Uranium Toxicity and Chelation Therapy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chelation Therapy
Medical Policy Chelation Therapy Table of Contents • Policy: Commercial • Coding Information • Information Pertaining to All Policies • Policy: Medicare • Description • References • Authorization Information • Policy History Policy Number: 122 BCBSA Reference Number: 8.01.02 NCD/LCD: N/A Related Policies None Policy Commercial Members: Managed Care (HMO and POS), PPO, and Indemnity Medicare HMO BlueSM and Medicare PPO BlueSM Members Chelation therapy in the treatment of the following conditions is MEDICALLY NECESSARY: • Extreme conditions of metal toxicity • Treatment of chronic iron overload due to blood transfusions (transfusional hemosiderosis) or due to nontransfusion-dependent thalassemia (NTDT) • Wilson's disease (hepatolenticular degeneration), or • Lead poisoning. Chelation therapy in the treatment of the following conditions is MEDICALLY NECESSARY if other modalities have failed: • Control of ventricular arrhythmias or heart block associated with digitalis toxicity • Emergency treatment of hypercalcemia. NaEDTA as chelation therapy is considered NOT MEDICALLY NECESSARY. Off-label applications of chelation therapy are considered INVESTIGATIONAL, including, but not limited to: • Alzheimer’s disease • Arthritis (includes rheumatoid arthritis) • Atherosclerosis, (e.g., coronary artery disease, secondary prevention in patients with myocardial infarction, or peripheral vascular disease) • Autism • Diabetes • Multiple sclerosis. 1 Prior Authorization Information Inpatient • For services described in this policy, precertification/preauthorization IS REQUIRED for all products if the procedure is performed inpatient. Outpatient • For services described in this policy, see below for products where prior authorization might be required if the procedure is performed outpatient. Outpatient Commercial Managed Care (HMO and POS) Prior authorization is not required. Commercial PPO and Indemnity Prior authorization is not required. Medicare HMO BlueSM Prior authorization is not required. -

Sources, Effects and Risks of Ionizing Radiation
SOURCES, EFFECTS AND RISKS OF IONIZING RADIATION United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2016 Report to the General Assembly, with Scientific Annexes UNITED NATIONS New York, 2017 NOTE The report of the Committee without its annexes appears as Official Records of the General Assembly, Seventy-first Session, Supplement No. 46 and corrigendum (A/71/46 and Corr.1). The report reproduced here includes the corrections of the corrigendum. The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. The country names used in this document are, in most cases, those that were in use at the time the data were collected or the text prepared. In other cases, however, the names have been updated, where this was possible and appropriate, to reflect political changes. UNITED NATIONS PUBLICATION Sales No. E.17.IX.1 ISBN: 978-92-1-142316-7 eISBN: 978-92-1-060002-6 © United Nations, January 2017. All rights reserved, worldwide. This publication has not been formally edited. Information on uniform resource locators and links to Internet sites contained in the present publication are provided for the convenience of the reader and are correct at the time of issue. The United Nations takes no responsibility for the continued accuracy of that information or for the content of any external website. -

