Great Orme Tramway 15 September 2009
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The International Light Rail Magazine
THE INTERNATIONAL LIGHT RAIL MAGAZINE www.lrta.org www.tautonline.com JUNE 2017 NO. 954 BLACKPOOL GOES FROM STRENGTH TO STRENGTH Sacramento: New lines and new life for San Jose cars US Congress rejects transit cutbacks Siemens and Bombardier to merge? Strasbourg opens cross-border link The art of track Saving Gent 06> £4.40 Challenges of design The impact and and maintenance legacy of the PCCs 9 771460 832050 Phil Long “A great event, really well organised and the dinner, reception and exhibition space made for great networking time.” Andy Byford – CEO, Toronto Transit Commission MANCHESTER “Once again your team have proved your outstanding capabilities. The content was excellent and the feedback from participants was great.” 18-19 July 2017 Simcha Ohrenstein – CTO, Jerusalem LRT Topics and themes for 2017 include: > Rewriting the business case for light rail investment > Cyber security – Responsibilities and safeguards > Models for procurement and resourcing strategies > Safety and security: Anti-vandalism measures > Putting light rail at the heart of the community > Digitisation and real-time monitoring > Street-running safety challenges > Managing obsolescence > Next-generation driver aids > Wire-free solutions > Are we delivering the best passenger environments? > Composite & materials technologies > From smartcard to smartphone ticketing > Rail and trackform innovation > Traction energy optimisation and efficiency > Major project updates Confirmed speakers include: SUPPORTED BY > Geoff Inskip – Chairman, UKTram > Danny Vaughan – Head -

News Update July 2017
Council of Tramway Museums of Australasia Inc. www.cotma.org.au News Update July 2017 From the Chairman Welcome to our third COTMA News Update for 2017. In this issue we report on the recent FEDECRAIL conference held in Antwerp, Belgium and attended by Warren Doubleday, and the NZ FRONZ conference in Dunedin which I attended. As I write this I am preparing to travel to Melbourne for the COTMA AGM on Tuesday (25 July) and an Executive meeting which will follow. At the Executive meeting we have a number of important issues to discuss, including spare parts - note the references further below to Wellington (trolley bus closure), and PC5 equipment, as well as getting an update on Melbourne W’s and equipment. All member museums will have received an invitation to the AGM and should by now have indicated whether they will be attending. The annual conference of the Federation of Rail Organisations of NZ (FRONZ) was well attended by both railway and tramway groups from around N.Z. and included rail trips on the Taieri Gorge line and on the main line to Oamaru as well as visits to the local Gasworks Museum, the Ocean Beach Railway and Toitu Otago Settlers Museum which includes in its collection former Maryhill Cable car No. 106, Roslyn Electric tram No. 1 (restored at Ferrymead) and Dunedin Trolley bus No 10. The Settlers Museum was the venue for an informative talk about the Dunedin Cable car systems and proposals to set up an operating cable car museum using restored cable cars from Ferrymead. -

A Bibliography of the History of Inland Waterways, Railways and Road
A Bibliography of thethe History of Inland Waterways, Railways andand Road Transport inin thethe BritishBritish Isles,Isles, 19921992 This eighth annual bibliographybibliography follows thethe usualusual format.format. 'Ott.xxxx'`Ott.xxxx' indicates a cross-reference toto anan entry in George Ottley, A bibliographybibliography of British railwayrailway historyhistory (1966) or its Supplement (1988). jt indicatesindicates thatthat aa copycopy ofof thethe bookbook has not beenbeen seenseen and, therefore,therefore, thethe bibliographicalbibliographical details may not be accurate. +1 The continuingcontinuing support ofof the regular contributorscontributors (listed in the introduction to the 1991 Bibliography), whowho searchsearch outout the rarer books and comb through somesome 300300 periodical titles, is gratefully acknowledged.acknowledged. ThanksThanks areare again due to the Ian AllanAllan Bookshop atat Waterloo,Waterloo, the World of Transport Bookshop at Twickenham, and the Inland Waterways Association bookshop for their kind indulgence.indulgence. SECTION GG GENERALGENERAL GB TRANSPORTTRANSPORT AT AT PARTICULAR PARTICULAR PERIODS GB1GBl PrehistoryPrehistory and and RomanRoman ANDERSON, JAMES D.D. RomanRoman militarymilitary supplysupply inin north-eastnorth·east England:England: anan analysisanalysis of and an alternativealternative to the PiereebridgcPiercebridge Formula. Oxford: TemposTempus Reparaturn,Reparatum, 1992.1992. pp.v,196. 2222 p1.,65pI. ,65 figs.figs. [B.[B.A.R. A.R. BritishBritish series, series, no.224.]no.224.) Based on Ph.D. thesis, Univ.of Newcastle upon Tyne. Examines transport by road & natural river, rejectingrejecting as 'unlikely''unlikely' thethe improvedimproved riverriver systemsystem suggestedsuggested inin Raymond Selkirk,Selkirk, The PiercebridgePiercebridge Formula (1983).(1983). GC TRANSPORTTRANSPORT IN IN PARTICULAR PARTICULAR REGIONS REGIONS OF THE BRITISH ISLESISLES GCGClb lb England—SouthEngland-South West West region 2 PERKINS, KEITH S.S. -

