A Pilot Study in Detoxification of Heavy Metals
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chelation Therapy
Medical Policy Chelation Therapy Table of Contents • Policy: Commercial • Coding Information • Information Pertaining to All Policies • Policy: Medicare • Description • References • Authorization Information • Policy History Policy Number: 122 BCBSA Reference Number: 8.01.02 NCD/LCD: N/A Related Policies None Policy Commercial Members: Managed Care (HMO and POS), PPO, and Indemnity Medicare HMO BlueSM and Medicare PPO BlueSM Members Chelation therapy in the treatment of the following conditions is MEDICALLY NECESSARY: • Extreme conditions of metal toxicity • Treatment of chronic iron overload due to blood transfusions (transfusional hemosiderosis) or due to nontransfusion-dependent thalassemia (NTDT) • Wilson's disease (hepatolenticular degeneration), or • Lead poisoning. Chelation therapy in the treatment of the following conditions is MEDICALLY NECESSARY if other modalities have failed: • Control of ventricular arrhythmias or heart block associated with digitalis toxicity • Emergency treatment of hypercalcemia. NaEDTA as chelation therapy is considered NOT MEDICALLY NECESSARY. Off-label applications of chelation therapy are considered INVESTIGATIONAL, including, but not limited to: • Alzheimer’s disease • Arthritis (includes rheumatoid arthritis) • Atherosclerosis, (e.g., coronary artery disease, secondary prevention in patients with myocardial infarction, or peripheral vascular disease) • Autism • Diabetes • Multiple sclerosis. 1 Prior Authorization Information Inpatient • For services described in this policy, precertification/preauthorization IS REQUIRED for all products if the procedure is performed inpatient. Outpatient • For services described in this policy, see below for products where prior authorization might be required if the procedure is performed outpatient. Outpatient Commercial Managed Care (HMO and POS) Prior authorization is not required. Commercial PPO and Indemnity Prior authorization is not required. Medicare HMO BlueSM Prior authorization is not required. -

Chelation Therapy
Corporate Medical Policy Chelation Therapy File Name: chelation_therapy Origination: 12/1995 Last CAP Review: 2/2021 Next CAP Review: 2/2022 Last Review: 2/2021 Description of Procedure or Service Chelation therapy is an established treatment for the removal of metal toxins by converting them to a chemically inert form that can be excreted in the urine. Chelation therapy comprises intravenous or oral administration of chelating agents that remove metal ions such as lead, aluminum, mercury, arsenic, zinc, iron, copper, and calcium from the body. Specific chelating agents are used for particular heavy metal toxicities. For example, desferroxamine (not Food and Drug Administration [FDA] approved) is used for patients with iron toxicity, and calcium-ethylenediaminetetraacetic acid (EDTA) is used for patients with lead poisoning. Note that disodium-EDTA is not recommended for acute lead poisoning due to the increased risk of death from hypocalcemia. Another class of chelating agents, called metal protein attenuating compounds (MPACs), is under investigation for the treatment of Alzheimer’s disease, which is associated with the disequilibrium of cerebral metals. Unlike traditional systemic chelators that bind and remove metals from tissues systemically, MPACs have subtle effects on metal homeostasis and abnormal metal interactions. In animal models of Alzheimer’s disease, they promote the solubilization and clearance of β-amyloid protein by binding to its metal-ion complex and also inhibit redox reactions that generate neurotoxic free radicals. MPACs therefore interrupt two putative pathogenic processes of Alzheimer’s disease. However, no MPACs have received FDA approval for treating Alzheimer’s disease. Chelation therapy has also been investigated as a treatment for other indications including atherosclerosis and autism spectrum disorder. -
Recognizing and Managing Lead and Mercury Poisonings
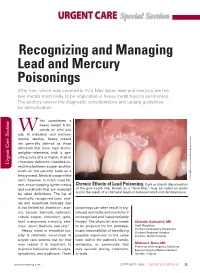
URGENT CARE Special Section Recognizing and Managing Lead and Mercury Poisonings After iron, which was covered in EM’s May issue, lead and mercury are the two metals most likely to be implicated in heavy metal toxicity syndromes. The authors review the diagnostic considerations and update guidelines for detoxification. hat constitutes a heavy metal? It de- W pends on who you ask. In industrial and environ- mental studies, heavy metals are generally defined as those elements that have high atomic weights—elements with a spe- cific gravity of 5 or higher. A strict chemistry definition classifies ev- Urgent Care Section Urgent Care erything between copper and bis- muth on the periodic table as a heavy metal. Medical usage of the term, however, is much more lib- Inc Researchers, Associates/Photo © 2009 Biphoto eral, encompassing lighter metals Chronic Effects of Lead Poisoning. Dark or bluish discoloration and metalloids that are excluded of the gum-tooth line, known as a “lead line,” may be noted on exam and is the result of a chemical reaction between lead and dental plaque. by other definitions. The list of medically recognized toxic met- als and metalloids includes (but is not limited to) aluminum, arse- poisonings can often result in sig- nic, barium, bismuth, cadmium, nificant morbidity and mortality if cobalt, copper, chromium, gold, unrecognized and inappropriately lead, manganese, mercury, sele- treated. The physician also needs Christian Balmadrid, MD nium, silver, thallium, and zinc.1 to be prepared for the postdiag- Staff Physician Heavy metal or metalloid tox- nostic responsibility of identifying Durham Emergency Physicians Durham Regional Hospital icity is relatively uncommon in possible exposures to the same Durham, North Carolina urgent care centers, but for that toxin within the patient’s family, very reason it is important to workplace, or community that Michael J. -

