Effect of Prostanoids on Human Platelet Function: an Overview
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cox Inhibitors and Thromboregulation
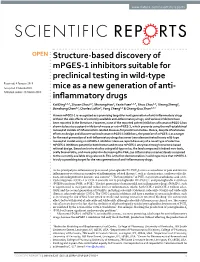
CLINICAL IMPLICATIONS OF BASIC RESEARCH Clinical Implications shown the importance of eicosanoids in preserving of Basic Research the dynamic balance among thrombosis, hemostasis, and the fluidity of blood. Recently, Cheng et al.1 presented compelling evi- dence that cell–cell interactions, principally between platelets and endothelial cells, that are mediated by ei- COX INHIBITORS cosanoids have a role in thrombosis. Using genetical- AND THROMBOREGULATION ly engineered mice that either overexpressed or lacked essential components of the eicosanoid pathway — ROM a historical perspective, there is perhaps no namely, receptors for prostacyclin (a platelet inhibitor Fmore interesting therapeutic saga than that of as- and vasodilator) or thromboxane A2 (a platelet agonist pirin, which began as a folk remedy, distilled from wil- and vasoconstrictor) — they found that the response low bark, and became a lifesaving preventive treatment of the intima of carotid vessels to mechanical injury is for ischemic cardiovascular disease. Aspirin primarily exuberant and leads to obstruction in mice lacking the inhibits the cyclooxygenase (COX)-dependent synthe- prostacyclin receptor. However, this response is muted sis of eicosanoids, which are the end products of me- in mice lacking the thromboxane A2 receptor or both tabolism of essential fatty acids and include prosta- receptors. In mice lacking the prostacyclin receptor cyclin and thromboxane A2. Numerous studies have (a defect that mimics the effects of COX-2–selective Endothelial cell Resting platelet Thromboxane A2 Soluble Stimulation CD39 Arachidonic acid Stimulated platelet COX inhibitor ATP and ADP Prostacyclin Nitric oxide AMP Carbon monoxide CD39 Resting platelet Figure 1. Effect on Platelet Reactivity of the Eicosanoids Thromboxane A2 and Prostacyclin, the Biologic Gases Nitric Oxide and Carbon Monoxide, and the Ectonucleotidase CD39. -

202514Orig1s000
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 202514Orig1s000 CLINICAL PHARMACOLOGY AND BIOPHARMACEUTICS REVIEW(S) OFFICE OF CLINICAL PHARMACOLOGY REVIEW NDA: 202-514 Submission Date(s): January 7, 2011 Proposed Brand Name TBD Generic Name Tafluprost Primary Reviewer Yongheng Zhang, Ph.D. Team Leader Philip M. Colangelo, Pharm.D., Ph.D. OCP Division DCP4 OND Division DTOP Applicant MERCK & CO., Inc. Relevant IND(s) 062690 Submission Type; Code 1S(NME) Formulation; Strength(s) Tafluprost 0.0015% Ophthalmic Solution Indication For the reduction of elevated intraocular pressure in open-angle glaucoma or ocular hypertension Dosage and Administration One drop of Tafluprost 0.0015% ophthalmic solution in the conjunctival sac of the affected eye(s) once daily in the evening TABLE OF CONTENTS 1. EXECUTIVE SUMMARY .................................................................................................................. 2 1.1. RECOMMENDATION ....................................................................................................................... 3 1.2. PHASE IV COMMITMENTS............................................................................................................. 3 1.3. SUMMARY OF IMPORTANT CLINICAL PHARMACOLOGY AND BIOPHARMACEUTICS FINDINGS.. 3 2. QUESTION BASED REVIEW ...........................................................................................................4 2.1. GENERAL ATTRIBUTES OF THE DRUG ......................................................................................... -

