CMC Arthroplasty
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Defining the Morphometrics of the First Metacarpal for the Development of an Osseointegrated Prosthesis
Defining the Morphometrics of the First Metacarpal for the Development of an Osseointegrated Prosthesis Authors: JJ Vaux OMS-IV1, RR Hugate, M.D.2, JW Hills3, RF Grzybowski, D.O.4, CK Funk. Ph.D.1 Affiliations: 1Rocky Vista University College of Osteopathic Medicine, 2Colorado Limb Consultants, 3Dept of Materials and Mechanical Engineering, Denver University, 4Diversified Radiology Objective: Amputation of the thumb presents a serious insult to the hand and can result in up to a 22% loss of functionality in that limb (2,3). To date, several different techniques have been explored for reconstruction of the thumb, however none seem to be incredibly successful (1,4). We believe the answer lies in an osseointegrated prosthesis within the first metacarpal. In order to successfully create an osseointegrated prosthesis, the morphometrics of the first metacarpal are needed. The aim of this study was to define the geometry of the first metacarpal in order to help create a standardized set of stems and prostheses to treat patients who have suffered amputation of the thumb at the level of the first metacarpal phalangeal joint (MCPJ). Methods: A total of eighty first metacarpals from forty-one cadavers were studied. All soft tissues were removed and the first metacarpals were imaged by computed tomography (CT). Three-dimensional models were constructed using cuts from the coronal, sagittal, and axial planes. Using a HyperMesh software, the individual first metacarpals were analyzed and measurements were taken for overall length, radius of curvature, medullary canal diameter, cortical thickness, and distance from the distal end to the center of the isthmus. -

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

The Carpometacarpal Joint of the Thumb: MR Appearance in Asymptomatic Volunteers
Skeletal Radiol (2013) 42:1105–1112 DOI 10.1007/s00256-013-1633-4 SCIENTIFIC ARTICLE The carpometacarpal joint of the thumb: MR appearance in asymptomatic volunteers Anna Hirschmann & Reto Sutter & Andreas Schweizer & Christian W. A. Pfirrmann Received: 23 January 2013 /Revised: 1 April 2013 /Accepted: 21 April 2013 /Published online: 15 May 2013 # ISS 2013 Abstract subjects. The AOL showed a variable SI (36 %/42 % low, Purpose To prospectively characterize the MR appearance 27 %/27 % increased, 36 %/30 % striated). The IML was the of the carpometacarpal (CMC) joint of the thumb in asymp- thickest ligament with a mean of 2.9 mm/3.1 mm and the tomatic volunteers. DRL the thinnest (1.2 mm/1.4 mm). There was a mean Materials and methods Thirty-four asymptomatic volun- dorsal subluxation of 1.8 mm/2.0 mm and radial subluxation teers (17 women, 17 men, mean age, 33.9±9.2 years) of 2.8 mm/3.4 mm of the metacarpal base. The AOL was underwent MR imaging of the thumb after approval by the significantly thicker in men (1.7 mm) than in women local ethical committee. Two musculoskeletal radiologists (1.2 mm; p=0.02). Radial subluxation was significantly independently classified visibility and signal intensity (SI) larger in men (3.4 mm) than in women (2.2 mm; p=0.02). characteristics of the anterior oblique (AOL/beak ligament), No subluxation in palmar or ulnar direction was seen. the posterior oblique (POL), the intermetacarpal (IML), and Conclusions Radial and dorsal subluxation of the CMC the dorsoradial ligaments (DRL) on a three-point Likert joint can be a normal finding in a resting position at MR scale. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -
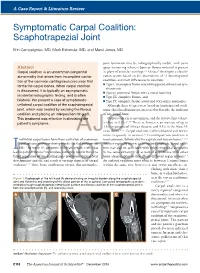
Symptomatic Carpal Coalition: Scaphotrapezial Joint
A Case Report & Literature Review E. Campaigniac et al Symptomatic Carpal Coalition: Scaphotrapezial Joint Erin Campaigniac, MD, Mark Eskander, MD, and Marci Jones, MD joint formation may be radiographically visible, with joint Abstract space narrowing wherein bone or fibrous material is present Carpal coalition is an uncommon congenital in place of articular cartilage.2,4 Minaar8 developed a classifi- abnormality that arises from incomplete cavita- cation system based on his observations of 12 lunotriquetral tion of the common cartilaginous precursor that coalitions and their differences in coalition: ◾ Type I, incomplete fusion resembling pseudarthrosis or syn- forms the carpal bones. When carpal coalition chondrosis is discovered, it is typically an asymptomatic ◾ Type II, proximal fusion with a distal notching incidental radiographic finding, and is often ◾ Type III, complete fusion, and bilateral. We present a case of symptomatic ◾ Type IV, complete fusion associated with other anomalies. unilateral carpal coalition of the scaphotrapezial Although these 4 types were based on lunotriquetral coali- joint, which was treated by excising the fibrous tions, this classification system is used to describe the coalition coalition and placing an interposition fat graft. of any carpal bone. This treatment was effective in alleviating the Carpal coalition is uncommon, and the reported prevalence 2,5,6,9 patient’s symptoms. is close to 0.1%. There is, however, an increase of up to 1.5% in patients of African descent, and 9.5% in the West Af- rican -

