NSAID–Gut Microbiota Interactions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Effect of Prostanoids on Human Platelet Function: an Overview
International Journal of Molecular Sciences Review Effect of Prostanoids on Human Platelet Function: An Overview Steffen Braune, Jan-Heiner Küpper and Friedrich Jung * Institute of Biotechnology, Molecular Cell Biology, Brandenburg University of Technology, 01968 Senftenberg, Germany; steff[email protected] (S.B.); [email protected] (J.-H.K.) * Correspondence: [email protected] Received: 23 October 2020; Accepted: 23 November 2020; Published: 27 November 2020 Abstract: Prostanoids are bioactive lipid mediators and take part in many physiological and pathophysiological processes in practically every organ, tissue and cell, including the vascular, renal, gastrointestinal and reproductive systems. In this review, we focus on their influence on platelets, which are key elements in thrombosis and hemostasis. The function of platelets is influenced by mediators in the blood and the vascular wall. Activated platelets aggregate and release bioactive substances, thereby activating further neighbored platelets, which finally can lead to the formation of thrombi. Prostanoids regulate the function of blood platelets by both activating or inhibiting and so are involved in hemostasis. Each prostanoid has a unique activity profile and, thus, a specific profile of action. This article reviews the effects of the following prostanoids: prostaglandin-D2 (PGD2), prostaglandin-E1, -E2 and E3 (PGE1, PGE2, PGE3), prostaglandin F2α (PGF2α), prostacyclin (PGI2) and thromboxane-A2 (TXA2) on platelet activation and aggregation via their respective receptors. Keywords: prostacyclin; thromboxane; prostaglandin; platelets 1. Introduction Hemostasis is a complex process that requires the interplay of multiple physiological pathways. Cellular and molecular mechanisms interact to stop bleedings of injured blood vessels or to seal denuded sub-endothelium with localized clot formation (Figure1). -

Studies on Betalain Phytochemistry by Means of Ion-Pair Countercurrent Chromatography
STUDIES ON BETALAIN PHYTOCHEMISTRY BY MEANS OF ION-PAIR COUNTERCURRENT CHROMATOGRAPHY Von der Fakultät für Lebenswissenschaften der Technischen Universität Carolo-Wilhelmina zu Braunschweig zur Erlangung des Grades einer Doktorin der Naturwissenschaften (Dr. rer. nat.) genehmigte D i s s e r t a t i o n von Thu Tran Thi Minh aus Vietnam 1. Referent: Prof. Dr. Peter Winterhalter 2. Referent: apl. Prof. Dr. Ulrich Engelhardt eingereicht am: 28.02.2018 mündliche Prüfung (Disputation) am: 28.05.2018 Druckjahr 2018 Vorveröffentlichungen der Dissertation Teilergebnisse aus dieser Arbeit wurden mit Genehmigung der Fakultät für Lebenswissenschaften, vertreten durch den Mentor der Arbeit, in folgenden Beiträgen vorab veröffentlicht: Tagungsbeiträge T. Tran, G. Jerz, T.E. Moussa-Ayoub, S.K.EI-Samahy, S. Rohn und P. Winterhalter: Metabolite screening and fractionation of betalains and flavonoids from Opuntia stricta var. dillenii by means of High Performance Countercurrent chromatography (HPCCC) and sequential off-line injection to ESI-MS/MS. (Poster) 44. Deutscher Lebensmittelchemikertag, Karlsruhe (2015). Thu Minh Thi Tran, Tamer E. Moussa-Ayoub, Salah K. El-Samahy, Sascha Rohn, Peter Winterhalter und Gerold Jerz: Metabolite profile of betalains and flavonoids from Opuntia stricta var. dilleni by HPCCC and offline ESI-MS/MS. (Poster) 9. Countercurrent Chromatography Conference, Chicago (2016). Thu Tran Thi Minh, Binh Nguyen, Peter Winterhalter und Gerold Jerz: Recovery of the betacyanin celosianin II and flavonoid glycosides from Atriplex hortensis var. rubra by HPCCC and off-line ESI-MS/MS monitoring. (Poster) 9. Countercurrent Chromatography Conference, Chicago (2016). ACKNOWLEDGEMENT This PhD would not be done without the supports of my mentor, my supervisor and my family. -