Managing Pet Bird Toxicoses J.A
birdtoxic.qxd 6/15/01 4:56 PM Page 23 CLINICIAN’S NOTEBOOK Managing Pet Bird Toxicoses J.A. RICHARDSON, L.A. MURPHY S.A. KHAN AND C. MEANS J.A. Richardson, DVM, Dipl ACFE L.A. Murphy, VMD S.A. Khan, DVM, PhD C. Means, DVM ASPCA Animal Poison Control Center 1717 South Philo Road Suite 36 Urbana, Illinois 61802 [email protected] Jill Richardson received her DVM degree from Tuskegee University in 1994. In 1996, following experience in small animal practices in Tennessee and West Virginia, Dr. Richardson joined the ASPCA Animal Poison Control BIRDS ARE CURIOUS BY NATURE, AND SOME HAZARDOUS OBJECTS Center as a Veterinary Poison may be attractive to them. Birds with free household access are more likely to Information Specialist. be exposed to toxicants. Sources of Toxicoses Affecting Pet Birds Reported to the APCC* 11% 27% 12% Pesticides Cleaning products Acknowledgements Plants Medicines The authors would like to thank 25% 25% Harold and Joyce Hamilton, Other, including heavy metals Cindy Dorner, Morgan Wilson, and Information collected between January 1996 - December 2000. Dr. Tracei Holder and the entire staff of the Animal Emergency Clinic of Champaign County. *The ASPCA Animal Poison Control Center, an operating division of the American Society for Photos: Tom Schaefges Photography the Prevention of Cruelty to Animals (ASPCA), is the only animal-oriented poison control Sidney, Illinois center in North America. It is a unique, emergency hotline providing 24-hour-a-day, [email protected] 7-day-a-week telephone assistance. The Center’s hotline veterinarians can quickly answer questions about toxic chemicals, dangerous plants, products or substances found in everyday surroundings that can prove poisonous or fatal to animals. -