Trams Der Welt / Trams of the World 2020 Daten / Data © 2020 Peter Sohns Seite/Page 1 Algeria
www.blickpunktstrab.net – Trams der Welt / Trams of the World 2020 Daten / Data © 2020 Peter Sohns Seite/Page 1 Algeria … Alger (Algier) … Metro … 1435 mm Algeria … Alger (Algier) … Tram (Electric) … 1435 mm Algeria … Constantine … Tram (Electric) … 1435 mm Algeria … Oran … Tram (Electric) … 1435 mm Algeria … Ouragla … Tram (Electric) … 1435 mm Algeria … Sétif … Tram (Electric) … 1435 mm Algeria … Sidi Bel Abbès … Tram (Electric) … 1435 mm Argentina … Buenos Aires, DF … Metro … 1435 mm Argentina … Buenos Aires, DF - Caballito … Heritage-Tram (Electric) … 1435 mm Argentina … Buenos Aires, DF - Lacroze (General Urquiza) … Interurban (Electric) … 1435 mm Argentina … Buenos Aires, DF - Premetro E … Tram (Electric) … 1435 mm Argentina … Buenos Aires, DF - Tren de la Costa … Tram (Electric) … 1435 mm Argentina … Córdoba, Córdoba … Trolleybus … Argentina … Mar del Plata, BA … Heritage-Tram (Electric) … 900 mm Argentina … Mendoza, Mendoza … Tram (Electric) … 1435 mm Argentina … Mendoza, Mendoza … Trolleybus … Argentina … Rosario, Santa Fé … Heritage-Tram (Electric) … 1435 mm Argentina … Rosario, Santa Fé … Trolleybus … Argentina … Valle Hermoso, Córdoba … Tram-Museum (Electric) … 600 mm Armenia … Yerevan … Metro … 1524 mm Armenia … Yerevan … Trolleybus … Australia … Adelaide, SA - Glenelg … Tram (Electric) … 1435 mm Australia … Ballarat, VIC … Heritage-Tram (Electric) … 1435 mm Australia … Bendigo, VIC … Heritage-Tram (Electric) … 1435 mm www.blickpunktstrab.net – Trams der Welt / Trams of the World 2020 Daten / Data © 2020 Peter Sohns Seite/Page -
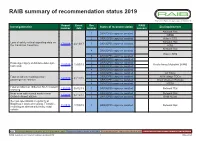
RAIB Summary of Recommendation Status 2019
RAIB summary of recommendation status 2019 Report Event Rec RAIB Investigation title Status of recommendation End implementer number date number concern Network Rail 1 ORR/OPB response awaited RSSB 2 ORR/OPB response awaited Hitachi STS Loss of safety critical signalling data on Network Rail 17/2019 20/10/17 3 ORR/OPB response awaited the Cambrian Coast line RSB Network Rail 4 ORR/OPB response awaited Hitachi STS 5 ORR/OPB response awaited 1 ORR/OPB response awaited Passenger injury at Ashton-under-Lyne 2 ORR/OPB response awaited 15/2019 12/03/19 Keolis Amey Metrolink (KAM) tram stop 3 ORR/OPB response awaited 4 ORR/OPB response awaited 1 ORR/OPB response awaited All TOCs Fatal accident involving a train 2 ORR/OPB response awaited All Heritage TOCs 14/2019 01/12/18 passenger at Twerton 3 ORR/OPB response awaited Great Western Railway 4 ORR/OPB response awaited RSSB Fatal accident at Tibberton No.8 footpath 13/2019 06/02/19 1 ORR/OPB response awaited Network Rail crossing Near miss with a track worker near 1 ORR/OPB response awaited Network Rail 12/2019 02/12/18 Gatwick Airport station 2 ORR/OPB response awaited BAM Nuttall Serious operational irregularity at Bagillt user worked crossing, Flintshire, 11/2019 17/09/19 1 ORR/OPB response awaited Network Rail involving an abnormally heavy road vehicle Key: Recommendations made prior to 2019 that remain open Recommendations made during 2019 Recommendations implemented during 2019 Recommendations where status changed during 2019 RAIB summary of recommendation status 2019 1 May 2020 Report Event -