Clinical Medical Policy
CLINICAL MEDICAL POLICY Noninvasive Electrical Bone Growth Stimulators Policy Name: (osteogenesis stimulators) Policy Number: MP-070-MD-PA Responsible Department(s): Medical Management Provider Notice Date: 12/15/2018 Issue Date: 01/15/2019 Effective Date: 01/15/2019 Annual Approval Date: 10/17/2019 Revision Date: N/A Products: Gateway Health℠ Medicaid Application: All participating hospitals and providers Page Number(s): 1 of 78 DISCLAIMER Gateway Health℠ (Gateway) medical policy is intended to serve only as a general reference resource regarding coverage for the services described. This policy does not constitute medical advice and is not intended to govern or otherwise influence medical decisions. POLICY STATEMENT Gateway Health℠ may provide coverage under the medical-surgical and DME benefits of the Company’s Medicaid products for medically necessary noninvasive electrical bone growth stimulators as treatment of nonunion long bone fractures or congenital pseudarthrosis. This policy is designed to address medical necessity guidelines that are appropriate for the majority of individuals with a particular disease, illness or condition. Each person’s unique clinical circumstances warrant individual consideration, based upon review of applicable medical records. (Current applicable Pennsylvania HealthChoices Agreement Section V. Program Requirements, B. Prior Authorization of Services, 1. General Prior Authorization Requirements.) Policy No. MP-070-MD-PA Page 1 of 78 DEFINITIONS Prior Authorization Review Panel - A panel of representatives from within the PA Department of Human Services who have been assigned organizational responsibility for the review, approval and denial of all PH-MCO Prior Authorization policies and procedures. Non-invasive (Osteogenic) Electrical Bone Growth Stimulator – A device that uses pulsed- electromagnetic fields, capacitative coupling or combined magnetic fields to generate a weak electric current through the target site. -

중수골 단독 골절에 대한 최소 관혈적 정복술 Mini-Open Reduction Of
Arch Hand Microsurg 2019;24(4):321-329. https://doi.org/10.12790/ahm.2019.24.4.321 Archives of pISSN 2586-3290 • eISSN 2586-3533 Hand and Microsurgery Original Article 중수골 단독 골절에 대한 최소 관혈적 정복술 정연진1ㆍ오세영2ㆍ최지선2ㆍ임진수2ㆍ심형섭2 1가톨릭대학교 의과대학 은평성모병원 성형외과학교실, 2가톨릭대학교 의과대학 성빈센트병원 성형외과학교실 Mini-Open Reduction of Isolated Metacarpal Bone Fracture Yeon Jin Jeong1, Se Young Oh2, Ji Seon Choi2, Jin Soo Lim2, Hyung-Sup Shim2 1Department of Plastic and Reconstructive Surgery, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea 2Department of Plastic and Reconstructive Surgery, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea Purpose: Metacarpal bone fracture is a commonly encountered. The authors applied a minimally invasive open reduction technique that comprises only a stab incision to treat metacarpal bone fractures, thereby minimizing complications that accompany traditional open reduction methods while retaining the advantages of closed reduction techniques. Methods: A 5-year retrospective study was carried out of all patients who underwent surgical treatment performed by two separate hand surgeons. Total 37 patients were operated. Fourteen patients of conventional open reduction group and 23 patients of minimal invasive group were included in the study. Results: Mini-open reduction group had shorter operative time, comparable radiological reduction result, lower subjec- tive pain, comparable mean active range of motion of the metacarpophalangeal joint, similar complication rate and supe- rior outcome scar quality than conventional open reduction group. Conclusion: Mini-open reduction method may be an alternative to conventional open reduction in treating metacarpal fractures. -

