Rotator Cuff Problems Written by Dr
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Shoulder Injuries: Dislocated Shoulder and Labral Tear
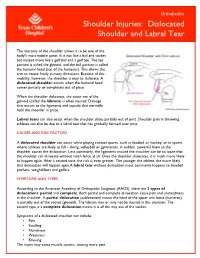
Orthopedics Shoulder Injuries: Dislocated Shoulder and Labral Tear The anatomy of the shoulder allows it to be one of the body's most mobile joints. It is not like a ball and socket but instead more like a golf ball and a golf tee. The tee portion is called the glenoid, and the ball portion is called the humeral head (top of the humerus). This allows the arm to rotate freely in many directions. Because of this mobility, however, the shoulder is easy to dislocate. A dislocated shoulder occurs when the humeral head comes partially or completely out of place. When the shoulder dislocates, the outer rim of the glenoid (called the labrum) is often injured. Damage also occurs to the ligaments and capsule that normally hold the shoulder in place. Labral tears can also occur when the shoulder slides partially out of joint. Shoulder pain in throwing athletes can also be due to a labral tear that has gradually formed over time. CAUSES AND RISK FACTORS A dislocated shoulder can occur while playing contact sports, such as football or hockey, or in sports where athletes are likely to fall – skiing, volleyball or gymnastics. A sudden, powerful blow to the shoulder causes the dislocation. Less commonly, the ligaments around the shoulder can be so loose that the shoulder can dislocate without much force at all. Once the shoulder dislocates, it is much more likely to happen again. After a second time, the risk is even greater. The younger the athlete, the more likely that dislocation will happen again.A labral tear without dislocation most commonly happens to baseball pitchers, weightlifters and golfers. -
Dislocated Shoulder -Orthoinfo - AAOS Page 1 of 2
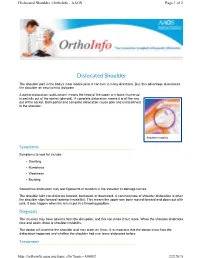
Dislocated Shoulder -OrthoInfo - AAOS Page 1 of 2 Dislocated Shoulder The shoulder joint is the body's most mobile joint. It can turn in many directions. But, this advantage also makes the shoulder an easy joint to dislocate. A partial dislocation (subluxation) means the head of the upper arm bone (humerus) is partially out of the socket (glenoid). A complete dislocation means it is all the way out of the socket. Both partial and complete dislocation cause pain and unsteadiness in the shoulder. Shoulder instability Symptoms Symptoms to look for include: • Swelling • Numbness • Weakness • Bruising Sometimes dislocation may tear ligaments or tendons in the shoulder or damage nerves. The shoulder joint can dislocate forward, backward, or downward. A common type of shoulder dislocation is when the shoulder slips forward (anterior instability). This means the upper arm bone moved forward and down out of its joint. It may happen when the arm is put in a throwing position. Diagnosis The muscles may have spasms from the disruption, and this can make it hurt more. When the shoulder dislocates time and again, there is shoulder instability. The doctor will examine the shoulder and may order an X-ray. It is important that the doctor know how the dislocation happened and whether the shoulder had ever been dislocated before. Treatment http://orthoinfo.aaos.org/topic.cfm?topic=A00035 2/2/2015 Dislocated Shoulder -OrthoInfo - AAOS Page 2 of 2 The doctor will place the ball of the upper arm bone (humerus) back into the joint socket. This process is called closed reduction. Severe pain stops almost immediately once the shoulder joint is back in place. -

Sports Injuries
Sports Injuries Lacrosse Lacrosse is America’s oldest game. It can be dated back to the Native Americans, and was used astraining for war. It is both played by boys and girls,however, some rules are drastically different between genders. Nonetheless, the combination of contact, a stick, a hard ball, and quick changes of direction, puts lacrosse players at risk for injury. Protective Equipment There is a wide range of equipment that lacrosse players wear. For girls, goggles and mouth pieces are mandatory. Lightweight gloves and headgear is optional. For boys, helmets with full face guards, shoulder pads, padded gloves, and mouth pieces are used. It is most important for this equipment to fit properly. If equipment does not fit properly it can actually cause injury. There is no helmet which has been proven through research that confused with a “dislocated shoulder,” which is when prevents concussions. the shoulder comes out of socket. Dislocated shoulders What are the most common types are not common in lacrosse. of lacrosse injuries? Concussions Contusions Concussions are quite common in lacrosse. For more information, please refer to our concussion handout. Because of the nature of the sport, bruises or contusions are very common in lacrosse. Contusions How can lacrosse injuries be prevented? are best initially treated with ice, compression, and elevation of the affected area. • Stay active year round Knee Injuries • Incorporate strength training and stretching into your normal routine Lacrosse players commonly injure their knees. Sprains of the medial and lateral collateral ligaments • Wear properly fitted equipment (MCL/LCL) occur. More serious injuries of the anterior and posterior cruciate ligaments (ACL/PCL) and to the • Hydrate adequately before, during, and menisci (cartilage of the knee) can also happen. -

