Insert Document Title
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Europcar Corporate Pack 2012
2012 Business Direct Corporate Package Page 1 TABLE OF CONTENTS EUROPCAR KEY CONTACT DETAILS ......................................................................................................... 3 ABOUT EUROPCAR ....................................................................................................................................... 4 EUROPCAR GROUP VISION, MISSION AND BUSINESS............................................................................ 5 GROUP CORE VALUES ................................................................................................................................. 5 OUR KEY PARTNERSHIPS............................................................................................................................ 6 COMPANY EXPERIENCE............................................................................................................................... 6 PRIVILEGE LOYALTY PROGRAM ................................................................................................................ 7 EUROPCAR SERVICES ................................................................................................................................. 8 OTHER SERVICES.......................................................................................................................................... 8 RENTAL INFORMATION, CONDITIONS AND AUXILIARY COSTS............................................................. 9 PREMIUM LOCATION SURCHARGE (PLS)............................................................................................... -

Avis Australia Commercial Vehicle Fleet and Location Guide
AVIS AUstralia COMMErcial VEHICLES FLEET SHEET UTILITIES & 4WDS 4X2 SINGLE CAB UTE | A | MPAR 4X2 DUAL CAB UTE | L | MQMD 4X4 WAGON | E | FWND • Auto/Manual • Auto/Manual • Auto/Manual • ABS • ABS • ABS SPECIAL NOTES • Dual Airbags • Dual Airbags • Dual Airbags • Radio/CD • Radio/CD • Radio/CD The vehicles featured here should • Power Steering • Power Steering • Power Steering be used as a guide only. Dimensions, carrying capacities and accessories Tray: Tray: are nominal and vary from location 2.3m (L), 1.8m (W) 1.5m (L), 1.5m (W), 1.1m (wheelarch), tub/styleside to location. All vehicles and optional 4X4 SINGLE CAB UTE | B | MPBD 4X4 DUAL CAB UTE | D | MQND 4X4 DUAL CAB UTE CANOPY | Z | IQBN extras are subject to availability. • Auto/Manual • Auto/Manual • Auto/Manual For full details including prices, vehicle • ABS • ABS • ABS availability and options, please visit • Dual Airbags • Dual Airbags • Dual Airbags • Radio/CD • Radio/CD • Radio/CD www.avis.com.au, call 1800 141 000 • Power Steering • Power Steering • Power Steering or contact your nearest Avis location. Tray: Tray: Tray: 1.5m (L), 1.5m (W), 2.3m (L), 1.8m (W) 1.8m (L), 1.8m (W) 0.9m (H) lockable canopy VANS & BUSES DELIVERY VAN | C | IKAD 12 SEATER BUS | W | GVAD LARGE BUS | K | PVAD • Air Con • Air Con • Air Con • Cargo Barrier • Tow Bar • Tow Bar • Car Licence • Car Licence • LR Licence Specs: 5m3 2.9m (L), 1.5m (W), Specs: 12 People Specs: 1.1m (wheelarch) including Driver 20-25 People HITop VAN | H | SKAD 4.2M MovING VAN | F | FKAD 6.4M MovING VAN | S | PKAD 7.3M VAN | V | PQMR • Air Con • Air Con • Air Con • Air Con • Power Steering • Ramp/Lift • Ramp/Lift • Ramp/Lift • Car Licence • Car Licence • MR Licence • MR Licence Specs: 3.7m (L), 1.75m (W), Specs: Specs: Specs: 19m3, 4.2m (L), 34m3, 6.4m (L), 42m3, 7.3m (L), 1.9m (H), between 2.1m (W), 2.1m (H), 2.3m (W), 2.3m (H), 2.4m (W), 2.4m (H), wheel arch 1.35m (L) up to 3 pallets up to 10 pallets up to 12 pallets *Minimum specs. -
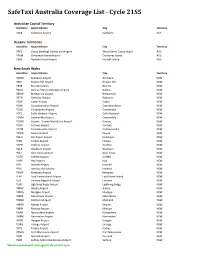
Safetaxi Australia Coverage List - Cycle 21S5
SafeTaxi Australia Coverage List - Cycle 21S5 Australian Capital Territory Identifier Airport Name City Territory YSCB Canberra Airport Canberra ACT Oceanic Territories Identifier Airport Name City Territory YPCC Cocos (Keeling) Islands Intl Airport West Island, Cocos Island AUS YPXM Christmas Island Airport Christmas Island AUS YSNF Norfolk Island Airport Norfolk Island AUS New South Wales Identifier Airport Name City Territory YARM Armidale Airport Armidale NSW YBHI Broken Hill Airport Broken Hill NSW YBKE Bourke Airport Bourke NSW YBNA Ballina / Byron Gateway Airport Ballina NSW YBRW Brewarrina Airport Brewarrina NSW YBTH Bathurst Airport Bathurst NSW YCBA Cobar Airport Cobar NSW YCBB Coonabarabran Airport Coonabarabran NSW YCDO Condobolin Airport Condobolin NSW YCFS Coffs Harbour Airport Coffs Harbour NSW YCNM Coonamble Airport Coonamble NSW YCOM Cooma - Snowy Mountains Airport Cooma NSW YCOR Corowa Airport Corowa NSW YCTM Cootamundra Airport Cootamundra NSW YCWR Cowra Airport Cowra NSW YDLQ Deniliquin Airport Deniliquin NSW YFBS Forbes Airport Forbes NSW YGFN Grafton Airport Grafton NSW YGLB Goulburn Airport Goulburn NSW YGLI Glen Innes Airport Glen Innes NSW YGTH Griffith Airport Griffith NSW YHAY Hay Airport Hay NSW YIVL Inverell Airport Inverell NSW YIVO Ivanhoe Aerodrome Ivanhoe NSW YKMP Kempsey Airport Kempsey NSW YLHI Lord Howe Island Airport Lord Howe Island NSW YLIS Lismore Regional Airport Lismore NSW YLRD Lightning Ridge Airport Lightning Ridge NSW YMAY Albury Airport Albury NSW YMDG Mudgee Airport Mudgee NSW YMER Merimbula -

