Ukhrul District 2010-11
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Study on Human Rights Violation of Tangkhul Community in Ukhrul District, Manipur
A STUDY ON HUMAN RIGHTS VIOLATION OF TANGKHUL COMMUNITY IN UKHRUL DISTRICT, MANIPUR. A THESIS SUBMITTED TO THE TILAK MAHARASHTRA VIDYAPEETH, PUNE FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN SOCIAL WORK UNDER THE BOARD OF SOCIAL WORK STUDIES BY DEPEND KAZINGMEI PRN. 15514002238 UNDER THE GUIDANCE OF DR. G. R. RATHOD DIRECTOR, SOCIAL SCIENCE CENTRE, BVDU, PUNE SEPTEMBER 2019 DECLARATION I, DEPEND KAZINGMEI, declare that the Ph.D thesis entitled “A Study on Human Rights Violation of Tangkhul Community in Ukhrul District, Manipur.” is the original research work carried by me under the guidance of Dr. G.R. Rathod, Director of Social Science Centre, Bharati Vidyapeeth University, Pune, for the award of Ph.D degree in Social Work of the Tilak Maharashtra Vidyapeeth, Pune. I hereby declare that the said research work has not submitted previously for the award of any Degree or Diploma in any other University or Examination body in India or abroad. Place: Pune Mr. Depend Kazingmei Date: Research Student i CERTIFICATE This is to certify that the thesis entitled, “A Study on Human Rights Violation of Tangkhul Community in Ukhrul District, Manipur”, which is being submitted herewith for the award of the Degree of Ph.D in Social Work of Tilak Maharashtra Vidyapeeth, Pune is the result of original research work completed by Mr. Depend Kazingmei under my supervision and guidance. To the best of my knowledge and belief the work incorporated in this thesis has not formed the basis for the award of any Degree or similar title of this or any other University or examining body. -

Imphal Times Regd.No
Evening daily Imphal Times Regd.No. MANENG /2013/51092 Volume 7, Issue 214, Thursday, March 5, 2020 Maliyapham Palcha kumsing 3418 Rs. 2/- Manipur government serious on COVID-19 29th coronavirus case in India; epidemic; surveillance activities enhanced Maharashtra govt says no need for CM appeals to avoid shaking hands, general public to use face masks By- Raju Vernekar the number of positive cases. the available Active says 24x7 control room open Mumbai, March 5 They include : a) An employee pharmaceutical ingredient working at DSM, Mindspace, (API), to manufacture drugs IT News An employee of Paytm, Madhapur, Hyderabad, who related to treatment would be Imphal, March 5 Gurugram (Haryana), who had returned from Dubai (admitted sufficient for at least two recently returned from a to Gandhi Hospital), b) A 69 months and up to three Following reports on the rise vacation in Italy, tested year Italian and his wife months. In order to maintain of the pandemic Coronavirus positive for coronavirus on admitted to Sawai Mansingh sufficient supply, the across the world, Chief Wednesday taking the total Hospital, Jaipur, Rajasthan, c) government is also Minister N. Biren Singh today number of infected persons in A 45 year old man, who considering to limit the export convened a review meeting India to 29 (16 Italian tourists, recently returned from Italy of 13 essential APIs and with heads of various 13 Indians). The employee has (admitted to the Safdarjung formulations made using departments and government been admitted to the Hospital, Delhi), d) 14 Italian them. officials which are taking up Safardarjung hospital. -

Understanding the Origin of the Terms 'WUNG', 'HAO' and 'TANGKHUL'