A Pilot Study in Detoxification of Heavy Metals
The Role of Heavy Metal Detoxification in Heart Disease and Cancers : A Pilot Study in Detoxification of Heavy Metals Daniel Dugi, M.D. Sir Arnold Takemoto Presented at the WESCON Biomedicine and Bioengineering Conference Anaheim Convention Center The Future of Medicine Afternoon Session September 24, 2002 Anaheim, California USA 1 ABSTRACT Heavy metal detoxification has been shown to decrease cancer mortality by 90% in a 18-year controlled clinical study by Blumer and Cranton. Frustachi et. al. has shown a very strong correlation between cardiomyopathy (heart disease) and heavy metals accumulation in the coronary arteries and heart muscle. The role of heavy metal detoxification in the prevention and/or treatment of cancers and heart disease is paramount for optimum healing or prevention. Heavy metal accumulation can cause suppression of the immune system, bind receptor sites, inhibit proper enzyme systems, and lead to undesirable free-radical and oxidative functions. A pilot study utilizing a unique oral detoxifying concentrate, DeTox Max, containing true disodium EDTA, microencapsulated in essential phospholipids microspheres was utilized as a provocation, detoxifying agent for a 16 patient pilot study. Significant quantities of heavy metals were excreted in a 48-hour collection versus each patient’s baseline 24 hour collection. The pilot study results confirmed substantial excretion of heavy metals. A surprising outcome of the study was the remarkable clinical healing and significant increase in brain acuity in patients that occurred within 2 weeks after only one vial was utilized, compared to previous pre - provocation. 2 Detox MAX Clinical Study Proposal ¾ To assess the heavy metal detoxifying ability of Detox MAX, an oral detoxification agent containing 22 grams of essential phospholipids (EPL’s); micro- encapsulating 1 gram of sodium endetate. -
Uranium-Free X Solution
www.nature.com/scientificreports OPEN Uranium‑free X solution: a new generation contrast agent for biological samples ultrastructure Aldo Moscardini1,6, Sebastiano Di Pietro 2,6, Giovanni Signore3*, Paola Parlanti4, Melissa Santi5, Mauro Gemmi5 & Valentina Cappello5* Biological samples are mainly composed of elements with a low atomic number which show a relatively low electron scattering power. For Transmission Electron Microscopy analysis, biological samples are generally embedded in resins, which allow thin sectioning of the specimen. Embedding resins are also composed by light atoms, thus the contrast diference between the biological sample and the surrounding resin is minimal. Due to that reason in the last decades, several staining solutions and approaches, performed with heavy metal salts, have been developed with the purpose of enhancing both the intrinsic sample contrast and the diferences between the sample and resin. The best staining was achieved with the uranyl acetate (UA) solution, which has been the election method for the study of morphology in biological samples. More recently several alternatives for UA have been proposed to get rid of its radiogenic issues, but to date none of these solutions has achieved efciencies comparable to UA. In this work, we propose a diferent staining solution (X Solution or X SOL), characterized by lanthanide polyoxometalates (LnPOMs) as heavy atoms source, which could be used alternatively to UA in negative staining (NS), in en bloc staining, and post sectioning staining (PSS) of biological samples. Furthermore, we show an extensive chemical characterization of the LnPOM species present in the solution and the detailed work for its fnal formulation, which brought remarkable results, and even better performances than UA. -

Chelation Therapy
Corporate Medical Policy Chelation Therapy File Name: chelation_therapy Origination: 12/1995 Last CAP Review: 2/2021 Next CAP Review: 2/2022 Last Review: 2/2021 Description of Procedure or Service Chelation therapy is an established treatment for the removal of metal toxins by converting them to a chemically inert form that can be excreted in the urine. Chelation therapy comprises intravenous or oral administration of chelating agents that remove metal ions such as lead, aluminum, mercury, arsenic, zinc, iron, copper, and calcium from the body. Specific chelating agents are used for particular heavy metal toxicities. For example, desferroxamine (not Food and Drug Administration [FDA] approved) is used for patients with iron toxicity, and calcium-ethylenediaminetetraacetic acid (EDTA) is used for patients with lead poisoning. Note that disodium-EDTA is not recommended for acute lead poisoning due to the increased risk of death from hypocalcemia. Another class of chelating agents, called metal protein attenuating compounds (MPACs), is under investigation for the treatment of Alzheimer’s disease, which is associated with the disequilibrium of cerebral metals. Unlike traditional systemic chelators that bind and remove metals from tissues systemically, MPACs have subtle effects on metal homeostasis and abnormal metal interactions. In animal models of Alzheimer’s disease, they promote the solubilization and clearance of β-amyloid protein by binding to its metal-ion complex and also inhibit redox reactions that generate neurotoxic free radicals. MPACs therefore interrupt two putative pathogenic processes of Alzheimer’s disease. However, no MPACs have received FDA approval for treating Alzheimer’s disease. Chelation therapy has also been investigated as a treatment for other indications including atherosclerosis and autism spectrum disorder. -