Queensland Section 2019/20
QUEENSLAND SECTION 2019/20 The furthest corner. The finest care. Providing excellence in, and access to, primary health care and aeromedical services across Queensland for 92 years. 2 The furthest corner. The finest care. The furthest corner. The finest care. Queensland Section | 2019-2020 3 From the Chairman While this year certainly delivered its challenges, I’m pleased to report that the Royal Flying Doctor Service (RFDS) in Queensland has closed the year with solid financial results, thanks to the ongoing commitment of our supporters, additional government funding, the RUSSELL POSTLE – CHAIRMAN resilience of our people and a strong and generous bequest program. COVIDsafe and secure with of pilots, medical officers, nurses, dentists and government support mental health clinicians that are geographically dispersed across our nine bases. When the pandemic was declared in March 2020 we were honoured that by July both the Corporate support building Commonwealth Government and Queensland remains strong Government had turned to the RFDS to help Our six principal partners have been particularly deliver the essential and specialised healthcare supportive over this unprecedented time, all services needed during the pandemic. showing their continued support regardless of the As one of the largest aeromedical retrieval economic impacts being felt in their own sectors. services in the world and with 92 years of serving Thank you to Ergon Energy Retail, QSuper, regional, rural and remote communities of Australia Woolworths, QCoal, Brisbane Airport Corporation, we are well placed to manage infectious diseases. and recent addition RioTinto who this year signed Our staff are well equipped and have the specialist a $1.25 million, five-year partnership with the skills needed to provide the finest care to our RFDS in Queensland. -