Catalogue Io7
ROBERT HUMM CATALOGUE IO7 One thousand books old, rore and recent on British ond foreign railways, ond related subjects. Periodicols, Time Tobles, Officiol Publicotionq Box Lots CATALOG UE SUBSCRI PTIONS These catalogues have appeared regularly since 1974. They are the most comprehensive railway book catalogues available in this country, or anywhere else, and the best of our new acquisitions always go into the catalogues first. We try to ensure that each one contains as wide a variety of material as possible, both British and overseas. We also aim to include material to suit all pockets and levels of collecting, with many books in the f,15-f30 range, as well as more expensive and recondite books. Recently frequency of issue has been one or two per year. The regular subscription will continue to bry the next four issues. The initial distribution of each catalogue is by first class post (or airmail overseas) to subscribers only. After a few weeks surplus copies are mailed to a non-subscribers who we think may be interested. If you are a dedicated collector it makes sense to subscribe - you will have the best opportunity to obtain the pick of our latest stock. You can subscribe either to a single issue or to the next two or four issues. Subscription rates are as follows: Great Britain & NI E u rope Rest of the world Next four issues f,l7 f22 f26 Next two issues f9 ft2 ft4 Single issue I,5i- f7 f9 ROBtrRT IIUMM & Co. BOOI(SELLERS 59 Scotgate,.Stamford, Lincolnshire. PE9 2YQ felephone 01 780 7 66266 books@roberthumm. -

THE CIRCULAR Bradford Railway Circle No.351 – 1St Quarter, 2010
THE CIRCULAR Bradford Railway Circle No.351 – 1st Quarter, 2010 Contents Page 1 Editorial 2 Douglas Butterfield – Obituary Frank Robertshaw 5 Ben‟s Bits Ben Burrows 9 Photo Competition 2010 Tom Ickringill 10 Japan – The Land of Rising Water (Pt.2) Michael Wade 11 Meeting Reports Philip Lockwood 13 Cambrian Coast Keith Preston 16 Membership Matters Michael Wade 17 Letter to the Editor 17 RCTS West Riding Indoor Programme 17 Special Traffic Notices 18 More Ben‟s Bits Ben Burrows 23 Secretary‟s Page Peter Holden 24 Circle Diary 2010 24 Small Ads Editorial Welcome to 2010! We now have 350 issues of The Circular under our belts, so here‟s to the next 350. This issue we begin with an obituary of late Honorary Life Member Douglas Butterfield, by his (and our) great friend Frank Robertshaw. Further on, a novelty is possibly the first ever poem in our magazine, written by Keith Preston when inspired by the Welsh landscape. We have liberal helpings of Ben‟s Bits this time, as I had many contributions from Ben that deserve an airing, and few from other members. So, the coffers are fairly empty now (except for a few Outer Circle articles from Geoff Butland, reissued by Frank Robertshaw) – please put pen to paper and keep the magazine going. I had no submissions for cover photos, so we have one from the Editor himself this year. Recent news on BBC Radio we heard that DMUs not being built as quickly as needed, because of problems at Bombardier Derby and also because investors (required to fund new stock) cannot be found due to declining confidence in diesel as an economically viable fuel for the future. -

