arthritis of the Trapeziometacarpal symptoms are. You can avoid certain activities joint? that cause you pain or take painkillers. Your The Trapezium is a small wrist bone that lies at hand therapist can provide or make splints for the base of your thumb. It is commonly affected you to rest your thumb in. Your doctor may also by wear and tear, otherwise known as arthritis. inject the joint with steroid (cortisone). This can be done under ultrasound or X-ray guidance Your surgeon has recommended an operation usually on a different day from the outpatient called trapeziectomy. It is the removal of this appointment. The injection only provides bone. However, it is your decision to go ahead temporary relief of symptoms (3-6 months) with the operation or not. or may not be successful at all. Repeated This leaflet gives you information about the injections often last a shorter duration each benefits and risks to help you to make an time. They do not cure the condition. informed decision. If you have any questions Surgical options: this leaflet does not answer, please ask your surgeon or the healthcare team. 1. Trapieziectomy – This is where the bone is removed completely. The gap fills with scar There is more than one way this surgery is tissue on which your thumb will sit to reduce carried out and if you research the internet you the pain of the bone on bone rubbing. will find a lot of information about it, some of 85% of patients have a significant pain which may not be relevant to you. -

Arthritis of the Base of the Thumb
Arthritis of the Base of the Thumb What is it? How is the diagnosis made? In a normal joint, cartilage covers the end of the bones and serves as a The diagnosis is made by history and physical evaluation. Pressure and shock absorber to allow smooth, pain-free movement. In osteoarthritis (OA, movement such as twisting will produce pain at the joint. A grinding or “degenerative arthritis”) the cartilage layer wears out, resulting in direct sensation may also be present at the joint (see Figure 3). X-rays are contact between the bones and producing pain and deformity. One of the used to confirm the diagnosis, although symptom severity often does not most common joints to develop OA in the hand is the base of the thumb. correlate with x-ray findings. The thumb basal joint, also called the carpometacarpal (CMC) joint, is a specialized saddle-shaped joint that is formed by a small bone of the wrist What are the treatment options? (trapezium) and the first bone of the thumb (metacarpal). The saddle shaped Less severe thumb arthritis will usually respond to non-surgical care. joint allows the thumb to have a wide range of motions, including up, down, Arthritis medication, splinting and limited cortisone injections may help across the palm, and the ability to pinch (see Figure 1). alleviate pain. A hand therapist might provide a variety of rigid and non-rigid splints which can be used while sleeping or during activities. Figure 1: Thumb Basal Joint Patients with advanced disease or who fail non-surgical treatment may be candidates for surgical reconstruction. -

Upper Limb 3 the Wrist
Upper Limb 3 The Wrist Donald Sammut Hand Surgeon Kings Upper Limb Anatomy plus lecture notes • Unlike'many'other'joints,'the'wrist'surface'anatomy'gives'away'little'of' the'bony'structures'beneath'the'surface.' • Still'less'does'it'suggest'the'complex'ligament'structures' Carpus' Radius' Ulna' • The'wrist'is'surrounded'by'vital'structures,'tendons,'nerves,'arteries.'' • Pathology'in'these'structures'can'give'symptoms'mistaken'for'problems' with'the'wrist'joint' • 8'wrist'bones'form'the'carpus.' • Proximally'these'articulate'with'the'radius' • Distally'they'articulate'with'the'metacarpals.' • The'carpal'bones'articulate'with'each'other'in'a'particular'configuration'of' bony'shapes'and'ligaments'which'dictate'the'complex'function.' Trapezoid' Capitate' Trapezium' Hamate' Scaphoid' Pisiform' Lunate' Triquetral' • Proximally'the'carpus'articulates'with'the'distal'radius'and'with'the' triangular'fibrocartilage.' • The'TFC'separates'the'carpus'from'the'ulna' • The'distal'ulna'does'not'participate'in'the'articulation'with'the'carpus' • View'of'the'distal'radius.'Proximal'aspect'of'the'RadioKcarpal'joint' • Note'' 'the'Scaphoid'fossa' 'the'Lunate'fossa' 'the'triangular'fibrocartilage' PROXIMAL)ARTICULAR)SURFACE)OF)THE)WRIST:)RADIUS'AND'TRIANGULAR'CARTILAGE' ' THE'ULNA'IS'EXCLUDED.' • Distal'aspect'of'the'RadioKcarpal'joint' The'radius'and'triangular'fibrocartilage'articulate'with'the'scaphoid,'lunate' and'triquetral' DISTAL)ARTICULAR)SURFACE)OF)THE)WRIST:)SCAPHOID,'LUNATE','TRIQUETRAL' ' • The'bony'shapes'of'the'radiocarpal'joint'make'for'an'unstable'arrangement' -