Trapezium Prosthetic Arthroplasty (Silicone, Artelon, Metal, and Pyrocarbon)
Trapezium Prosthetic Arthroplasty (Silicone, Artelon, Metal, and Pyrocarbon) Mark A. Vitale, MD, MPHa, Fraser Taylor, MB, BS, FRACSb,c, Mark Ross, MB, BS, FRACSb,c,d, Steven L. Moran, MDe,* KEYWORDS Thumb Trapezial-metacarpal (TM) joint Silicone Artelon Pyrocarbon Total joint arthroplasty KEY POINTS Trapezium prosthetic arthroplasty has been used to treat basal joint arthritis for nearly 5 decades. Implant arthroplasty seeks to preserve joint biomechanics, avoid metacarpal subsidence, and provide immediate stability. There has been rapid development of trapezial prosthetic implants, including synthetic interposition materials, metal total joint arthroplasties and pyrocarbon trapezial arthroplasties. While many recently available implants have been shown to have short-term success, determining the medium- to long-term outcomes require further study. INTRODUCTION method has specific advantages and disadvan- tages for the surgeon to consider. The basal joint of the thumb is the second most 1 In contrast to ablative resection and joint fusion commonly affected joint by arthritis. Degenerative procedures, which sacrifice function of the basal disease of this joint can result in significant pain, joint in an effort to provide pain relief, prosthetic ar- stiffness, weakness, and disability. Conservative throplasty offers the theoretic advantages of pres- measures, such as nonsteroidal anti-inflammatory ervation of normal anatomy and biomechanics. drugs, splinting, and intra-articular corticosteroid This could be accomplished without subsidence injections, can provide relief for some patients; for of the thumb metacarpal, with preservation of those with severe disease in whom nonoperative normal motion at the trapezialmetacarpal (TM) measures fail, many surgical methods are available, joint, prevention of metacarpophalangeal joint with successful outcomes reported in the literature. -

Trapeziectomy
Trapeziectomy What is arthritis of the Trapeziometacarpal symptoms are. You can avoid certain activities joint? that cause you pain or take painkillers. Your The Trapezium is a small wrist bone that lies at hand therapist can provide or make splints for the base of your thumb. It is commonly affected you to rest your thumb in. Your doctor may also by wear and tear, otherwise known as arthritis. inject the joint with steroid (cortisone). This can be done under ultrasound or X-ray guidance Your surgeon has recommended an operation usually on a different day from the outpatient called trapeziectomy. It is the removal of this appointment. The injection only provides bone. However, it is your decision to go ahead temporary relief of symptoms (3-6 months) with the operation or not. or may not be successful at all. Repeated This leaflet gives you information about the injections often last a shorter duration each benefits and risks to help you to make an time. They do not cure the condition. informed decision. If you have any questions Surgical options: this leaflet does not answer, please ask your surgeon or the healthcare team. 1. Trapieziectomy – This is where the bone is removed completely. The gap fills with scar There is more than one way this surgery is tissue on which your thumb will sit to reduce carried out and if you research the internet you the pain of the bone on bone rubbing. will find a lot of information about it, some of 85% of patients have a significant pain which may not be relevant to you. -