About Soft Tissue Sarcoma Overview and Types
cancer.org | 1.800.227.2345 About Soft Tissue Sarcoma Overview and Types If you've been diagnosed with soft tissue sarcoma or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Is a Soft Tissue Sarcoma? Research and Statistics See the latest estimates for new cases of soft tissue sarcoma and deaths in the US and what research is currently being done. ● Key Statistics for Soft Tissue Sarcomas ● What's New in Soft Tissue Sarcoma Research? What Is a Soft Tissue Sarcoma? Cancer starts when cells start to grow out of control. Cells in nearly any part of the body can become cancer and can spread to other areas. To learn more about how cancers start and spread, see What Is Cancer?1 There are many types of soft tissue tumors, and not all of them are cancerous. Many benign tumors are found in soft tissues. The word benign means they're not cancer. These tumors can't spread to other parts of the body. Some soft tissue tumors behave 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 in ways between a cancer and a non-cancer. These are called intermediate soft tissue tumors. When the word sarcoma is part of the name of a disease, it means the tumor is malignant (cancer).A sarcoma is a type of cancer that starts in tissues like bone or muscle. Bone and soft tissue sarcomas are the main types of sarcoma. Soft tissue sarcomas can develop in soft tissues like fat, muscle, nerves, fibrous tissues, blood vessels, or deep skin tissues. -

Bilateral Simultaneous Rupture of the Quadriceps Tendons in Healthy Individuals Takuro Moriya1,2* and Abe Yoshihiro1
Moriya et al. Trauma Cases Rev 2016, 2:043 Volume 2 | Issue 3 ISSN: 2469-5777 Trauma Cases and Reviews Case Report: Open Access Bilateral Simultaneous Rupture of the Quadriceps Tendons in Healthy Individuals Takuro Moriya1,2* and Abe Yoshihiro1 1Department of Orthopaedic Surgery, Chiba Rosai Hospital, Japan 2Department of Orthopaedic Surgery, Chiba Kaihin Municipal Hospital, Japan *Corresponding author: Takuro Moriya, Department of Orthopaedic Surgery, Chiba Rosai Hospital, 2-16 Tatsumidai- higashi, Ichihara 290-0003, Japan, Tel: +81-436-74-1111, Fax: +81-436-74-1151, E-mail: [email protected] Abstract Quadriceps tendon rupture is an uncommon injury in healthy individuals. This paper presents two case reports of patients of bilateral quadriceps tendon rupture, who were misdiagnosed as muscle weakness of quadriceps with contusion of the knee joint. Subsequent physical examination showed a supra-patellar gap, moderate hemarthrosis of both knees, and failure of active knee extension. MRI showed bilateral rupture of the quadriceps tendons at the osteotendinous junction. Radiographs described the depression in the suprapatellar soft tissue, patella baja and an avulsion bony fragment on the patella. Surgery confirmed the MRI observation, so transosseous suturing and augmentation were undertaken. Both patients returned to a normal life with useful function. Adequate physical examination and correct understanding of both radiograph and MRI were required to prevent misdiagnosis. Keywords Bilateral quadriceps tendon ruptures, Healthy individuals Figure 1: Suprapatellar gap in Case 1. Introduction avulsion fragment on the patella (Figure 3). The patellar heights of his right and left knees were 0.89 and 0.68, respectively, using the Insall- Rupture of the quadriceps tendon is an uncommon injury, and Saivati method. -

Shoulder Dislocation
Shoulder Dislocation The human shoulder is an amazing machine. The unique us (ball) and the glenoid (socket) help prevent the anatomy of the shoulder enables the greatest range of joint from dislocating. The labrum, a firm tissue motion of any joint in the body. The shoulder allows over- that surrounds the glenoid, is another important head activities like screwing in a lightbulb and provides structure. When an injury happens, these liga- the strength to do a handstand or throw a 95-mile per ments and the labrum can be damaged, and a hour fastball. shoulder dislocation can result. Under normal circumstances, we rarely stop to think Causes about our shoulders. When an injury to the shoulder The normal shoulder joint can be thought of as a golf ball occurs, however, it often can be impossible to ignore. A balancing on a tee. If a large enough force in the right shoulder dislocation is one of those injuries. This article direction is applied to the arm, the ball will dislocate from covers the important aspects of shoulder dislocation: nor- the socket. This causes pain, and the shoulder will ap- mal anatomy, anatomy of a dislocation, diagnosis, treat- pear and feel abnormal. It will be difficult to move the ment, and future considerations after a dislocation. shoulder and arm. Sometimes the shoulder will go back into place on its own. When the shoulder will not go back Normal Anatomy of the Shoulder into place on its own, a reduction is required. This usually When most people think of the shoulder joint, the “ball involves a trip to the emergency room or other health and socket” comes to mind. -