Dorsoscapularis Triangularis: Embryological and Phylogenetic Characterization of a Rare Variation of Trapezius
Case Report http://dx.doi.org/10.5115/acb.2016.49.3.213 pISSN 2093-3665 eISSN 2093-3673 Dorsoscapularis triangularis: embryological and phylogenetic characterization of a rare variation of trapezius Lalit Mehra, Anita Tuli, Shashi Raheja Department of Anatomy, Lady Hardinge Medical College and Associated Hospitals, New Delhi, India Abstract: The muscle trapezius shows considerable morphological diversity. Variations include an anomalous origin and complete or partial absence of the muscle. The present study reported, a hitherto undocumented complete bilateral absence of the cervical part of trapezius. Based on its peculiar origin and insertion, it was named dorsoscapularis triangularis. The embryological, phylogenetic and molecular basis of the anomaly was elucidated. Failure of cranial migration of the trapezius component of the branchial musculature anlage to gain attachment on the occipital bone, cervical spinous processes, ligamentum nuchae between 11 mm and 16 mm stage of the embryo, resulted in this anomaly. A surgeon operating on the head and neck region or a radiologist analyzing a magnetic resonance imaging of the cervical region would find the knowledge of this morphological variation of trapezius useful in making clinical decisions. Key words: Trapezius, Variation, Morphology, HOX D4, Molecular Received August 19, 2015; Revised January 26, 2016; Accepted February 29, 2016 Introduction fibres pass into an aponeurosis which glides over a smooth triangular surface at the medial end of the scapular spine and Trapezius, a flat triangular muscle, which forms a diamond is attached to a tubercle at the lateral apex [1]. shape with the muscle of the opposite side, helps suspend The present study reports a case of dorsoscapularis tri- the pectoral girdle from the axial skeleton. -

Isolated Metastatic Lesion of the Trapezium
A Case Report & Literature Review Isolated Metastatic Lesion of the Trapezium R. Glenn Gaston, MD, Gary M. Lourie, MD, and C. Cullen Scott, MD and metastases are rare. Their incidence among After surgery, the patient reported marked wrist pain relief. all metastatic lesions is only slightly more than Three months after surgery, she had excellent pain relief, but 0.1%. The distal phalanx is the most commonly overall she continued to decline. Pathology of the excised involved site of hand metastases. Pancarpal trapezium was consistent with metastatic non–small cell Hinvolvement is more common than isolated carpal metas- carcinoma (Figure 3). tases. A solitary carpal metastasis can pose a diagnostic dilemma, as it mimics acute arthritis, osteomyelitis, and DISCUSSION avascular necrosis, and, up to 16% of the time, it may The hand is an uncommon site for metastases. Metastatic be the first indication of a primary cancer elsewhere. An hand lesions represent only 0.1% of all metastatic lesions,1-4 isolated metastatic lesion of the trapezium is reported for though some authors have suggested that this incidence the first time. may be an underrepresentation of the true incidence, as cases may go unnoticed or be subclinical in sick patients.1 CASE REPORT The most common site of hand metastases are the distal A right-hand–dominant woman in her mid-40s, who had phalanges (51%),5 followed by the carpal bones (29.5%)5 a history of active non–small cell lung carcinoma and was and the metacarpals (27.6%).5 Lung carcinoma is the most undergoing chemotherapy, presented with a 3-week history of common primary tumor (40%-52%)5,6 and carries a poor increasing pain at the base of the right thumb. -