Anatomical Snuffbox and It Clinical Significance. a Literature Review
Int. J. Morphol., 33(4):1355-1360, 2015. Anatomical Snuffbox and it Clinical Significance. A Literature Review La Tabaquera Anatómica y su Importancia Clínica. Una Revisión de la Literatura Aladino Cerda*,** & Mariano del Sol ***,**** CERDA, A & DEL SOL, M. Anatomical snuffbox and it clinical significance. A literature review. Int. J. Morphol., 33(4):1355-1360, 2015. SUMMARY: The anatomical snuffbox is a small triangular area situated in the radial part of the wrist, often used to perform clinical and surgical procedures. Despite the frequency with which this area is used, there is scarce information in literature about its details. The objective of this study is detailed knowledge of the anatomical snuffbox’s anatomy and its components, the reported alterations at this portion, besides the clinical uses and significance of this area. KEY WORDS: Hand; Wrist; Anatomical Snuffbox; Radial artery; Cephalic vein; Superficial branch of radial nerve; Scaphoid. INTRODUCTION The anatomical snuffbox (AS) is a depression in (Latarjet & Ruíz-Liard). This triangular structure presents a wrist’s radial part, limited by the tendons of abductor longus base formed by the distal margin of the retinaculum of ex- muscle, extensor pollicis brevis and extensor pollicis longus tensor muscles (Kahle et al., 1995), and a vertex conformed muscles (Latarjet & Ruíz-Liard, 2007). This little triangular by the attachment of the tendons of extensor pollicis longus area is often used to perform clinical procedures as the and extensor pollicis brevis muscles (Fig. 2) (Latarjet & cannulation of the cephalic vein, and surgical procedures as Ruíz-Liard). The roof is formed by the skin and superficial placing arteriovenous fistula between the radial artery and cephalic vein, among other uses. -

DISTAL RADIUS FRACTURES: REHABILITATIVE EVALUATION and TREATMENT PDH Academy Course #OT-1901 | 5 CE HOURS
CONTINUING EDUCATION for Occupational Therapists DISTAL RADIUS FRACTURES: REHABILITATIVE EVALUATION AND TREATMENT PDH Academy Course #OT-1901 | 5 CE HOURS This course is offered for 0.5 CEUs (Intermediate level; Category 2 – Occupational Therapy Process: Evaluation; Category 2 – Occupational Therapy Process: Intervention; Category 2 – Occupational Therapy Process: Outcomes). The assignment of AOTA CEUs does not imply endorsement of specific course content, products, or clinical procedures by AOTA. Course Abstract This course addresses the rehabilitation of patients with distal radius fractures. It begins with a review of relevant terminology and anatomy, next speaks to medical intervention, and then examines the role of therapy as it pertains to evaluation, rehabilitation, and handling complications. It concludes with case studies. Target audience: Occupational Therapists, Occupational Therapy Assistants, Physical Therapists, Physical Therapist Assistants (no prerequisites). NOTE: Links provided within the course material are for informational purposes only. No endorsement of processes or products is intended or implied. Learning Objectives At the end of this course, learners will be able to: ❏ Differentiate between definitions and terminology pertaining to distal radius fractures ❏ Recall the normal anatomy and kinesiology of the wrist ❏ Identify elements of medical diagnosis and treatment of distal radius fractures ❏ Recognize roles of therapy as it pertains to the evaluation and rehabilitation of distal radius fractures ❏ Distinguish -

Arthritis of the Base of the Thumb
Arthritis of the Base of the Thumb What is it? How is the diagnosis made? In a normal joint, cartilage covers the end of the bones and serves as a The diagnosis is made by history and physical evaluation. Pressure and shock absorber to allow smooth, pain-free movement. In osteoarthritis (OA, movement such as twisting will produce pain at the joint. A grinding or “degenerative arthritis”) the cartilage layer wears out, resulting in direct sensation may also be present at the joint (see Figure 3). X-rays are contact between the bones and producing pain and deformity. One of the used to confirm the diagnosis, although symptom severity often does not most common joints to develop OA in the hand is the base of the thumb. correlate with x-ray findings. The thumb basal joint, also called the carpometacarpal (CMC) joint, is a specialized saddle-shaped joint that is formed by a small bone of the wrist What are the treatment options? (trapezium) and the first bone of the thumb (metacarpal). The saddle shaped Less severe thumb arthritis will usually respond to non-surgical care. joint allows the thumb to have a wide range of motions, including up, down, Arthritis medication, splinting and limited cortisone injections may help across the palm, and the ability to pinch (see Figure 1). alleviate pain. A hand therapist might provide a variety of rigid and non-rigid splints which can be used while sleeping or during activities. Figure 1: Thumb Basal Joint Patients with advanced disease or who fail non-surgical treatment may be candidates for surgical reconstruction.