Prostaglandin E2 Deficiency Uncovers a Dominant Role for Thromboxane A2
Prostaglandin E2 deficiency uncovers a dominant role for thromboxane A2 in house dust mite-induced allergic pulmonary inflammation Tao Liua,b, Tanya M. Laidlawa,b,c, Chunli Fenga,b, Wei Xinga,b, Shiliang Shena,b, Ginger L. Milned, and Joshua A. Boycea,b,c,1 Departments of aMedicine and cPediatrics, Harvard Medical School, Boston, MA 02115; bDivision of Rheumatology, Immunology, and Allergy, Jeff and Penny Vinik Center for Allergic Disease Research, Brigham and Women’s Hospital, Boston, MA 02115; and dDepartment of Pharmacology, Vanderbilt University, Nashville, TN 37232 Edited* by K. Frank Austen, Brigham and Women’s Hospital, Boston, MA, and approved June 20, 2012 (received for review May 10, 2012) fl – Prostaglandin E2 (PGE2) is an abundant lipid in ammatory media- PGE2 production (16 19) and reduced expression of the EP2 re- tor with potent but incompletely understood anti-inflammatory ceptor (20, 21), as well as marked tissue eosinophilia and bron- actions in the lung. Deficient PGE2 generation in the lung predis- choconstrictive responses to the administration of nonselective poses to airway hyperresponsiveness and aspirin intolerance in COX inhibitors. These findings suggest potential therapeutic fi −/− asthmatic individuals. PGE2-de cient ptges mice develop exag- applications of PGE2 in asthma and AERD if the mechanisms gerated pulmonary eosinophilia and pulmonary arteriolar smooth- responsible for the homeostatic functions of PGE2 in asthma can fi muscle hyperplasia compared with PGE2-suf cient controls when be fully defined. challenged intranasally with a house dust mite extract. We now An extract (Df) of the house dust mite Dermatophagoides demonstrate that both pulmonary eosinophilia and vascular farinae contains clinically relevant protease allergens, as well as fi remodeling in the setting of PGE2 de ciency depend on thrombox- adjuvants (glycans, endotoxin) that elicit sensitization through ane A2 and signaling through the T prostanoid (TP) receptor. -

Coexpression of Microsomal Prostaglandin E Synthase With
Coexpression of Microsomal Prostaglandin E Synthase with Cyclooxygenase-2 in Human Rheumatoid Synovial Cells FUMIAKI KOJIMA, HIROAKI NARABA, YASUHARU SASAKI, RENZO OKAMOTO, TOMIHISA KOSHINO, and SHINICHI KAWAI ABSTRACT. Objective. Recently, microsomal prostaglandin (PG) E synthase (mPGES) was cloned as a terminal enzyme catalyzing PGH2 to PGE2. We investigated mPGES as well as cyclooxygenase (COX)-2, catalyzing arachidonic acid to PGH2, in synovial cells from patients with rheumatoid arthritis (RA). The effect of dexamethasone on mPGES expression was also studied. Methods. Synovial cells were treated with interleukin 1ß (IL-1ß) and dexamethasone under various conditions, and expression of mPGES mRNA and protein was analyzed by Northern blot and Western blot, respectively. Conversions of arachidonic acid or PGH2 to PGE2 were measured by ELISA. Subcellular localization of mPGES and COX-2 was determined by immunofluorescent microscopic analysis. Results. mPGES mRNA and protein expression were significantly upregulated by IL-1ß in synovial cells. COX-2 mRNA and protein were also upregulated by IL-1ß, but with a different time course from that of mPGES. Conversion of PGH2 to PGE2 was increased by IL-1ß and was correlated with mPGES expression. Increased conversion of arachidonic acid to PGE2 was maintained when mPGES and COX-2 were coexpressed. Subcellular localization of mPGES and COX-2 overlapped in the perinuclear region in IL-1ß stimulated synovial cells. Dexamethasone inhibited mRNA and protein expression for mPGES and increased conversion of arachidonic acid to PGE2, but inhibition of mPGES was weaker compared with that of COX-2 in IL-1ß stimulated cells. Conclusion. The results suggest that abundant PGE2 production at inflammation sites such as rheumatoid synovia is caused by the coordinated upregulation of mPGES and COX-2. -
Structure-Based Discovery of Mpges-1 Inhibitors Suitable For
www.nature.com/scientificreports OPEN Structure-based discovery of mPGES-1 inhibitors suitable for preclinical testing in wild-type Received: 4 January 2018 Accepted: 9 March 2018 mice as a new generation of anti- Published: xx xx xxxx infammatory drugs Kai Ding1,2,3, Ziyuan Zhou1,2, Shurong Hou2, Yaxia Yuan1,2,4, Shuo Zhou1,2, Xirong Zheng2, Jianzhong Chen1,2, Charles Loftin2, Fang Zheng1,2 & Chang-Guo Zhan1,2,4 Human mPGES-1 is recognized as a promising target for next generation of anti-infammatory drugs without the side efects of currently available anti-infammatory drugs, and various inhibitors have been reported in the literature. However, none of the reported potent inhibitors of human mPGES-1 has shown to be also a potent inhibitor of mouse or rat mPGES-1, which prevents using the well-established mouse/rat models of infammation-related diseases for preclinical studies. Hence, despite of extensive eforts to design and discover various human mPGES-1 inhibitors, the promise of mPGES-1 as a target for the next generation of anti-infammatory drugs has never been demonstrated in any wild-type mouse/rat model using an mPGES-1 inhibitor. Here we report discovery of a novel type of selective mPGES-1 inhibitors potent for both human and mouse mPGES-1 enzymes through structure-based rational design. Based on in vivo studies using wild-type mice, the lead compound is indeed non-toxic, orally bioavailable, and more potent in decreasing the PGE2 (an infammatory marker) levels compared to the currently available drug celecoxib. This is the frst demonstration in wild-type mice that mPGES-1 is truly a promising target for the next generation of anti-infammatory drugs. -