Bill 2012 Notes on the Bill Volume 4
Statute Law (Repeals) Bill 2012 Notes on the Bill Volume 4 October 2012 STATUTE LAW (REPEALS) BILL 2012 NOTES ON THE BILL CONTENTS VOLUME 4 Page SCHEDULE 1 – REPEALS PART 9 - RAILWAYS Group 2 – Rates and Charges 1179-1225 Group 3 – Miscellaneous 1226-1237 PART 10 - TAXATION AND PENSIONS 1238-1351 Group 1 – General Taxation 1238-1333 Group 2 – Scottish Local Taxation 1334-1349 Group 3 – Personal Accounts Delivery Authority 1350-1351 PART 11 - TURNPIKES 1352-1449 Introduction 1352-1354 Group 1 – Gloucestershire and Oxfordshire 1355-1361 Group 2 – Surrey 1362-1364 Group 3 – London to Holyhead 1365-1449 GROUP 2 - RATES AND CHARGES ___________________________________________________________________ Reference Extent of repeal or revocation ___________________________________________________________________ Liverpool, Crosby, and Southport Railway The whole Act. Amendment Act 1853 (16 & 17 Vict. c.ccxi) Great Eastern Railway Company (Rates The whole Act. and Charges) Order Confirmation Act 1891 (54 & 55 Vict. c.ccxiv) Great Northern Railway Company (Rates The whole Act. and Charges) Order Confirmation Act 1891 (54 & 55 Vict. c.ccxv) London and South Western Railway The whole Act. Company (Rates and Charges) Order Confirmation Act 1891 (54 & 55 Vict. c.ccxvi) London, Brighton, and South Coast Railway The whole Act Company (Rates and Charges) Order Confirmation Act 1891 (54 & 55 Vict. c.ccxvii) London, Chatham, and Dover Railway The whole Act. Company (Rates and Charges) Order Confirmation Act 1891 (54 & 55 Vict. c.ccxviii) Midland Railway Company (Rates and The whole Act. Charges) Order Confirmation Act 1891 (54 & 55 Vict. c.ccxix) South-Eastern Railway Company (Rates The whole Act. and Charges) Order Confirmation Act 1891 (54 & 55 Vict. -

Of RAIB Recommendations
Index of RAIB recommendations Investigation Title Report Event Recommendation Response Status RAIB End Implementer Recommendation(s), status Number Date Number Concern and action taken Freight train derailment at Awaiting Recommendation(s) and Status 02/2021 28/01/20 02/2021/01 None Network Rail Eastleigh, Hampshire Response Report: Eastleigh Freight train derailment at Awaiting Recommendation(s) and Status 02/2021 28/01/20 02/2021/02 None Network Rail Eastleigh, Hampshire Response Report: Eastleigh Person struck by a train at Awaiting Department for Recommendation(s) and Status Eden Park station, south-east 01/2021 26/02/20 01/2021/01 None Response Transport Report: Eden Park London Person struck by a train at Awaiting Recommendation(s) and Status Eden Park station, south-east 01/2021 26/02/20 01/2021/01 None Network Rail Response Report: Eden Park London Person struck by a train at Awaiting Department for Recommendation(s) and Status Eden Park station, south-east 01/2021 26/02/20 01/2021/02 None Response Transport Report: Eden Park London Person struck by a train at Awaiting Recommendation(s) and Status Eden Park station, south-east 01/2021 26/02/20 01/2021/02 None Network Rail Response Report: Eden Park London Person struck by a train at Awaiting Recommendation(s) and Status Eden Park station, south-east 01/2021 26/02/20 01/2021/03 None Rail Delivery Group Response Report: Eden Park London Person struck by a train at Awaiting Office of Rail and Recommendation(s) and Status Eden Park station, south-east 01/2021 26/02/20 01/2021/04 None -

Railway Correspondence & Travel Society
The R.C.T.S. is a Charitable Incorporated Organisation registered with The Charities Commission Registered No. 1169995. THE RAILWAY CORRESPONDENCE AND TRAVEL SOCIETY PHOTOGRAPHIC LIST LIST 9 - MISCELLANEOUS SUBJECTS (INCLUDING RAILWAY COATS OF ARMS) JULY 2019 The R.C.T.S. is a Charitable Incorporated Organisation registered with The Charities Commission Registered No. 1169995. www.rcts.org.uk VAT REGISTERED No. 197 3433 35 R.C.T.S. PHOTOGRAPHS – ORDERING INFORMATION The Society has a collection of images dating from pre-war up to the present day. The images, which are mainly the work of late members, are arranged in in fourteen lists shown below. The full set of lists covers upwards of 46,900 images. They are : List 1A Steam locomotives (BR & Miscellaneous Companies) List 1B Steam locomotives (GWR & Constituent Companies) List 1C Steam locomotives (LMS & Constituent Companies) List 1D Steam locomotives (LNER & Constituent Companies) List 1E Steam locomotives (SR & Constituent Companies) List 2 Diesel locomotives, DMUs & Gas Turbine Locomotives List 3 Electric Locomotives, EMUs, Trams & Trolleybuses List 4 Coaching stock List 5 Rolling stock (other than coaches) List 6 Buildings & Infrastructure (including signalling) List 7 Industrial Railways List 8 Overseas Railways & Trams List 9 Miscellaneous Subjects (including Railway Coats of Arms) List 10 Reserve List (Including unidentified images) LISTS Lists may be downloaded from the website http://www.rcts.org.uk/features/archive/. PRICING AND ORDERING INFORMATION Prints and images are now produced by ZenFolio via the website. Refer to the website (http://www.rcts.org.uk/features/archive/) for current prices and information. NOTES ON THE LISTS 1. -