Medical Toxicologists Determine Chelation Therapy Rarely Necessary
Medical Toxicologists Determine Chelation Therapy Rarely Necessary Experts from the American College of Medical Toxicology, the Centers for Disease Control, the Agency for Toxic Substances and Disease Registry, and others met at the CDC to review the current use and misuse of chelation therapy in the United States for the treatment of metal poisoning. It was concluded that incorrect diagnosis of metal poisoning is common, and inappropriate use of chelation therapy is widespread. Phoenix, Arizona (PRWEB) March 30, 2012 -- Medical toxicologists and scientific experts speaking at a recent conference at the Centers for Disease Control in Atlanta criticized the widespread misdiagnosis of poisoning from lead, arsenic, mercury and other metals, and called for strong efforts to decrease the inappropriate use of metal chelation therapy. Chelating agents are medications that may be given to patients to increase elimination of metals from the body. Traditionally chelating agents have been used to treat acute poisoning following a large exposure to a metal such as arsenic, mercury, or lead. In recent years, the administration of chelating agents by some health providers has increased. Although chelating agents such as calcium EDTA, DMSA, and DMPS are medications intended to be prescribed by licensed physicians, they are often sold to patients by health care practitioners or obtained without a prescription over the internet, possibly in violation of federal regulations. It has been estimated that nearly 200,000 people may be treated with chelating agents each year in the United States. These patients are frequently diagnosed with chronic metal poisoning based on a poorly documented environmental exposure, vague clinical findings, and inappropriate diagnostic testing. -

Role of the Intensive Care Unit in the Management of the Poisoned Patient Per Kulling and Hans Persson Swedish Poison Information Centre, Stockholm
Concepts in Toxicology Review Medical Toxicology I: 375·386 (1986) 0112·5966/0090·0375/$06.00/0 © ADIS Press Limited All rights reserved. Role of the Intensive Care Unit in the Management of the Poisoned Patient Per Kulling and Hans Persson Swedish Poison Information Centre, Stockholm Summary By applying a sensible toxicological approach to the general principles ofintensive care, an optimum setting for the treatment ofpoisoning is created. The intensive care unit (ICU) can perform the necessary close observation and monitoring, and thus facilitate rapid detection ofsymptoms, and the institution of early appropriate treatment. Diagnosis may be complex in poisoning and require continuous qualified interpretation of clinical and analytical data. Antidote therapy and treatment to enhance elimination ofthe poison must often be dealt with under careful supervision. The capacity ofthe ICU to counteract various toxic effects in a nonspecific way and to provide optimum symptomatic and supportive care is crucial. However, the ongoing toxic effects on the body must always be considered and allowed to guide symptomatic treatment. Thus, clinical toxicology appears to be a specialised branch of intensive care medicine. Many patients exposed to a poison may, after is of utmost importance for a proper interpretation initial measures like clinical assessment, gastric of clinical and analytical data and an immediate lavage and administration of activated charcoal, be start for necessary therapy. In some cases the ICU managed in general wards. However, to be able to may have a laboratory of its own, offering rapid adequately treat a severely poisoned patient the fa and frequent analysis. Another important aspect of cilities of an intensive care unit (ICU) are often the ICU is that there is generally a low threshold required and the capacity of such units to provide for accepting and utilising new and advanced ther optimum conditions for diagnosis and treatment apeutic methods. -

Uranium Toxicity and Chelation Therapy
Pure Appl. Chem. 2014; 86(7): 1105–1110 Conference paper Glen D. Lawrence*, Kamalkumar S. Patel and Aviva Nusbaum Uranium toxicity and chelation therapy Abstract: Uranium toxicity has been a concern for more than 100 years. The toxicology of many forms of uranium, ranging from dust of several oxides to soluble uranyl ion, was thoroughly studied during the Man- hattan Project in the United States in the 1940s. The development of depleted uranium kinetic penetrators as armor-piercing incendiary weaponry produced a novel form of uranium environmental contamination, which led to greater susceptibility to the adverse health effects of the toxic heavy metal after its use in various military conflicts. The aerosol from burning uranium penetrator fragments is rapidly dissolved in biological fluids and readily absorbed from the lungs, leading to a wide range of toxic effects. We have studied some chelating agents for uranyl ion, including citrate ion and desferal (desferrioxamine B), which may be effective for minimizing the toxic effects of this insidious heavy metal. Some characteristics of the desferrioxamine complex are presented, along with information about the use of citrate as an effective chelating agent for therapy of uranium toxicity. Keywords: bioactivity; environmental chemistry; IUPAC Congress-44; metal complexes; solubility; toxi- cology; uranium. DOI 10.1515/pac-2014-0109 Introduction Uranium is the heaviest naturally occurring element in the earth’s crust; it is more abundant than gold or silver. Although discovered in 1789, it found few commercial uses for a century and a half beyond its use as a coloring agent for pottery and glass. Radioactivity was first discovered in uranium in 1896, soon after the discovery of X-rays. -