Endogenous Biosynthesis of Prostacyclin and Thromboxane and Platelet Function During Chronic Administration of Aspirin in Man
Endogenous biosynthesis of prostacyclin and thromboxane and platelet function during chronic administration of aspirin in man. G A FitzGerald, … , J A Lawson, A R Brash J Clin Invest. 1983;71(3):676-688. https://doi.org/10.1172/JCI110814. Research Article To assess the pharmacologic effects of aspirin on endogenous prostacyclin and thromboxane biosynthesis, 2,3-dinor-6- keto PGF1 alpha (PGI-M) and 2,3-dinor-thromboxane B2 (Tx-M) were measured in urine by mass spectrometry during continuing administration of aspirin. To define the relationship of aspirin intake to endogenous prostacyclin biosynthesis, sequential urines were initially collected in individuals prior to, during, and subsequent to administration of aspirin. Despite inter- and intra-individual variations, PGI-M excretion was significantly reduced by aspirin. However, full mass spectral identification confirmed continuing prostacyclin biosynthesis during aspirin therapy. Recovery of prostacyclin biosynthesis was incomplete 5 d after drug administration was discontinued. To relate aspirin intake to indices of thromboxane biosynthesis and platelet function, volunteers received 20 mg aspirin daily followed by 2,600 mg aspirin daily, each dose for 7 d in sequential weeks. Increasing aspirin dosage inhibited Tx-M excretion from 70 to 98% of pretreatment control values; platelet TxB2 formation from 4.9 to 0.5% and further inhibited platelet function. An extended study was performed to relate aspirin intake to both thromboxane and prostacyclin generation over a wide range of doses. Aspirin, in the range of 20 to 325 mg/d, resulted in a dose-dependent decline in both Tx-M and PGI-M excretion. At doses of 325-2,600 mg/d Tx-M excretion ranged from 5 to 3% of control values while PGI-M remained at 37-23% of control. -

Challenging the FDA Black Box Warning for High Aspirin Dose with Ticagrelor in Patients with Diabetes James J
PERSPECTIVES IN DIABETES Challenging the FDA Black Box Warning for High Aspirin Dose With Ticagrelor in Patients With Diabetes James J. DiNicolantonio and Victor L. Serebruany – Ticagrelor, a novel reversible antiplatelet agent, has a Food and ASA 300 325 mg (53.6%) in the U.S. compared with the Drug Administration (FDA) black box warning to avoid mainte- rest of the world (1.7%) was the only factor to explain nance doses of aspirin (ASA) .100 mg/daily. This restriction is (out of 37 variables explored) the regional interaction based on the hypothesis that ASA doses .100 mg somehow de- that ticagrelor was less effective and potentially more creased ticagrelor’s benefit in the Platelet Inhibition and Patient harmful than clopidogrel (2). However, this interaction Outcomes (PLATO) U.S. cohort. However, these data are highly was not significant, is highly postrandomized, comes postrandomized, come from a very small subgroup in PLATO from a very small subgroup of PLATO, and makes no (57% of patients in the U.S. site), and make no biological sense. biological sense (3). Moreover, the ticagrelor-ASA interaction was not significant by any multivariate Cox regression analyses. The Complete Re- sponse Review for ticagrelor indicates that for U.S. PLATO patients, an ASA dose .300 mg was not a significant interaction TICAGRELOR-ASA HYPOTHESIS for vascular outcomes. In the ticagrelor-ASA .300 mg cohort, all- The claimed ticagrelor-ASA interaction states that ticagrelor cause and vascular mortality were not significantly increased fi – P plus low-dose ASA is bene cial, whereas increasing doses (hazard ratio [HR] 1.27 [95% CI 0.84 1.93], = 0.262 and 1.39 of ASA in combination with ticagrelor produces adverse [0.87–2.2], P = 0.170), respectively. -