Muscles of the Upper Extremity
MUSCLES OF THE UPPER EXTREMITY: Movement of the shoulder and arm: Anterior Axioappendicular Muscles: Pectoralis major O: (clavicular head) medial 1/2 of Clavicle, All fibers : Adducts and medially rotates humerus at Nerves: Lateral and medial pectoral nerves (Sternocostal) Sternum, Anterior suface of shoulder. Also, draws scapula anteriorly and inferiorly Roots: Clavicular (C 5-6), Sternocostal (C 7-8, T1) Ribs 1-6, aponeurosis of External Oblique Clavicular and Sterno fibers : flexes and I: Lateral lip of intertubercular sulcus horizonly adducts humerus. of humerus. Costal fibers : extends humerus. S: Adduction: Latissimus Dorsi, Teres (major & minor), Extension: Posterior deltoid, Latissimus dorsi, Medial rotation: Latissimus Dorsi, Anterior Deltoid, Infraspinatus, Long head Triceps, coracobrachialis teres major, Long head Tricep Teres major, subscapularis A: Abduction: All 3 parts of Deltoid, Supraspinatus, Flexion: Anterior Deltoid, Biceps brachii Lateral rotation: Infraspinatus, Teres minor, coracobrachialis Posterior Deltoid Pectoralis minor O: Anterior superior surface of ribs 3-5 With ribs fixed: Nerve: Medial pectoral nerves sometimes rib 6 Depresses, abducts, downwardly rotate scapula. Roots: (C8 and T1) I: Coracoid process of scapula. With scapula fixed: Elevates 3rd through 5th ribs during forced inspiration. S: Abduction: Serratus Anterior Depression: Lower Trapezius, Serratus anterior Downward rotation: Rhomboid major and minor, Levator scapula, A: Adduction: Romboideus Major and Minor, middle Tapezius Elevation : Upper Trapezius, -

Muscles of the Back Editing File Objectives
Muscles Of The Back Editing File Objectives : At the end of the lecture, students should be able to: • Distinguish between the different groups of back muscles. • Compare between groups of back muscles as regard their nerve supply and action. • List the back muscles of each group. • Describe the attachments of each muscle of the superficial group, as well as, its nerve supply and action. • Describe the triangles of back and their clinical significance. Back Muscles: They are organized into 3 groups: 1- Deep group Intrinsic muscles: Attached to & involved in the movement of Vertebral column &Head. *Develop in the Back *Supplied by Posterior Rami 2- Intermediate group of spinal nerves Attached to Ribs & serve Respiratory Functions. 3- Superficial group Attached to & involved in the movement of Upper limbs. Extrinsic muscles: *Not Developed in the Back *Supplied by Anterior Rami of spinal nerves *Exception within the slides… للتوضيح فقط 1- Deep Group Of Back Muscles: • They extend from sacrum to the base of the skull. • They include extensors* and rotators* of head & vertebral column. So, It is a set of muscles that straighten and rotate the back. • Their tone is responsible for maintenance of normal curvature of vertebral column. • The largest muscle of this group is “erector spinae” which is formed of 3 vertical columns (from lateral to medial): Ilio=ilium , costa= from rib iliocostalis, Longissimus لتسهيل الحفظ : اسمك طويل = لونق اسمس spinalis. (Note the length and attachment of the muscle fibers) Extensor: a muscle whose contraction extends or straightens a limb or other part of the body. Rotator: a muscle whose contraction causes or assists in the rotation of a part of the body. -

Osteoarthritis of the Joints of the Thumb (CMC and STT Arthritis)
Osteoarthritis of the Joints of the Thumb (CMC and STT Arthritis) WHAT IS OSTEOARTHRITIS OF THE CMC AND The most common symptom of osteoarthritis of the STT JOINTS OF THE THUMB? carpometacarpal (CMC) joint or scapho-trapezium/trapezoid (STT) joint, is pain at the bottom of the thumb. Osteoarthritis has been called “joint wear and tear” or “degenerative” arthritis. Osteoarthritis can occur in any joint in The pain can be worse with activities that require pinching, the body but it commonly occurs in the hands and thumbs. such as opening jars, turning door knobs or keys, and writing. If the arthritis progresses you may feel pain at rest and pain at night. In more severe cases, the bottom of the thumb will be bigger and it looks like there is a bump at the bottom end of the thumb. This change can cause stiffness and weakness, making it hard to pick up small objects. The next joint above may compensate by loosening, causing it to bend further back (hyperextension). In healthy joints cartilage, a smooth tissue that covers the ends of the bones, acts as a shock absorber and provides a smooth surface between the bones to allow easy movement. When a joint develops osteoarthritis the cartilage thins and becomes rough. In some cases the cartilage breaks down, leaving the bones unprotected. The joint loses its ability to move smoothly. The bones lose shape and thicken at the end, producing bony spurs (or growths) and pieces of cartilage may break off and float around in the joint. This can disturb other tissues in the joint, causing pain and swelling.