Chelation Therapy: Stepping Into the Next 60 Years a Historical Commentary
Published in The Townsend Letter , April 2013 Reprinted with Permission, All Rights Reserved Chelation Therapy: Stepping Into the Next 60 Years A Historical Commentary John Parks Trowbridge M. D., FACAM Diplomate, American Board of Clinical Metal Toxicology “Mind-body medicine,” a term well known in medicine, has major roots in observations made in the 1960s by one of my lab directors at Stanford, George Solomon, M.D. Intensive study of the “relaxation response,” “healing touch,” “acupuncture,” and similar “soft science” technologies has led to widespread acceptance in the medical and lay communities. At about the same time, startling observations were being made of reversals of increasingly prevalent coronary and peripheral vascular maladies by chelation therapy with intravenous EDTA. Despite “hard science” showing that these beneficial discoveries have been replicated time and again, chelation remains largely unknown or, at worst, vigorous defiled. Paul Dudley White, M.D., President Eisenhower’s cardiologist, encountered similar resistance for over two decades to his introduction of the EKG. Laënnec was more fortunate in securing wide acceptance of the scientific results available with his new “stethoscope” within a decade in the early 1800s. Given a world increasingly aware of pollution with toxic heavy metals, and given a population with younger onset of serious degenerative diseases, and given 60 years of overwhelmingly successful results, why have conventional medicine and regulatory government tossed chelation aside, onto the trash heap of so-called fraudulent diversions? Going to the Dogs – and Nowhere Else? What we now unquestionably call “modern medicine” was largely invented since the late 1940s. Houston cardiovascular surgeon Denton Cooley, M.D., studied pediatric procedures in post-war Europe and his research efforts have saved countless children. -

Contamination of Drinking-Water by Arsenic in Bangladesh: a Public Health Emergency Allan H
Contamination of drinking-water by arsenic in Bangladesh: a public health emergency Allan H. Smith,1 Elena O. Lingas,2 & Mahfuzar Rahman3 The contamination of groundwater by arsenic in Bangladesh is the largest poisoning of a population in history, with millions of people exposed. This paper describes the history of the discovery of arsenic in drinking-water in Bangladesh and recommends intervention strategies. Tube-wells were installed to provide ‘‘pure water’’ to prevent morbidity and mortality from gastrointestinal disease. The water from the millions of tube-wells that were installed was not tested for arsenic contamination. Studies in other countries where the population has had long-term exposure to arsenic in groundwater indicate that 1 in 10 people who drink water containing 500 mg of arsenic per litre may ultimately die from cancers caused by arsenic, including lung, bladder and skin cancers. The rapid allocation of funding and prompt expansion of current interventions to address this contamination should be facilitated. The fundamental intervention is the identification and provision of arsenic-free drinking water. Arsenic is rapidly excreted in urine, and for early or mild cases, no specific treatment is required. Community education and participation are essential to ensure that interventions are successful; these should be coupled with follow-up monitoring to confirm that exposure has ended. Taken together with the discovery of arsenic in groundwater in other countries, the experience in Bangladesh shows that groundwater sources throughout the world that are used for drinking-water should be tested for arsenic. Keywords: Bangladesh; arsenic poisoning, prevention and control; arsenic poisoning, therapy; water pollution, chemical, prevention and control; water treatment; environmental monitoring. -