International Research Journal of Social Sciences_____________________________________ ISSN 2319–3565 Vol. 3(5), 36-40, May (2014) Int. Res. J. Social Sci. Understanding the Origin of the terms ‘WUNG’, ‘HAO’ and ‘TANGKHUL’ Mawon Somingam Department of Cultural and Creative Studies, North-Eastern Hill University (NEHU) Shillong, Meghalaya, 793022, INDIA Available online at: www.isca.in, www.isca.me Received 7th March 2014, revised 10 th April 2014, accepted 12 th May 2014 Abstract Understanding the origin and meaning of nomenclature of the ‘people’ or term referring to the ‘people’ is as important as identity of the people itself. At times, terms and nomenclatures of the ‘people’ are given by non locals. In the Naga context, the term ‘Naga’ itself is non-local, nomenclature of its federating tribes like Tangkhul is non-local, and names of many Tangkhul villages like Ukhrul, Tushen, Lambui, and Hundung etc. are given by non local administrators, missionaries, anthropologists and neighbouring communities among others. The core focus of the paper is to understand the origin of the terms WUNG, HAO and TANGKHUL. It also brings in the hypothesis of ‘Tangkhul-Meitei Origin’ while attempting to understand the people in brief. One of the main arguments of the paper is that the term HAO is the original or traditional nomenclature of the Tangkhul Nagas. Keywords : Wung, Hao, Tangkhul, Meitei, Christian and People. Introduction “Wung is no longer use today, neither by the people themselves, nor in official transaction” 5. However, it would be wrong to say Though there is no consensus among the local writers and that the term wung is no longer in use today. -
A RECONSTRUCTION of PROTO-TANGKHULIC RHYMES David R
A RECONSTRUCTION OF PROTO-TANGKHULIC RHYMES David R. Mortensen University of Pittsburgh James A. Miller Independent Scholar This paper presents a reconstruction of the rhyme system of Proto-Tangkhulic, the putative ancestor of the Tangkhulic languages, a Tibeto-Burman subgroup. A reconstructed rhyme inventory for the proto-language is presented. Correspondence sets for each of the members of the inventory are then systematically presented, along with supporting cognate sets drawn from four Tangkhulic languages: Ukhrul, Huishu, Kachai, and Tusom. This paper also summarizes the major sound changes that relate Proto-Tangkhulic to the daughter languages on which the reconstruction is based. It is concluded that Proto-Tangkhulic was considerably more conservative than any of these languages. It preserved the Proto-Tibeto-Burman length distinction in certain contexts and reflexes of final *-l, even though these are not preserved as such in Ukhrul, Huishu, Kachai, or Tusom. Proto-Tangkhulic is argued to be a potentially useful source of evidence in the reconstruction of Proto-Tibeto- Burman. Tangkhulic, comparative reconstruction, rhymes, vowel length 1. INTRODUCTION The goal of this paper is to present a preliminary reconstruction of the rhyme system of Proto-Tangkhulic (PT), the ancestor of the Tangkhulic languages of Manipur and contiguous parts of India and Burma. It will show that Proto- Tangkhulic was a relatively conservative daughter language of Proto-Tibeto- Burman, preserving final *-l, and the vowel length distinction (in some contexts), among other features. As such, we suggest that Proto-Tangkhulic has significant importance in understanding the history of Tibeto-Burman. 1.1. The Tangkhulic language family All Tangkhulic languages are spoken in a compact area centered around Ukhrul District, Manipur State, India. -