Department of State Development, Manufacturing, Infrastructure And
Department of State Development, Manufacturing, Infrastructure and Planning What this report contains For more information This report outlines the structure, tel 13 QGOV (13 74 68) operations, achievements and performance fax 07 3220 6465 of the Department of State Development, [email protected] Manufacturing, Infrastructure and Planning for www.dsdmip.qld.gov.au the 2018–19 financial year. You can provide feedback on the annual report at the Queensland Government Get Involved website at www.qld.gov.au/annualreportfeedback Why we have an The Queensland Government is annual report committed to providing accessible services to Queenslanders from all As well as meeting the statutory requirements culturally and linguistically diverse backgrounds. set out in the Financial Accountability Act 2009 If you have difficulty in understanding the annual and the Financial and Performance Management report, you can contact us on either Standard 2019, the annual report is an important 07 3452 7100 or call the Translating and tool for informing community, industry, government and organisations about our performance and Interpreting Service (TIS National) on telephone future priorities. 131 450 and ask them to contact the Queensland Department of State Development, Manufacturing, Infrastructure and Planning on 07 3452 7100. Accessing the report The annual report is available on the Department of State Development, Manufacturing, Copyright Infrastructure and Planning website at www.dsdmip.qld.gov.au/corporate-publications/ This publication is protected by the Copyright annual-report.html or in hard copy on request. Act 1968. Additional annual reporting requirements have © The State of Queensland (Department of State been published on the Queensland Government Development, Manufacturing, Infrastructure and Open Data portal at https://data.qld.gov.au Planning) 2019. -

New Air Conditioning Design Temperatures for Queensland
New air-conditioning design temperatures for Queensland, Australia by Eric Peterson¹, Nev Williams¹, Dale Gilbert¹, Klaus Bremhorst² ¹Thermal Comfort Initiative of Queensland Department of Public Works, Brisbane ²Professor of Mechanical Engineering, the University of Queensland, St Lucia Abstract : This paper presents results of a detailed analysis of meteorological data to determine air conditioning design temperatures dry bulb and wet bulb for hundreds of locations throughout Queensland, using the tenth-highest daily maximum observed per year. This is a modification of the AIRAH 1997 method that uses only 3PM records of temperature. In this paper we ask the reader to consider Australian Bureau of Meteorology official “climate summaries” as a benchmark upon which to compare various previously published comfort design temperatures, as well as the new design temperatures proposed in the present paper. We see some possible signals from climate change, but firstly we should apply all available historical data to establish outdoor design temperatures that will ensure that cooling plant are correctly sized in the near future. In a case- studies of Brisbane, we find that inner city temperatures are rising, that airport temperatures are not, and that suburban variability is substantially important. Table 1: Air-conditioning design temperatures compared at eight locations 2004 1986 2004 2004 1975 2004 1998 AERO AERO BRISBANE 1939 – 1942 – 1851 – 1939 – 1942 – 1957 – 1950 – 2000 1940 – TOOWOOMBA CAIRNSAERO CHARLEVILLE (EAGLE FARM) ROCKHAMPTON BRISBANE -

Competition Policy and International Airport Services, 1997
Competition Policy and International Airport Services 1997 The OECD Competition Committee debated competition policy and international airport services in June 1997. This document includes an executive summary, an analytical note by the OECD staff and written submissions from Australia, Austria, Canada, the European Commission, Germany, Hungary, Italy, Japan, Korea, Norway, Poland, Sweden, Switzerland, the United Kingdom, the United States and BIAC, as well as an aide-memoire of the discussion. Although airlines have long sought to enter alliances, an important new development in the last decade has been the crystallization of international airline alliances around major airline groupings. The scope and nature of these alliances differ, but there is a tendency towards deeper alliances involving co-operation on all aspects of the airline business. These super-alliances are coming as close to actual mergers as aviation’s Byzantine regulations allow, raising fundamental questions for competition policy-makers and enforcers. Alliances have the potential both to enhance the level and quality of services offered to consumers and to significantly restrict competition. Why do airlines seek to enter such alliances? What are the benefits to the airlines or consumers? How do alliances restrict competition? What is the role played by frequent-flyer programmes and other loyalty schemes? What remedies should competition authorities consider to alleviate the harmful effects of alliances? What is the appropriate role for international co-operation between authorities? Structural Reform in the Rail Industry (2005) Competition Issues in Road Transport (2000) Competition in Local Services (2000) Airlines Mergers and Alliances (1999) Promoting Competition in Postal Services (1999) Unclassified DAFFE/CLP(98)3 Organisation de Coopération et de Développement Economiques OLIS : 07-May-1998 Organisation for Economic Co-operation and Development Dist. -