Nonsteroidal Antiinflammatory Drugs Inhibiting Prostanoid Efflux: As Easy As ABC?
Nonsteroidal antiinflammatory drugs inhibiting prostanoid efflux: As easy as ABC? Timothy D. Warner*† and Jane A. Mitchell‡ *The William Harvey Research Institute, Barts and the London School of Medicine and Dentistry, Charterhouse Square, London EC1M 6BQ, United Kingdom; and ‡National Heart and Lung Institute, Imperial College School of Medicine, Dovehouse Street, London SW3 6LY, United Kingdom onsteroidal antiinflammatory may explain its antinociceptive proper- resistance proteins (MRP) form a sub- drugs (NSAIDs) and prosta- ties (7). Others have found therapeutic family within the ABC transporters. noids continue to be fascinat- effects of NSAID metabolites that are MRP1 is a high-affinity leukotriene C4 N ing research targets. Humans inactive on COX; sulindac sulfone is a transporter, and mice that harbor dele- have been using NSAIDs in one form or clear example. The NSAID sulindac is tions of this gene have an altered re- another, from folk remedies through to an inactive drug metabolized to a phar- sponse to inflammatory stimuli but are the products of modern pharmaceutical macologically active sulfide derivative, otherwise healthy and fertile. MRP2 is research, for thousands of years. How- which potently inhibits COX. Sulindac is the major transporter responsible for ever, we still have not characterized all also metabolized to a sulfone derivative the secretion of bilirubin glucuronides of the systems through which these that is inactive against COX. However, into bile (11). MRP1 and -4 may also be drugs produce their beneficial and like sulindac sulfide, sulindac sulfone involved in the transport of dehydroepi- harmful effects (1, 2). We are certain, both promotes cellular apoptosis and androsterone 3-sulfate (the most abun- from seminal work carried out in the dant circulating steroid in humans), and 1960s and early 1970s, that NSAIDs MRP4 transports conjugated steroids have the common property of inhibiting Some NSAIDs and bile acids (12). -

Antiplatelet Effects of Prostacyclin Analogues: Which One to Choose in Case of Thrombosis Or Bleeding? Sylwester P
INTERVENTIONAL CARDIOLOGY Cardiology Journal 20XX, Vol. XX, No. X, XXX–XXX DOI: 10.5603/CJ.a2020.0164 Copyright © 20XX Via Medica REVIEW ARTICLE ISSN 1897–5593 eISSN 1898–018X Antiplatelet effects of prostacyclin analogues: Which one to choose in case of thrombosis or bleeding? Sylwester P. Rogula1*, Hubert M. Mutwil1*, Aleksandra Gąsecka1, Marcin Kurzyna2, Krzysztof J. Filipiak1 11st Chair and Department of Cardiology, Medical University of Warsaw, Poland 2Department of Pulmonary Circulation, Thromboembolic Diseases and Cardiology, Center of Postgraduate Education Medical, European Health Center Otwock, Poland Abstract Prostacyclin and analogues are successfully used in the treatment of pulmonary arterial hypertension (PAH) due to their vasodilatory effect on pulmonary arteries. Besides vasodilatory effect, prostacyclin analogues inhibit platelets, but their antiplatelet effect is not thoroughly established. The antiplatelet effect of prostacyclin analogues may be beneficial in case of increased risk of thromboembolic events, or undesirable in case of increased risk of bleeding. Since prostacyclin and analogues differ regarding their potency and form of administration, they might also inhibit platelets to a different extent. This review summarizes the recent evidence on the antiplatelet effects of prostacyclin and analogue in the treatment of PAH, this is important to consider when choosing the optimal treatment regimen in tailoring to an individual patients’ needs. (Cardiol J 20XX; XX, X: xx–xx) Key words: prostacyclin analogues, pulmonary arterial hypertension, platelets, antiplatelet effect, thrombosis, bleeding Introduction tiproliferative effects [4]. The main indication for PGI2 and analogues is advanced pulmonary arterial Since 1935 when prostaglandin was isolated hypertension (PAH) and peripheral vascular disor- for the first time [1], many scientists have focused ders [5]. -