Circular of the Bureau of Standards No
t9?2 fcixt .Wii * S/ DEPARTMENT OF COMMERCE BUREAU OF STANDARDS S. W. STRATTON, Director CIRCULAR OF THE BUREAU OF STANDARDS No. Ill [Issued, March 11, 1921] RECOMMENDED SPECIFICATION FOR FLAT INTERIOR LITHOPONE PAINT, WHITE AND LIGHT TINTS PREPARED AND RECOMMENDED BY THE U. S. INTERDEPARTMENTAL COM- MITTEE ON PAINT SPECIFICATION STANDARDIZATION, JANUARY 21, 1921. P. H. WALKER, BUREAU OF STANDARDS, CHAIRMAN; J. W. GINDER, TREAS- URY DEPARTMENT, SECRETARY [This committee was appointed at the suggestion of the Secretary of Commerce, and consisted of repre- sentatives of the War, Navy, Agriculture, Interior, Post Office, Treasury, and Commerce Departments, the Panama Canal, and the Educational Bureau of the Paint Manufacturers* Association of the United States. The committee submitted a preliminary draft of the specification to a large number of representa- tives of the paint manufacturers, and gave careful consideration to the replies received.] CONTENTS Page 1. General 1 2 . Sampling 2 3 . Laboratory examination 3 4 . Analysis of pigment 5 5 . Reagents 7 1. GENERAL This specification covers ready-mixed lithopone paints, fre- quently known as flat, washable wall paint, in white and a variety of light tints. Paints under this specification are not intended for outside exposure; they shall dry to dead flat opaque coats that will adhere well to wood, metal, and plaster, stand washing with soap and water, and show no material change in color on exposure to light. The paint shall be purchased by volume (231 cubic inches to the gallon). 34615°—21 T 2 Circular of the Bureau of Standards (a) Pigment.—The pigment shall consist of: Maximum Minimum Per cent Per cent Lithopone 80 Zinc oxide 10 Tinting and extending pigments 10 Material soluble in water 0.8 Note.— he lithopone used must contain not less than 26 per cent of zinc sulphide and must not darken on exposure. -

Uranium Waste Focus Sheet
URANIUM WASTE Read below for information about safe packaging, labeling and disposing of uranium and thorium compounds. DESCRIPTION LABEL Uranium waste consists of solids and liquids Ensure container is contaminated with uranium and thorium compounds. properly labelled with Examples include uranyl acetate, uranyl nitrate, information about the uranyl formate and thorium nitrate. uranium or thorium compound, concentrations and a “Caution Radioactive Materials” sticker. DISPOSE Uranyl acetate and similar compounds are generally licensed, however any liquid or solid waste must be disposed of as radiological waste. Due to toxicity element of most Uranium and STORE Thorium compounds, liquid waste may be designated as Mixed Waste. Labs planning or concerned about generating uranium waste must consult with Solids Radiation Safety for disposal pricing, guidelines and For contaminated solids, designate an appropriate alternative options. sized container in a secure area (e.g., back of a fume hood in a locked lab). Label the container with a Uranium and thorium solid waste, powders or “Caution Radioactive Material” sticker. crystals will be collected by Radiation Safety for disposal. Liquids Store contaminated liquids in an appropriate strong To arrange a pick-up of uranium waste, complete a plastic container in secondary containment. Keep the Radioactive Waste Collection Request. waste container close to your work area to minimize chance of spilling. When not working, place waste in a posted and secure storage area. Liquid waste containers must always be properly labelled, and securely closed when not in use. Please contact EH&S Radiation Safety at 206.543.0463 or [email protected] for more information. Page 1 | September 2019 www.ehs.washington.edu | 206.543.7262 | [email protected] . -
Recognizing and Managing Lead and Mercury Poisonings
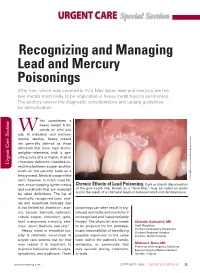
URGENT CARE Special Section Recognizing and Managing Lead and Mercury Poisonings After iron, which was covered in EM’s May issue, lead and mercury are the two metals most likely to be implicated in heavy metal toxicity syndromes. The authors review the diagnostic considerations and update guidelines for detoxification. hat constitutes a heavy metal? It de- W pends on who you ask. In industrial and environ- mental studies, heavy metals are generally defined as those elements that have high atomic weights—elements with a spe- cific gravity of 5 or higher. A strict chemistry definition classifies ev- Urgent Care Section Urgent Care erything between copper and bis- muth on the periodic table as a heavy metal. Medical usage of the term, however, is much more lib- Inc Researchers, Associates/Photo © 2009 Biphoto eral, encompassing lighter metals Chronic Effects of Lead Poisoning. Dark or bluish discoloration and metalloids that are excluded of the gum-tooth line, known as a “lead line,” may be noted on exam and is the result of a chemical reaction between lead and dental plaque. by other definitions. The list of medically recognized toxic met- als and metalloids includes (but is not limited to) aluminum, arse- poisonings can often result in sig- nic, barium, bismuth, cadmium, nificant morbidity and mortality if cobalt, copper, chromium, gold, unrecognized and inappropriately lead, manganese, mercury, sele- treated. The physician also needs Christian Balmadrid, MD nium, silver, thallium, and zinc.1 to be prepared for the postdiag- Staff Physician Heavy metal or metalloid tox- nostic responsibility of identifying Durham Emergency Physicians Durham Regional Hospital icity is relatively uncommon in possible exposures to the same Durham, North Carolina urgent care centers, but for that toxin within the patient’s family, very reason it is important to workplace, or community that Michael J. -