Mollen Kamsei Primary School Mull
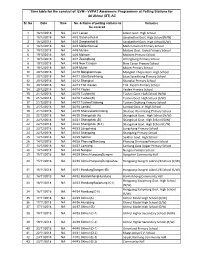
Time table for the conduct of EVM - VVPAT Awareness Programmes at Polling Stations for 44 Ukhrul (ST) AC Sl. No Date Time No. & Name of polling stations to Venue(s) be covered 1 18/12/2018 NA 44/1 Leisan Leisan Govt. High School 2 18/12/2018 NA 44/2 Sanakeithel-A Sanakeithel Govt. High School(N/W) 3 18/12/2018 NA 44/3 Sanakeithel-B Sanakeithel Govt. High School(S/W) 4 18/12/2018 NA 44/4 MollenKamsei Mollen Kamsei Primary School 5 19/12/2018 NA 44/5 Mullam Mullam Govt. Aided Primary School 6 19/12/2018 NA 44/6 Molnom Molnom Primary School 7 19/12/2018 NA 44/7 Zelengbung Zelengbung Primary School 8 19/12/2018 NA 44/8 New Canaan New Canan Primary School 9 19/12/2018 NA 44/9 Muirei Muirei Primary School 10 20/12/2018 NA 44/10 MongkotChepu Mongkot Chepu Govt. High School 11 20/12/2018 NA 44/11 LitanSareikhong Litan Sareikhong Primary School 12 20/12/2018 NA 44/12 Shangkai Shangkai Primary School 13 20/12/2018 NA 44/13 T.M. Kasom T.M. Kasom Primary School 14 20/12/2018 NA 44/14 Yaolen Yaolen Primary School 15 21/12/2018 NA 44/15 Tushen(A) Tushen Govt. High School (N/W) 16 21/12/2018 NA 44/16 Tushen(B) Tushen Govt. High School (S/W) 17 21/12/2018 NA 44/17 TushenChahong Tushen Chahong Primary School 18 21/12/2018 NA 44/18 Lambui Lambui Govt. Jr. -

7112712551213Eokjhjustificati
Consultancy Services for Carrying out Feasibility Study, Preparation of Detailed Project Report and providing pre- Final Alignment construction services in respect of 2 laning of Pallel-Chandel Option Study Report Section of NH- 102C on Engineering, Procurement and Construction mode in the state of Manipur. ALIGNMENT OPTION STUDY 1.1 Prologue National Highways and Infrastructure Development Corporation (NHIDCL) is a fully owned company of the Ministry of Road Transport & Highways (MoRT&H), Government of India. The company promotes, surveys, establishes, design, build, operate, maintain and upgrade National Highways and Strategic Roads including interconnecting roads in parts of the country which share international boundaries with neighboring countrie. The regional connectivity so enhanced would promote cross border trade and commerce and help safeguard India’s international borders. This would lead to the formation of a more integrated and economically consolidated South and South East Asia. In addition, there would be overall economic benefits for the local population and help integrate the peripheral areas with the mainstream in a more robust manner. As a part of the above mentioned endeavor, National Highways & Infrastructure Development Corporation Limited (NHIDCL) has been entrusted with the assignment of Consultancy Services for Carrying out Feasibility Study, Preparation of Detailed Project Report and providing pre-construction services in respect of 2 laning with paved of Pallel-Chandel Section of NH-102C in the state of Manipur. National Highways & Infrastructure Development Corporation Ltd. is the employer and executing agency for the consultancy services and the standards of output required from the appointed consultants are of international level both in terms of quality and adherence to the agreed time schedule. -

MANIPUR Perils of War and Womanhood