Prostacyclin Therapies for the Treatment of Pulmonary Arterial Hypertension
Eur Respir J 2008; 31: 891–901 DOI: 10.1183/09031936.00097107 CopyrightßERS Journals Ltd 2008 SERIES ‘‘PULMONARY HYPERTENSION: BASIC CONCEPTS FOR PRACTICAL MANAGEMENT’’ Edited by M.M. Hoeper and A.T. Dinh-Xuan Number 2 in this Series Prostacyclin therapies for the treatment of pulmonary arterial hypertension M. Gomberg-Maitland* and H. Olschewski# ABSTRACT: Prostacyclin and its analogues (prostanoids) are potent vasodilators and possess AFFILIATIONS antithrombotic, antiproliferative and anti-inflammatory properties. Pulmonary hypertension (PH) *Dept of Cardiology, University of Chicago Hospitals, Chicago, IL, USA. is associated with vasoconstriction, thrombosis and proliferation, and the lack of endogenous #Dept of Pulmonology, Medical prostacyclin may considerably contribute to this condition. This supports a strong rationale for University Graz, Graz, Austria. prostanoid use as therapy for this disease. The first experiences of prostanoid therapy in PH patients were published in 1980. CORRESPONDENCE H. Olschewski Epoprostenol, a synthetic analogue of prostacyclin, and the chemically stable analogues Dept of Pulmonology iloprost, beraprost and treprostinil were tested in randomised controlled trials. The biological Medical University Graz actions are mainly mediated by activation of specific receptors of the target cells; however, new Auenbruggerplatz 20 data suggest effects on additional intracellular pathways. In the USA and some European Graz 8010 Austria countries, intravenous infusion of epoprostenol and treprostinil, as well as subcutaneous infusion Fax: 43 3163853578 of treprostinil and inhalation of iloprost, have been approved for therapy of pulmonary arterial E-mail: horst.olschewski@ hypertension. Iloprost infusion and beraprost tablets have been approved in few other countries. meduni-graz.at Ongoing clinical studies investigate oral treprostinil, inhaled treprostinil and the combination of Received: inhaled iloprost and sildenafil in pulmonary arterial hypertension. -

"Ellagic Acid, an Anticarcinogen in Fruits, Especially in Strawberries: a Review"
FEATURE Ellagic Acid, an Anticarcinogen in Fruits, Especially in Strawberries: A Review John L. Maasl and Gene J. Galletta2 Fruit Laboratory, U.S. Department of Agriculture, Agricultural Research Service, Beltsville, MD 20705 Gary D. Stoner3 Department of Pathology, Medical College of Ohio, Toledo, OH 43699 The various roles of ellagic acid as an an- digestibility of natural forms of ellagic acid, Mode of inhibition ticarcinogenic plant phenol, including its in- and the distribution and organ accumulation The inhibition of cancer by ellagic acid hibitory effects on chemically induced cancer, or excretion in animal systems is in progress appears to occur through the following its effect on the body, occurrence in plants at several institutions. Recent interest in el- mechanisms: and biosynthesis, allelopathic properties, ac- lagic acid in plant systems has been largely a. Inhibition of the metabolic activation tivity in regulation of plant hormones, for- for fruit-juice processing and wine industry of carcinogens. For example, ellagic acid in- mation of metal complexes, function as an applications. However, new studies also hibits the conversion of polycyclic aromatic antioxidant, insect growth and feeding in- suggest that ellagic acid participates in plant hydrocarbons [e.g., benzo (a) pyrene, 7,12- hibitor, and inheritance are reviewed and hormone regulatory systems, allelopathic and dimethylbenz (a) anthracene, and 3-methyl- discussed in relation to current and future autopathic effects, insect deterrent princi- cholanthrene], nitroso compounds (e.g., N- research. ples, and insect growth inhibition, all of which nitrosobenzylmethylamine and N -methyl- N- Ellagic acid (C14H6O8) is a naturally oc- indicate the urgent need for further research nitrosourea), and aflatoxin B1 into forms that curring phenolic constituent of many species to understand the roles of ellagic acid in the induce genetic damage (Dixit et al., 1985; from a diversity of flowering plant families. -