QUEENSLAND SECTION 2016/17 the Furthest Corner
QUEENSLAND SECTION 2016/17 The furthest corner. The finest care. The furthest corner. The finest care. Providing excellence in primary health care and aeromedical service across Queensland. Contents Letters from the CEO and Chairman .................3 Year in numbers .....................................................6 Our people ..............................................................9 Queensland Fleet .................................................16 Service maps .........................................................18 Funding model ..................................................... 21 Our services ..........................................................23 Case study .............................................................34 Clinical Governance and Training .....................36 Queensland Section | 2016-2017 1 2 The furthest corner. The finest care. From the Chairman The past year has been one of considerable progress for RFDS Queensland Section, as we’ve pursued improvements designed to strengthen and future proof the organisation, while continuing to uphold our high standards of clinical and aviation performance and provide access to vital health care to over MARK GRAY – CHAIRMAN 90,000 people. In October 2016, with the assistance of industry experts This NSQHS accreditation is again an important in the health and aviation markets, Dr John O’Donnell independent and objective benchmark of the high (former CEO of Mater Health) and David Hall (former CEO standards of our patient care across our aeromedical of -

Queensland Section 2018/19
QUEENSLAND SECTION 2018/19 The furthest corner. The finest care. The furthest corner. The finest care. Providing excellence in, and access to, primary health care and aeromedical services across Queensland for 91 years. 2 The furthest corner. The finest care. Queensland Section | 2018-2019 3 RFDS (Queensland Section) 2019 Annual General Meeting Chairman’s Report Over the past year, the Queensland Section of the Royal Flying Doctor Service has made significant progress, and continues to expand its vital role in delivering aeromedical and primary health care services to people in regional, rural and remote parts of the State. MARK GRAY – CHAIRMAN There’s no doubt if our founder, Reverend John There’s no doubt if our founder, Flynn, could see where we are today, he would be proud of how far we have come. From a single Reverend John Flynn, could see leased Qantas plane in Cloncurry in 1928, the where we are today, he would be RFDS has now been recognised as Australia’s proud of how far we have come. most reputable charity for the eighth year in a row, based on its unswerving commitment to delivering Flynn’s original vision – still so relevant today – of a “mantle of safety” for the bush. van under the innovative program we pioneered in 2012 with the support of Q-Coal. As I will be stepping down as Chairman at this year’s Annual General Meeting, I would like to In April last year, we were delighted to welcome reflect briefly on some of the key milestones of His Royal Highness, The Prince of Wales to the last three years and, indeed, the total of five the Cairns base during the Gold Coast years that I have served in this role (including an Commonwealth Games for the dedication of earlier stint from 2011 to 2013). -

Aaa Submission to the Rural and Regional Affairs and Transport References Committee
AAA SUBMISSION TO THE RURAL AND REGIONAL AFFAIRS AND TRANSPORT REFERENCES COMMITTEE Inquiry into the operation, regulation and funding of air route service delivery to rural, regional and remote communities ABOUT THE AUSTRALIAN AIRPORTS ASSOCIATION The Australian Airports Association The AAA represents the interests of The AAA facilitates co-operation among (AAA) is a non-profit organisation that over 380 members. This includes more all member airports and their many and was founded in 1982 in recognition of than 260 airports and aerodromes varied partners in Australian aviation, Australia wide – from the local country whilst contributing to an air transport the real need for one coherent, cohesive, community landing strip to major system that is safe, secure, environmentally consistent and vital voice for aerodromes international gateway airports. responsible and efficient for the benefit of and airports throughout Australia. all Australians and visitors. The AAA also represents more than 120 aviation stakeholders and The AAA is the leading advocate for organisations that provide goods and appropriate national policy relating to services to airports. airport activities and operates to ensure regular transport passengers, freight, and the community enjoy the full benefits of a progressive and sustainable airport 2 industry. CONTENTS EXECUTIVE SUMMARY 2 1 INTRODUCTION 3 2 Impacts of regional services 4 2.1 Social impacts 4 2.2 Economic impacts 5 2.3 Economic contribution of regional airports 7 3 REGIONAL AVIATION SERVICES 9 3.1 Domestic -