MEMORANDUM MANIPUR: PERILS OF WAR AND WOMANHOOD Submitted to: Rashida Manjoo Special Rapporteur on violence against women, its causes and consequences Human Rights Council By: The Civil Society Coalition on Human Rights in Manipur and the UN Imphal 28 April 2013 MANIPUR: PERILS OF WAR AND WOMANHOOD © December 2013 Civil Society Coalition on Human Rights in Manipur and the UN ISBN 978-81-905939-6-0 Email: [email protected] www.humanrightsmanipur.wordpress.com Cover Design: M. James. Mc. Cover Photo: Jansen Lonnquist Back Cover Photo: Human Rights Alert Editorial Team Expert Contribution Nandini Thockchom Thingnam Anjulika Samom Laifungbam Debabrata Roy Sobita Mangsatabam Basantakumar Wareppam Nonibala Narengbam Babloo Loitongbam Hajarimayum Jubita Acknowledgements Manipur: Perils of war and womanhood has benefited from the substantive contribution of Mona Lukram, Lukram Sophy, Wangkheirakpam Shivani, Yengkhom Nonibala, Kangjam Thanilsana, Jiten Yumnam. This document may be freely quoted or cited with due acknowledgement of source Contributory Price: 500 INR/10 USD Printed by MODERN PRESS, M.G. Avenue, Thangal Bazar, Imphal FOREWORD “The death of a woman is not a new act, but the ultimate act in the continuum of violence in the life of the woman.” Rashida Manjoo, UN Special Rapporteur on violence against women 28 April 2013, Imphal Violence against women is one phenomenon of deepest social concern in the growing wave of alarm regarding many forms of violence in our society. The concern is even more significant because, historically and traditionally, gender based violence is accorded zero tolerance amongst the indigenous societies of Manipur. Media reports at the national level of so-called “high-profile cases” pay scant attention to the on- going tragedies of women’s lives across India, particularly among the indigenous and tribal women in remote rural areas where class and development related violent conflicts are played out. -

A Print Version of All the Papers Of
LANGUAGE IN INDIA Strength for Today and Bright Hope for Tomorrow Volume 15:2 February 2015 ISSN 1930-2940 Managing Editor: M. S. Thirumalai, Ph.D. Editors: B. Mallikarjun, Ph.D. Sam Mohanlal, Ph.D. B. A. Sharada, Ph.D. A. R. Fatihi, Ph.D. Lakhan Gusain, Ph.D. Jennifer Marie Bayer, Ph.D. S. M. Ravichandran, Ph.D. G. Baskaran, Ph.D. L. Ramamoorthy, Ph.D. C. Subburaman, Ph.D. (Economics) N. Nadaraja Pillai, Ph.D. Assistant Managing Editor: Swarna Thirumalai, M.A. Materials published in Language in India www.languageinindia.com are indexed in EBSCOHost database, MLA International Bibliography and the Directory of Periodicals, ProQuest (Linguistics and Language Behavior Abstracts) and Gale Research. The journal is listed in the Directory of Open Access Journals. It is included in the Cabell’s Directory, a leading directory in the USA. Articles published in Language in India are peer-reviewed by one or more members of the Board of Editors or an outside scholar who is a specialist in the related field. Since the dissertations are already reviewed by the University-appointed examiners, dissertations accepted for publication in Language in India are not reviewed again. This is our 15th year of publication. All back issues of the journal are accessible through this link: http://languageinindia.com/backissues/2001.html Contents RIP RP: In Search of a More Pragmatic Model for Pronunciation Teaching in the Indian Context ... Anindya Syam Choudhury, Ph.D., PGCTE, PGDTE, CertTESOL (Trinity, London) 1-11 Language in India www.languageinindia.com ISSN 1930-2940 15:2 February 2015 List of Contents i Enhancement of Public Speaking Skill through Practice among Teacher-Trainees in English: A Study .. -

H Geography / / 2003