AARON, Professor Richard Ithamar
NLW MSS 22853-23691 (2) Index AARON, Professor Richard Ithamar. Letter from (1961), 23416, f. 1. 'AB IORWERTH'. see Roberts, Jonah. 'AB ITHEL'. see Williams, John. 'AB MYRDDIN'. see Edwards, Edward. ABADAM, Edward, Middleton Hall, co. Carmarthen. Book-plate of (1865), 23148, f. 11. ABBEY CONSOLS MINES, co. Cardigan. Refs to (1856-9), 23159, ff. 25v-47v passim. ABBEY CWM-HIR. Tour (1910), 23218, pp. 114-15. ABBEYS. Abbotsbury, aquatint of (c. 1811), 23401, f. 41. Basingwerk, ref. to (1796), 23253, ff. 96v-7. Combermere, engraving of (1828), 23302, f. 24v. Cymer, list of plants at (1855), 23304, f. 16. Dryburgh, water-colour of (1805), 22983, f. 74. Evesham, fragment of missal from (15 cent.), 22857, ff. 1-2. La Boissière, diocese of Angers, MS from (1610), 23205. Llanthony, description of (1810), 23218, pp. 121-2, 149. Nashdom, co. Buckingham, letters from (1927-32), 23190, ff. 17, 24-7, 29-32v, 34, 36-9. Neath, description of (1796), 23253, f. 30. Shrewsbury, description of (1859), 23065, f. 77. Shrewsbury, engravings of (1856), 23065, f. 76v. Strata Florida, accounts rel. to (1887-90), 23159, ff. 210, 220v-1, 225v, 231v. Tintern, description of (1796), 23253, ff. 5, 7. Tintern, description of (1844), 23063, ff. 90v-1. Tintern, description of (1859), 23065, f. 15. Tintern, engravings of (early 19 cent.), 23401, f. 41. Tintern, engravings of (1842-1850s), 23065, f. 14v. Valle Crucis, description of (1778), 22967, ff. 12-13. Valle Crucis, description of (1796), 23253, ff. 109-10. Valle Crucis, description of (1810), 23218, pp. 103-4. Valle Crucis, description of (1837), 23062, pp. -
Report on the Value of Heritage Railways
All Party Parliamentary Group on Heritage Rail Report on the Value of Heritage Railways July 2013 1 Members conducting the oral evidence sessions House of Commons: Mark Garnier MP (Con) - Chair Susan Elan Jones MP (Lab) -Vice-Chair Martin Vickers MP (Con) - Vice-Chair Nigel Mills MP (Con) Nicky Morgan MP (Con) Helen Goodman MP (Lab) Robert Goodwill MP (Con) Andrew Selous (Con) Richard Bacon (Con) (Research Assistants to Rt Hon Patrick McLoughlin MP and Norman Lamb MP also attended a session.) House of Lords: Lord Grocott (Lab) - Vice-Chair Lord Faulkner of Worcester (Lab) - Vice-Chair Lord Snape (Lab) Lord Wigley (Plaid Cymru) Secretariat: Chris Austin, OBE - Secretary 2 PART ONE – KEY RECOMMENDATIONS AND EXECUTIVE SUMMARY Key recommendations. The Group has made six key recommendations as a result of this inquiry: FOR GOVERNMENT 1. Planning Law. Heritage railways should be able to benefit from the same permitted development rights as Network Rail does on the national network. We believe guidance is needed to prevent over-zealous interpretation of planning legislation and regulation stifling development of heritage railways. 2. Railway extensions. The requirements for a Transport & Works Act Order for modest extensions to heritage lines should be simplified, possibly using an on-line proforma application process. 3. Sponsorship. The Department for Transport should take the lead sponsorship role on policies affecting heritage railways. The Department for Culture, Media and Sport should remain responsible for policy on tourism issues and the Department for Business, Innovation and Skills for apprenticeships, training and development. FOR LOCAL AUTHORITIES 4. Public Transport. There is scope to provide a public transport service on some heritage railways and a „public tourist service‟ on some others which should 3 be further developed and encouraged.