KODY LOTNISK ICAO Niniejsze Zestawienie Zawiera 8372 Kody Lotnisk
KODY LOTNISK ICAO Niniejsze zestawienie zawiera 8372 kody lotnisk. Zestawienie uszeregowano: Kod ICAO = Nazwa portu lotniczego = Lokalizacja portu lotniczego AGAF=Afutara Airport=Afutara AGAR=Ulawa Airport=Arona, Ulawa Island AGAT=Uru Harbour=Atoifi, Malaita AGBA=Barakoma Airport=Barakoma AGBT=Batuna Airport=Batuna AGEV=Geva Airport=Geva AGGA=Auki Airport=Auki AGGB=Bellona/Anua Airport=Bellona/Anua AGGC=Choiseul Bay Airport=Choiseul Bay, Taro Island AGGD=Mbambanakira Airport=Mbambanakira AGGE=Balalae Airport=Shortland Island AGGF=Fera/Maringe Airport=Fera Island, Santa Isabel Island AGGG=Honiara FIR=Honiara, Guadalcanal AGGH=Honiara International Airport=Honiara, Guadalcanal AGGI=Babanakira Airport=Babanakira AGGJ=Avu Avu Airport=Avu Avu AGGK=Kirakira Airport=Kirakira AGGL=Santa Cruz/Graciosa Bay/Luova Airport=Santa Cruz/Graciosa Bay/Luova, Santa Cruz Island AGGM=Munda Airport=Munda, New Georgia Island AGGN=Nusatupe Airport=Gizo Island AGGO=Mono Airport=Mono Island AGGP=Marau Sound Airport=Marau Sound AGGQ=Ontong Java Airport=Ontong Java AGGR=Rennell/Tingoa Airport=Rennell/Tingoa, Rennell Island AGGS=Seghe Airport=Seghe AGGT=Santa Anna Airport=Santa Anna AGGU=Marau Airport=Marau AGGV=Suavanao Airport=Suavanao AGGY=Yandina Airport=Yandina AGIN=Isuna Heliport=Isuna AGKG=Kaghau Airport=Kaghau AGKU=Kukudu Airport=Kukudu AGOK=Gatokae Aerodrome=Gatokae AGRC=Ringi Cove Airport=Ringi Cove AGRM=Ramata Airport=Ramata ANYN=Nauru International Airport=Yaren (ICAO code formerly ANAU) AYBK=Buka Airport=Buka AYCH=Chimbu Airport=Kundiawa AYDU=Daru Airport=Daru -

(AAA) - Submission to Commonwealth Budget 2019-20
Department of the Treasury Langton Crescent PARKES ACT 2600 E: [email protected] 1 February 2019 Australian Airports Association (AAA) - Submission to Commonwealth Budget 2019-20 Dear Minister, I am writing to you in relation to the upcoming Commonwealth Budget for 2019-20 and would like to bring the critical issue of regional airport infrastructure funding to your attention. By way of background, the Australian Airports Association (AAA) is the national industry voice for airports in Australia. The AAA represents the interests of more than 340 airports and aerodromes Australia wide – from local country community landing strips to major international gateway airports. The AAA’s members include Adelaide, Brisbane, Cairns, Canberra, Darwin, Gold Coast, Hobart, Perth, Melbourne and Sydney airports. There are a further 150 corporate members who provide goods and services to airports. The Charter of the AAA is to facilitate co-operation among all member airports and their many and varied partners in Australian aviation, whilst maintaining an air transport system that is safe, secure, environmentally responsible and efficient for the benefit of all Australians. In October 2017, the AAA launched its Protect Regional Airports campaign, highlighting the important role regional airports play in this country by supporting exports, providing employment and developing tourism. The campaign also identified a number of the unique challenges regional airports face, including wildlife issues, historic and outdated lighting and poor surfaces. This campaign includes express support and endorsement from several independent third-party organisations, including the Royal Flying Doctors Service (RFDS), Regional Aviation Association of Australia (RAAA), Australian Logistics Council (ALC) and the Australian Local Government Association (ALGA).