IMPACT OF JHUM CULTIVATION ON THE ECOSYSTEM OF MANIPUR : A CASE STUDY OF UKHRUL DISTRICT "ABSTRACT f/:^ THESIS SUBMITTED FOR THE AWARD OF THE DEGREE OF IN H GEOGRAPHY / / By MD. BAHAR-UD-DIN SHAH Under the Supervision of Prof. (Mrs.) Abha Lakshmi Singh DEPARTMENT OF GEOGRAPHY ALIGARH MUSLIM UNIVERSITY ALIGARH (INDIA) 2003 ,ov Azad f/,;: 1 As the pressure of population increased, the hunters-cum-cultivators of the Neolithic period started clearing of more patches in forests to bring them under cultivation. At the depletion of fertility, Ihe cultivators used to migrate to new tracts to bum and cleaf forests for sowing of crops. This type of cultivation is termed as 'slash and bum agriculture'.or'shifting cultivation' or 'bush fallow agriculture' or 'swidden agriculture' or ""jhum cultivation'. Jhum cultivation otherwise called 'Pamlou' in Manipur may be defined as an agricultural system which is characterized by rotation of fields rather than crops, by short period of cropping altemating with long fallow periods and clearing by means of slash and burn. It occupies a distinct place in the tribal economy and contributes a vital part of the socio-economic network of tribal life in Manipur and particularly in Ukhml district. This practise of raising agricultural crops does not involve cultivation of land using agricultural implements or draught animals or any mechanical power. The inputs are human labour and seeds. Crops raised for a few seasons and area are abandoned once in 2 or 3 years which are affected by serious erosion. The farmers called J/jwm/a5, then shift over to other lands and resort to similar practise ( but the villages do not shift). -

Women, Peace and Security"
In 2000 the UN Security Council adopted Resolution (UNSCR) 1325 on "Women, Peace and Security". It acknowledges the disproportionate effects of war and conflict on women, as well as the influence women can and must have in prevention and resolution of conflict, and in peace and reconstruction processes. Its main goals are to enhance women's role and decision-making capacities with regard to conflict prevention, conflict resolution and peace building; and to significantly improve factors that directly influence women's security. Finland launched its National Action Plan on the implementation of UNSCR 1325 in 2008. The main objective of this research is to contribute to the understanding of, and provide practical recommendations on, how the Ministry for Foreign Affairs of Finland can: i) Implement Finland's National Action Plan on 1325 through development cooperation, especially its commitment to facilitate women's participation in decision-making in conflict situations, peace processes and post-conflict activities, as well as to protect women in conflicts; ii) Support conflict prevention and post conflict development by strengthening women's role, and empowering women in countries with fragile situations; and; iii) Monitor and measure the Security and Peace Women, progress of such implementation. In addition, the study explored three specific, innovative themes relevant for the question of Women, Peace and Security: i) Involvement of Men; ii) Internally Displaced Persons; and iii) Environment. This study was carried out from April to December 2009 and included case studies in Kenya, Nepal and North-Eastern India, all of which represent countries or areas in diverse and complex conflict and post-conflict situations. -

Manipur State Information Technology Society