Managing Pet Bird Toxicoses J.A
birdtoxic.qxd 6/15/01 4:56 PM Page 23 CLINICIAN’S NOTEBOOK Managing Pet Bird Toxicoses J.A. RICHARDSON, L.A. MURPHY S.A. KHAN AND C. MEANS J.A. Richardson, DVM, Dipl ACFE L.A. Murphy, VMD S.A. Khan, DVM, PhD C. Means, DVM ASPCA Animal Poison Control Center 1717 South Philo Road Suite 36 Urbana, Illinois 61802 [email protected] Jill Richardson received her DVM degree from Tuskegee University in 1994. In 1996, following experience in small animal practices in Tennessee and West Virginia, Dr. Richardson joined the ASPCA Animal Poison Control BIRDS ARE CURIOUS BY NATURE, AND SOME HAZARDOUS OBJECTS Center as a Veterinary Poison may be attractive to them. Birds with free household access are more likely to Information Specialist. be exposed to toxicants. Sources of Toxicoses Affecting Pet Birds Reported to the APCC* 11% 27% 12% Pesticides Cleaning products Acknowledgements Plants Medicines The authors would like to thank 25% 25% Harold and Joyce Hamilton, Other, including heavy metals Cindy Dorner, Morgan Wilson, and Information collected between January 1996 - December 2000. Dr. Tracei Holder and the entire staff of the Animal Emergency Clinic of Champaign County. *The ASPCA Animal Poison Control Center, an operating division of the American Society for Photos: Tom Schaefges Photography the Prevention of Cruelty to Animals (ASPCA), is the only animal-oriented poison control Sidney, Illinois center in North America. It is a unique, emergency hotline providing 24-hour-a-day, [email protected] 7-day-a-week telephone assistance. The Center’s hotline veterinarians can quickly answer questions about toxic chemicals, dangerous plants, products or substances found in everyday surroundings that can prove poisonous or fatal to animals. -

Medical Toxicologists Determine Chelation Therapy Rarely Necessary
Medical Toxicologists Determine Chelation Therapy Rarely Necessary Experts from the American College of Medical Toxicology, the Centers for Disease Control, the Agency for Toxic Substances and Disease Registry, and others met at the CDC to review the current use and misuse of chelation therapy in the United States for the treatment of metal poisoning. It was concluded that incorrect diagnosis of metal poisoning is common, and inappropriate use of chelation therapy is widespread. Phoenix, Arizona (PRWEB) March 30, 2012 -- Medical toxicologists and scientific experts speaking at a recent conference at the Centers for Disease Control in Atlanta criticized the widespread misdiagnosis of poisoning from lead, arsenic, mercury and other metals, and called for strong efforts to decrease the inappropriate use of metal chelation therapy. Chelating agents are medications that may be given to patients to increase elimination of metals from the body. Traditionally chelating agents have been used to treat acute poisoning following a large exposure to a metal such as arsenic, mercury, or lead. In recent years, the administration of chelating agents by some health providers has increased. Although chelating agents such as calcium EDTA, DMSA, and DMPS are medications intended to be prescribed by licensed physicians, they are often sold to patients by health care practitioners or obtained without a prescription over the internet, possibly in violation of federal regulations. It has been estimated that nearly 200,000 people may be treated with chelating agents each year in the United States. These patients are frequently diagnosed with chronic metal poisoning based on a poorly documented environmental exposure, vague clinical findings, and inappropriate diagnostic testing. -