Betanin, the Main Pigment of Red Beet
Betanin, the main pigment of red beet - molecular origin of its exceptionally high free radical scavenging activity Anna Gliszczyńska-Świglo, Henryk Szymusiak, Paulina Malinowska To cite this version: Anna Gliszczyńska-Świglo, Henryk Szymusiak, Paulina Malinowska. Betanin, the main pigment of red beet - molecular origin of its exceptionally high free radical scavenging activity. Food Additives and Contaminants, 2006, 23 (11), pp.1079-1087. 10.1080/02652030600986032. hal-00577387 HAL Id: hal-00577387 https://hal.archives-ouvertes.fr/hal-00577387 Submitted on 17 Mar 2011 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Food Additives and Contaminants For Peer Review Only Betanin, the main pigment of red beet - molecular origin of its exceptionally high free radical scavenging activity Journal: Food Additives and Contaminants Manuscript ID: TFAC-2005-377.R1 Manuscript Type: Original Research Paper Date Submitted by the 20-Aug-2006 Author: Complete List of Authors: Gliszczyńska-Świgło, Anna; The Poznañ University of Economics, Faculty of Commodity Science -
Steviol Glycoside Determination by HPLC with Charged Aerosol and UV Detections Using the Acclaim Trinity P1 Column
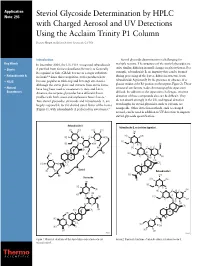
Application Note: 293 Steviol Glycoside Determination by HPLC with Charged Aerosol and UV Detections Using the Acclaim Trinity P1 Column Deanna Hurum and Jeffrey Rohrer; Sunnyvale, CA USA Introduction Steviol glycoside determination is challenging for Key Words In December 2008, the U.S. FDA recognized rebaudioside multiple reasons. The structures of the steviol glycosides are quite similar, differing in small changes in glycosylation. For • Stevia A purified from Stevia rebaudiana (Bertoni) as Generally Recognized as Safe (GRAS) for use as a sugar substitute example, rebaudioside B, an impurity that can be formed • Rebaudioside A in foods.1,2 Since this recognition, stevia products have during processing of the leaves, differs in structure from rebaudioside A primarily by the presence or absence of a • HILIC become popular as table-top and beverage sweeteners. Although the stevia plant and extracts from stevia leaves glucose residue at the R1 position on the terpene (Figure 2). These • Natural have long been used as sweeteners in Asia and Latin structural similarities make chromatographic separation Sweeteners America, the terpene glycosides have different flavor difficult. In addition to the separation challenges, sensitive profiles with both sweet and unpleasant bitter flavors.3 detection of these compounds also can be difficult. They Two steviol glycosides, stevioside and rebaudioside A, are do not absorb strongly in the UV, and typical detection largely responsible for the desired sweet flavor of the leaves wavelengths for steviol glycosides, such as 210 nm, are (Figure 1), with rebaudioside A preferred for sweeteners.4 nonspecific. Other detection methods, such as charged aerosol, can be used in addition to UV detection to improve steviol glycoside quantification. -
Application A1108 Rebaudioside M As a New Steviol Glycoside Intense
Supporting document 1 Risk and technical assessment report – Application A1108 Rebaudioside M as a New Steviol Glycoside Intense Sweetener Executive summary Rebaudioside M is similar in chemical structure and sweetness intensity to other currently permitted steviol glycosides. The production of rebaudioside M preparations, analytical methods, specifications and stability are similar to other steviol glycosides. Rebaudioside M occurs naturally in the leaves of the stevia plant at much lower concentrations than several other steviol glycosides so specific concentration and purification steps are required to produce preparations containing high concentrations of rebaudioside M. As for other steviol glycosides, rebaudioside M is hydrolysed completely to steviol by gut microflora. The existing acceptable daily intake (ADI) for steviol glycosides of 0– 4 mg/kg bodyweight, which is expressed on the basis of steviol, is therefore applicable to rebaudioside M. Rebaudioside M-containing preparations are intended for use in the same food categories and at the same use-levels already permitted for other steviol glycoside products. FSANZ has previously conducted a dietary exposure assessment using the current permissions for steviol glycosides and therefore no dietary exposure assessment was necessary for this Application. It is concluded that the use of rebaudioside M as a food additive in accordance with the current permissions for steviol glycosides raises no public health and safety concerns. 1 Table of Contents EXECUTIVE SUMMARY ........................................................................................................................ -