MANIPUR STATE INFORMATION TECHNOLOGY SOCIETY (A Government of Manipur Undertaking) 4th Floor, Western Block, New Secretariat, Imphal – 795001 www.msits.gov.in; Email: [email protected] Phone: 0385-24476877 District wise Status of Common Service Centres (As on 25th March, 2013) District: Ukhrul Total No. of CSCs : 33 VSAT Solar Power Sl. CSC Location & VLE Contact District BLOCK CSC Name Name of VLE Installation pack status No Address Number Status 1 Ukhrul Ukhrul CSC-Hundung Hundung K.Y.S Yangmi 9612005006 Installed Installed 2 Ukhrul Chingai CSC-Kalhang Kalhang R.S. Michael (Aphung) 9612765614 / Pending Installed 9612130987 3 Ukhrul Ukhrul CSC-Nungshong Nungshong Khullen Ignitius Yaoreiwung 9862883374 Pending Installed Khullen Chithang 4 Ukhrul Ukhrul CSC-Shangkai Shangkai Chongam Haokip 9612696292 Installed Installed 5 Ukhrul Ukhrul CSC-New Cannon New Cannon ZS Somila 9862826487 / Installed Installed 9862979109 6 Ukhrul Ukhrul CSC-Jessami Jessami Village Nipekhwe Lohe 9862835841 Pending Installed 7 Ukhrul Ukhrul CSC-Teinem Teinem Mashangam Raleng 8730963043 Pending Installed 8 Ukhrul Ukhrul CSC-Seikhor Seikhor L.A. Pamreiphi 9436243204 / Pending Installed 857855919 / 8731929981 9 Ukhrul Chingai CSC-Chingjaroi Chingjaroi Khullen Joyson Tamang 9862992294 Pending Installed Khullen 10 Ukhrul Ukhrul CSC-Litan Litan JS. Aring 9612937524 / Installed Installed 8974425854 / 9436042452 11 Ukhrul Ukhrul CSC-Shangshak Shangshak khullen R.S. Ngaranmi 9862069769 / Pending Installed T.D.Block Khullen 9436086067 / 9862701697 12 Ukhrul Ukhrul CSC-Lambui Lambui L. Seth 9612489203 / Installed Installed T.D.Block 8974459592 / 9862038398 13 Ukhrul Kasom Khullen CSC-Kasom Kasom Khullen Shanglai Thangmeichui 9862760611 / Not approved for Installed T.D.Block Khullen 9612320431 VSAT 14 Ukhrul Kasom Khullen CSC-Khamlang Khamlang N. -
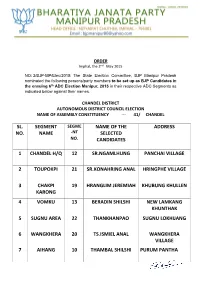
Sl. No. Segment Name Name of the Selected Candidates
ORDER Imphal, the 2nd May 2015 NO: 2/BJP-MP/Elec/2015: The State Election Committee, BJP Manipur Pradesh nominated the following persons/party members to be set up as BJP Candidates in the ensuing 6th ADC Election Manipur, 2015 in their respective ADC Segments as indicated below against their names. CHANDEL DISTRICT AUTONOMOUS DISTRICT COUNCIL ELECTION NAME OF ASSEMBLY CONSTITUENCY --- 41/ CHANDEL SL. SEGMENT SEGME NAME OF THE ADDRESS NO. NAME -NT SELECTED NO. CANDIDATES 1 CHANDEL H/Q 12 SR.NGAMLHUNG PANCHAI VILLAGE 2 TOUPOKPI 21 SR.KONAHRING ANAL HRINGPHE VILLAGE 3 CHAKPI 19 HRANGLIM JEREMIAH KHUBUNG KHULLEN KARONG 4 VOMKU 13 BERADIN SHILSHI NEW LAMKANG KHUNTHAK 5 SUGNU AREA 22 THANKHANPAO SUGNU LOKHIJANG 6 WANGKHERA 20 TS.ISMIEL ANAL WANGKHERA VILLAGE 7 AIHANG 10 THAMBAL SHILSHI PURUM PANTHA 8 PANTHA 11 H.ANGTIN MONSANG JAPHOU VILLAGE 9 SAJIK TAMPAK 23 THANGSUANKAP GELNGAI VILAAGE 10 TOLBUNG 24 THANGKHOMANG AIBOL JOUPI VILLAGE HAOKIP CHANDEL DISTRICT AUTONOMOUS DISTRICT COUNCIL ELECTION NAME OF ASSEMBLY CONSTITUENCY --- 42/ TENGNOUPAL SL. SEGMENT SEGME NAME OF THE ADDRESS NO. NAME -NT SELECTED NO. CANDIDATES 1 KOMLATHABI 8 NG.KOSHING MAYON KOMLATHABI VILLAGE 2 MACHI 2 SK.KOTHIL MACHI VILLAGE, MACHI BLOCK 3 RILRAM 5 K.PRAKASH LANGKHONGCHING VILLAGE 4 MOREH 17 LAMTHANG HAOKIP UKHRUL DISTRICT AUTONOMOUS DISTRICT COUNCIL ELECTION NAME OF ASSEMBLY CONSTITUENCY --- 43/ PHUNGYAR SL. SEGMENT SEGME NAME OF THE ADDRESS NO. NAME -NT SELECTED NO. CANDIDATES 1 GRIHANG 19 SAUL DUIDAND GRIHANG VILLAGE KAMJONG 2 SHINGKAP 21 HENRY W. KEISHING TANGKHUL HUNDUNG 3 KAMJONG 18 C.HOPINGSON KAMJONG BUNGPA KHULLEN 4 CHAITRIC 17 KS.GRACESON SOMI PUSHING VILLAGE 5 PHUNGYAR 20 A.