Role of the Intensive Care Unit in the Management of the Poisoned Patient Per Kulling and Hans Persson Swedish Poison Information Centre, Stockholm
Concepts in Toxicology Review Medical Toxicology I: 375·386 (1986) 0112·5966/0090·0375/$06.00/0 © ADIS Press Limited All rights reserved. Role of the Intensive Care Unit in the Management of the Poisoned Patient Per Kulling and Hans Persson Swedish Poison Information Centre, Stockholm Summary By applying a sensible toxicological approach to the general principles ofintensive care, an optimum setting for the treatment ofpoisoning is created. The intensive care unit (ICU) can perform the necessary close observation and monitoring, and thus facilitate rapid detection ofsymptoms, and the institution of early appropriate treatment. Diagnosis may be complex in poisoning and require continuous qualified interpretation of clinical and analytical data. Antidote therapy and treatment to enhance elimination ofthe poison must often be dealt with under careful supervision. The capacity ofthe ICU to counteract various toxic effects in a nonspecific way and to provide optimum symptomatic and supportive care is crucial. However, the ongoing toxic effects on the body must always be considered and allowed to guide symptomatic treatment. Thus, clinical toxicology appears to be a specialised branch of intensive care medicine. Many patients exposed to a poison may, after is of utmost importance for a proper interpretation initial measures like clinical assessment, gastric of clinical and analytical data and an immediate lavage and administration of activated charcoal, be start for necessary therapy. In some cases the ICU managed in general wards. However, to be able to may have a laboratory of its own, offering rapid adequately treat a severely poisoned patient the fa and frequent analysis. Another important aspect of cilities of an intensive care unit (ICU) are often the ICU is that there is generally a low threshold required and the capacity of such units to provide for accepting and utilising new and advanced ther optimum conditions for diagnosis and treatment apeutic methods. -

Exhibit 2D-3
Exhibit 2D–3. Hazardous Substances 1. Acetaldehyde 73. Captan 144. Ferrous sulfate 2. Acetic acid 74. Carbaryl 145. Formaldehyde 3. Acetic anhydride 75. Carbofuran 146. Formic acid 4. Acetone cyanohydrin 76. Carbon disulfide 147. Fumaric acid 5. Acetyl bromide 77. Carbon tetrachloride 148. Furfural 6. Acetyl chloride 78. Chlordane 149. Guthion 7. Acrolein 79. Chlorine 150. Heptachlor 8. Acrylonitrile 80. Chlorobenzene 151. Hexachlorocyclopentadiene 9. Adipic acid 81. Chloroform 152. Hydrochloric acid 10. Aldrin 82. Chloropyrifos 153. Hydrofluoric acid 11. Allyl alcohol 83. Chlorosulfonic acid 154. Hydrogen cyanide 12. Allyl chloride 84. Chromic acetate 155. Hydrogen sulfide 13. Aluminum sulfate 85. Chromic acid 156. Isoprene 14. Ammonia 86. Chromic sulfate 157. Isopropanolamine dodecylbenzenesulfonate 15. Ammonium acetate 87. Chromous chloride 158. Kelthane 16. Ammonium benzoate 88. Cobaltous bromide 159. Kepone 17. Ammonium bicarbonate 89. Cobaltous formate 160. Lead acetate 18. Ammonium bichromate 90. Cobaltous sulfamate 161. Lead arsenate 19. Ammonium bifluoride 91. Coumaphos 162. Lead chloride 20. Ammonium bisulfite 92. Cresol 163. Lead fluoborate 21. Ammonium carbamate 93. Crotonaldehyde 164. Lead fluorite 22. Ammonium carbonate 94. Cupric acetate 165. Lead iodide 23. Ammonium chloride 95. Cupric acetoarsenite 166. Lead nitrate 24. Ammonium chromate 96. Cupric chloride 167. Lead stearate 25. Ammonium citrate 97. Cupric nitrate 168. Lead sulfate 26. Ammonium fluoroborate 98. Cupric oxalate 169. Lead sulfide 27. Ammonium fluoride 99. Cupric sulfate 170. Lead thiocyanate 28. Ammonium hydroxide 100. Cupric sulfate ammoniated 171. Lindane 29. Ammonium oxalate 101. Cupric tartrate 172. Lithium chromate 30. Ammonium silicofluoride 102. Cyanogen chloride 173. Malathion 31. Ammonium sulfamate 103. Cyclohexane 174. Maleic acid 32. Ammonium sulfide 104.