8.01.535 Chelation Therapy BCBSA Ref
MEDICAL POLICY – 8.01.535 Chelation Therapy BCBSA Ref. Policy: 8.01.02 Effective Date: May 1, 2021 RELATED MEDICAL POLICIES: Last Revised: April 1, 2021 None Replaces: 8.01.02 Select a hyperlink below to be directed to that section. POLICY CRITERIA | DOCUMENTATION REQUIREMENTS | CODING RELATED INFORMATION | EVIDENCE REVIEW | REFERENCES | HISTORY ∞ Clicking this icon returns you to the hyperlinks menu above. Introduction Chelation is a process to remove certain heavy metals from the blood. In this treatment, a chemical solution is injected into the bloodstream or taken by mouth. Molecules then bind to heavy metals and/or minerals. The heavy metals are then cleared out of the body through urination. Chelation therapy has been studied and approved by the Food and Drug administration to treat certain conditions. This includes removing dangerously high levels of iron, as well as lead or mercury. Thinking that the process of chelation could also remove the buildup of some other substances in the body, some doctors have tried to use it to try to treat other conditions. Examples of these other conditions include Alzheimer disease, autism, diabetes, and plaque inside of arteries (atherosclerosis). Scientific research has not proven that using chelation therapy treatment for these or other conditions is effective. For this reason, chelation therapy for many conditions is considered investigational (unproven). Note: The Introduction section is for your general knowledge and is not to be taken as policy coverage criteria. The rest of the policy uses specific words and concepts familiar to medical professionals. It is intended for providers. A provider can be a person, such as a doctor, nurse, psychologist, or dentist. -

CHELATION THERAPY for NON-OVERLOAD CONDITIONS Policy Number: REHABILITATION 015.25 T1 Effective Date: May 1, 2018
UnitedHealthcare® Oxford Clinical Policy CHELATION THERAPY FOR NON-OVERLOAD CONDITIONS Policy Number: REHABILITATION 015.25 T1 Effective Date: May 1, 2018 Table of Contents Page Related Policy INSTRUCTIONS FOR USE .......................................... 1 Omnibus Codes CONDITIONS OF COVERAGE ...................................... 1 BENEFIT CONSIDERATIONS ...................................... 1 COVERAGE RATIONALE ............................................. 2 APPLICABLE CODES ................................................. 2 DESCRIPTION OF SERVICES ...................................... 3 CLINICAL EVIDENCE ................................................. 3 U.S. FOOD AND DRUG ADMINISTRATION .................... 5 REFERENCES ........................................................... 6 POLICY HISTORY/REVISION INFORMATION ................. 7 INSTRUCTIONS FOR USE This Clinical Policy provides assistance in interpreting Oxford benefit plans. Unless otherwise stated, Oxford policies do not apply to Medicare Advantage members. Oxford reserves the right, in its sole discretion, to modify its policies as necessary. This Clinical Policy is provided for informational purposes. It does not constitute medical advice. The term Oxford includes Oxford Health Plans, LLC and all of its subsidiaries as appropriate for these policies. When deciding coverage, the member specific benefit plan document must be referenced. The terms of the member specific benefit plan document [e.g., Certificate of Coverage (COC), Schedule of Benefits (SOB), and/or Summary -

Table of Contents
____________________________________________________________________________________________________ Subject Chemistry Paper No and Title 15. Bioinorganic Chemistry Module No and Title 4. Toxicity and chelation therapy Module Tag CHE_P15_M4 TABLE OF CONTENTS 1. Learning Outcomes 2. Toxicity 3. Toxic metals 3.1 Mercury 3.2 Cadmium 3.3 Lead 4. Use of chelating agents in medicine; or chelation therapy 5. Summary CHEMISTRY PAPER No. : TITLE MODULE No. : TITLE ____________________________________________________________________________________________________ 1. Learning Outcomes After studying this module, you shall be able to • Know the mechanism of the toxicity of various metals in our body. • Identify the toxic metals, their toxic effects and the reason for their toxicity. • Learn about the chelating therapy and the criteria of a potential chelating drug. • Know about the various chelating agents and their action over the metal poisoning. • Know the mechanism of cisplatin in the fight against cancer. 2. Toxicity Toxicity is the degree to which a substance can damage an organism. Toxicity can refer to the effect on a whole organism, such as an animal, bacterium, or plant, as well as the effect on a substructure of the organism, such as a cell (cytotoxicity) or an organ such as the liver (hepatotoxicity). By extension, the word may be metaphorically used to describe toxic effects on larger and more complex groups, such as the family unit or society at large. Mechanism of the toxicity of metals is very complicated. Generally toxicity of metals may result from one of the following: i) Blocking the essential biological functional groups of biomolecules such as enzymes. Amino acid residues like serine is –OH functional group, cysteine is –SH group and histidine –N group often constitute the active sites of enzymes.