Estimation of Serum Prostaglandin D2 Levels and Its Expression in Tissue of Alopecia Areata
ISSN: 2536-9474 (Print) Original article / FYMJ ISSN: 2536-9482 (Online) Fayoum University Medical Journal Soliman et al., 2019,4(1), 77-85 Estimation of serum prostaglandin D2 levels and its expression in tissue of Alopecia areata Talal A. Abd-ElRaheem1, Samar M.R. El-Tahlawy2, Olfat G. Shaker3, Mohamed H.Mohamed4 and Yasmin F.Soliman5 1. M.D, professor of Dermatology, STDs and Andrology department, Faculty of Medicine Fayoum University. 2. M.D, professor of Dermatology department, Faculty of Medicine Cairo University 3. M.D, professor of Biochemistry department, Faculty of Medicine-Cairo University 4. MD, lecturer of Dermatology, STDs and Andrology department, Faculty of Medicine Fayoum University 5. M.B.B.CH, Dermatology, STDs and Andrology department, Faculty of Medicine, Cairo University Abstract Results: There was statistically highly Back ground: Alopecia areata is a recurrent, significant difference between the two groups non-scaring type of hair loss considered to be regarding the mean value of PGD2 in tissue in an autoimmune process. Though its AA patients. It was significantly lower than in etiopathogenesis is not fully understood, many control group (p < 0.001). The mean value of therapeutic options have been used by PGD2 in serum in AA patients was dermatologists, but none are curative or significantly lower than in control group (p< preventive. Prostaglandins analogues which 0.05). are used to treat glaucoma. Increase in eye lash Conclusion: Prostaglandin D2 exhibits a number, thickness and pigmentation have been strong role in etiology of alopecia areata and reported as side effect. significantly was elevated in serum and tissue Methods: This cross sectional case control of alopecia areata patients. -

GTH 2021 State of the Art—Cardiac Surgery: the Perioperative Management of Heparin-Induced Thrombocytopenia in Cardiac Surgery
Review Article 59 GTH 2021 State of the Art—Cardiac Surgery: The Perioperative Management of Heparin-Induced Thrombocytopenia in Cardiac Surgery Laura Ranta1 Emmanuelle Scala1 1 Department of Anesthesiology, Cardiothoracic and Vascular Address for correspondence Emmanuelle Scala, MD, Centre Anesthesia, Lausanne University Hospital (CHUV), Lausanne, Hospitalier Universitaire Vaudois, Rue du Bugnon 46, BH 05/300, 1011 Switzerland Lausanne, Suisse, Switzerland (e-mail: [email protected]). Hämostaseologie 2021;41:59–62. Abstract Heparin-induced thrombocytopenia (HIT) is a severe, immune-mediated, adverse drug Keywords reaction that paradoxically induces a prothrombotic state. Particularly in the setting of ► Heparin-induced cardiac surgery, where full anticoagulation is required during cardiopulmonary bypass, thrombocytopenia the management of HIT can be highly challenging, and requires a multidisciplinary ► cardiac surgery approach. In this short review, the different perioperative strategies to run cardiopul- ► state of the art monary bypass will be summarized. Introduction genicity of the antibodies and is diagnostic for HIT. The administration of heparin to a patient with circulating Heparin-induced thrombocytopenia (HIT) is a severe, im- pathogenic HITabs puts the patient at immediate risk of mune-mediated, adverse drug reaction that paradoxically severe thrombotic complications. induces a prothrombotic state.1,2 Particularly in the setting The time course of HIT can be divided into four distinct of cardiac surgery, where full anticoagulation is required phases.6 Acute HIT is characterized by thrombocytopenia during cardiopulmonary bypass (CPB), the management of and/or thrombosis, the presence of HITabs, and confirma- HIT can be highly challenging, and requires a multidisciplin- tion of their platelet activating capacity by a functional ary approach. -
Differential Activity and Clinical Utility of Latanoprost in Glaucoma and Ocular Hypertension
Clinical Ophthalmology Dovepress open access to scientific and medical research Open Access Full Text Article REVIEW Differential activity and clinical utility of latanoprost in glaucoma and ocular hypertension Fernanda Pacella Background: The purpose of this study was to demonstrate the hypotensive efficacy and tolerability Paolo Turchetti of latanoprost when used as monotherapy and as polytherapy associated with antiglaucomatous Valentina Santamaria medication proven to be ineffective in keeping intraocular pressure under control. David Impallara Methods: Three hundred and thirty-seven patients (672 eyes) affected by primary open-angle Gianpaolo Smaldone glaucoma and intraocular hypertension were recruited over a period of 10 years from the Chiara Brillante Glaucoma Centre, Department of Ophthalmological Sciences, University of Rome “Sapienza”, and treated, subject to informed consent, with latanoprost 0.005% alone or in combination Aloisa Librando with other ocular hypotensive drugs. The patients were followed during this period at regular Angela Damiano intervals, with determination of visual field, fundus oculi, visual acuity, and eventual onset of Jose Pecori-Giraldi local and systemic side effects. Elena Pacella Results: Latanoprost used as monotherapy and as polytherapy renders possible optimal and Department of Sense Organs, durable control of intraocular pressure in the form of one antiglaucomatous drug because it can University of Rome “Sapienza”, substitute for one or more drugs and obtain the same hypotensive effect. Roma, -