Apricot Kernel Oil (AKO)
RISK PROFILE Apricot kernel oil (AKO) C A S N o . 72869- 69- 3 Date of reporting 31.05.201 3 Content of document 1. Identification of substance ……………………………………………………… p. 1 2. Uses and origin ……………………………………………………… p. 7 3. Regulation ………………………………………………………………………… p. 10 4. Relevant toxicity studies ……………………………………………………… p. 10 5. Exposure estimates and critical NOAEL/NOEL …………………………………… p. 16 6. Other sources of exposure than cosmetic products …………………………. p. 19 7. Assessment ………………………………………………………………………… p. 23 8. Conclusion ………………………………………………………………………… p. 24 9. References ………………………………………………………………………… p. 25 10. Annexes ………………………………………………………………………… p. 29 1. Identification of substance Chemical name (IUPAC): Apricot kernel oil INCI PRUNUS ARMENIACA KERNEL OIL Synonyms Apricot oil CAS No. 72869-69-3 EINECS No. 272-046-1 / - Molecular formula Chemical structure Molecular weight Contents (if relevant) AKO is the fixed oil expressed from the kernels of the Apricot, Prunus armeniaca L., Rosaceae AKO meant for cosmetic purposes is usually produced by cold pressing of the kernel (seed) of wild (bitter) apricots (Asma BM et al 2007, Dwivedi DH et al 2008). A typical composition of such a seed is as follows (Azou Z et al 2009): (w/w) Risk profile Apricot kernel oil Page 1 of 36 Version date: 31MAY2013 Fat (triglycerides): 50.3 % Protein 27.8 % Sugar 11.3 % Fiber 3.1 % Moisture 5.5 % Ash 2.2 % Annex 1 shows a more detailed chemical composition of the seed according to the Phytochemical database of the American Department of Agriculture1. A combination of cold pressing and solvent extraction (petroleum ether, hexane, chloroform-methanol or methanol) yield an AKO that consists of the lipids 92 – 98 %. Besides, that oil consists of smaller amounts of phytosterols like beta-sitosterol. -

GRAS Notice 821 for Glucosylated Steviol Glycosides
GRAS Notice (GRN) No. 821 https://www.fda.gov/food/generally-recognized-safe-gras/gras-notice-inventory {Ri~(C~ij\;#~[Q) NOV I 9 2018 16 November 20 l 8 OFFICE OF FOOD ADDITIVE SAFETY Dr. Paulette Gaynor Office of Food Additive Safety (HFS-200) Center for Food Safety and Applied Nutrition (CFSAN) Food and Drug Administration 500 l Campus Drive College Park, MD 20740 USA Dear Dr. Gaynor: Re: GRAS Notice for High-Purity Glucosylated Steviol Glycosides In accordance with 21 CFR § 170 Subpart E consisting of§ 170.203 through 170.285, Haigen-BGG Natural Ingredients (HBNI) Limited [l 1038, 11/F, Tower A, Gateway Square No. 18, Xiaguangli, North Road East Third Ring, Chaoyang District, Beijing, China], as the notifier, is submitting one hard copy and one electronic copy (on CD), of all data and information supporting the company's conclusion that high-purity glucosylated steviol glycosides, as manufactured by HBNI, is GRAS under the specified conditions of use as a food ingredient on the basis of scientific procedures, and therefore are not subject to the premarket approval requirements of the Federal Food, Drug and Cosmetic Act. Information setting forth the basis for HBNI's GRAS conclusion, as well as a consensus opinion of an independent panel of experts, also are enclosed for review by the agency. l certify that the enclosed electronic files were scanned for viruses prior to submission and are thus certified as being virus-free using Symantec Endpoint Protection 12.1.5. Should you have any questions or concerns regarding this GRAS notice, please do not hesitate to contact me at any point during the review process so that we may provide a response in a timely manner. -

Modes of Action of Herbal Medicines and Plant Secondary Metabolites
Medicines 2015, 2, 251-286; doi:10.3390/medicines2030251 OPEN ACCESS medicines ISSN 2305-6320 www.mdpi.com/journal/medicines Review Modes of Action of Herbal Medicines and Plant Secondary Metabolites Michael Wink Institute of Pharmacy and Molecular Biotechnology, Heidelberg University, INF 364, Heidelberg D-69120, Germany; E-Mail: [email protected]; Tel.: +49-6221-544-881; Fax: +49-6221-544-884 Academic Editor: Shufeng Zhou Received: 13 August 2015 / Accepted: 31 August 2015 / Published: 8 September 2015 Abstract: Plants produce a wide diversity of secondary metabolites (SM) which serve them as defense compounds against herbivores, and other plants and microbes, but also as signal compounds. In general, SM exhibit a wide array of biological and pharmacological properties. Because of this, some plants or products isolated from them have been and are still used to treat infections, health disorders or diseases. This review provides evidence that many SM have a broad spectrum of bioactivities. They often interact with the main targets in cells, such as proteins, biomembranes or nucleic acids. Whereas some SM appear to have been optimized on a few molecular targets, such as alkaloids on receptors of neurotransmitters, others (such as phenolics and terpenoids) are less specific and attack a multitude of proteins by building hydrogen, hydrophobic and ionic bonds, thus modulating their 3D structures and in consequence their bioactivities. The main modes of action are described for the major groups of common plant secondary metabolites. The multitarget activities of many SM can explain the medical application of complex extracts from medicinal plants for more health disorders which involve several targets.