FDA-Approved Pre-Mixed Bag of Ibuprofen
Corporate Presentation Nasdaq CPIX Safe Harbor Statement This presentation contains forward-looking statements Important factors that could cause actual results to differ concerning our approved products and product materially from those indicated by such forward-looking development, our technology, our competitors, our statements include, among others, those set forth under intellectual property, our financial condition and our plans the headings "Risk factors" and "Management's discussion for research and development programs that involve risks, and analysis of financial condition and results of uncertainties and assumptions. These statements are operations" in our Form 10-K and Form 10-Q Reports on based on the current estimates and assumptions of the file with the SEC. The Company does not undertake any management of Cumberland Pharmaceuticals as of the obligation to release publicly any revisions to these date of this presentation and are subject to uncertainty and forward-looking statements to reflect events or changes in circumstances. Given these uncertainties, you circumstances after the date hereof or to reflect the should not place undue reliance upon these forward- occurrence of unanticipated events. All statements looking statements. Such forward-looking statements are contained in this presentation are made only as of the date subject to risks, uncertainties, assumptions and other of this presentation. For more information on our brands, factors that may cause the actual results of Cumberland including full prescribing and -

Antiluteogenic Effects of Serial Prostaglandin F2α Administration in Mares
ANTILUTEOGENIC EFFECTS OF SERIAL PROSTAGLANDIN F2α ADMINISTRATION IN MARES Thesis Presented in partial fulfillment of the requirements for the Master of Science in the Graduate School of The Ohio State University Elizabeth Ann Coffman Graduate ProGram in Comparative and Veterinary Medicine The Ohio State University 2013 Thesis committee: Carlos R.F. Pinto PhD, MV, DACT; Dissertation Advisor Marco A. Coutinho da Silva PhD, MV, DACT; Academic Advisor Christopher Premanandan PhD, DVM, DACVP Copyright by Elizabeth Ann Coffman 2013 Abstract For breedinG manaGement and estrus synchronization, prostaGlandin F2α (PGF) is one of the most commonly utilized hormones to pharmacologically manipulate the equine estrous cycle. There is a general supposition a sinGle dose of PGF does not consistently induce luteolysis in the equine corpus luteum (CL) until at least five to six days after ovulation. This leads to the erroneous assumption that the early CL (before day five after ovulation) is refractory to the luteolytic effects of PGF. An experiment was desiGned to test the hypotheses that serial administration of PGF in early diestrus would induce a return to estrus similar to mares treated with a sinGle injection in mid diestrus, and fertility of the induced estrus for the two treatment groups would not differ. The specific objectives of the study were to evaluate the effects of early diestrus treatment by: 1) assessing the luteal function as reflected by hormone profile for concentration of plasma progesterone; 2) determininG the duration of interovulatory and treatment to ovulation intervals; 3) comparing of the number of pregnant mares at 14 days post- ovulation. The study consisted of a balanced crossover desiGn in which reproductively normal Quarter horse mares (n=10) were exposed to two treatments ii on consecutive reproductive cycles.