A Miniature from the 15Th Century That Narrates Shoulder Reduction
DOI: 10.14744/ejmo.2017.46855 EJMO 2017;1(3):179-182 Letter to the Editor A Miniature From the 15th Century That Narrates Shoulder Reduction Engin Kesgin Private Antalya Medical Center, Antalya, Turkey Cite This Article: Kesgin E. A Miniature From 15th Century That Narrates Shoulder Reduction. EJMO. 2017; 1(3): 179-182 erefeddin Sabuncuoglu (1385–1470 A.D.) was a sur- gical textbook in Anatolian medicine.[2] Sgeon who lived in Amasya, which is in the northern part Sabuncuoglu was a master of Turkish, his mother lan- of middle Anatolia, in the 15th century during the period of guage. Although he knew Arabic, Greek, and Persian, he the Ottoman Empire. During his lifetime, he wrote detailed consciously wrote his book in Turkish because most phy- explanations of surgical methods and used miniatures to sicians and majority of the Anatolian public spoke Turkish demonstrate these methods. He made a significant con- at that time. The other reason was that medical books were tribution to the field of medical sciences, which included commonly written in other languages; thus, the public of the fields of obstetrics, gynecology, vascular surgery, nerve Anatolia was deprived of this knowledge in his era.[2] surgery, ophthalmology, oncology, dentistry, and plastic surgery.[1, 2] The 3rd volume of Sabuncuoglu’s manuscript’s, which deals with fractures and dislocations, includes a very de- His main book, Cerrahiyyet’ul Haniyye (Imperial Surgery), has tailed classification, definition, and treatment methods for three volumes: treatment by cauterization, surgical inter- shoulder dislocation with the inclusion of individual minia- ventions, and fractures and dislocations. -

Rotator Cuff Tears
OrthoInfo Basics Rotator Cuff Tears What is a rotator cuff? One of the Your rotator cuff helps you lift your arm, rotate it, and reach up over your head. most common middle-age It is made up of muscles and tendons in your shoulder. These struc- tures cover the head of your upper arm bone (humerus). This “cuff” complaints is holds the upper arm bone in the shoulder socket. shoulder pain. Rotator cuff tears come in all shapes and sizes. They typically occur A frequent in the tendon. source of that Partial tears. Many tears do not completely sever the soft tissue. Full thickness tears. A full or "complete" tear will split the soft pain is a torn tissue into two, sometimes detaching the tendon from the bone. rotator cuff. Rotator Cuff Bursa A torn rotator cuff will Tendon Clavicle (Collarbone) Humerus weaken your shoulder. (Upper Arm) This means that many Normal shoulder anatomy. daily activities, like combing your hair or Scapula getting dressed, may (Shoulder Blade) become painful and difficult to do. Rotator Cuff Tendon A complete tear of the rotator cuff tendon. 1 OrthoInfo Basics — Rotator Cuff Tears What causes rotator cuff tears? There are two main causes of rotator cuff repeating the same shoulder motions again and tears: injury and wear. again. Injury. If you fall down on your outstretched This explains why rotator cuff tears are most arm or lift something too heavy with a jerking common in people over 40 who participate in motion, you could tear your rotator cuff. This activities that have repetitive overhead type of tear can occur with other shoulder motions. -

Open Fracture As a Rare Complication of Olecranon Enthesophyte in a Patient with Gout Rafid Kakel, MD, and Joseph Tumilty, MD
A Case Report & Literature Review Open Fracture as a Rare Complication of Olecranon Enthesophyte in a Patient With Gout Rafid Kakel, MD, and Joseph Tumilty, MD has been reported in the English literature. The patient Abstract provided written informed consent for print and elec- Enthesophytes are analogous to osteophytes of osteo- tronic publication of this case report. arthritis. Enthesopathy is the pathologic change of the enthesis, the insertion site of tendons, ligaments, and CASE REPORT joint capsules on the bone. In gout, the crystals of mono- A 50-year-old man with chronic gout being treated with sodium urate monohydrate may provoke an inflamma- tory reaction that eventually may lead to ossification at allopurinol (and indomethacin on an as-needed basis) those sites (enthesophytes). Here we report the case of presented to the emergency department. He reported a man with chronic gout who sustained an open fracture of an olecranon enthesophyte when he fell on his left elbow. To our knowledge, no other case of open fracture of an enthesophyte has been reported in the English literature. nthesophytes are analogous to osteophytes of osteoarthritis. Enthesopathy is the pathologic change of the enthesis, the insertion site of ten- dons, ligaments, and joint capsules on the bone. EEnthesopathy occurs in a wide range of conditions, notably spondyloarthritides, crystal-induced diseases, and repeated minor trauma to the tendinous attach- ments to bones. Enthesopathy can be asymptomatic or symptomatic. In gout, crystals of monosodium urate are found in and around the joints—the cartilage, epiphyses, synovial membrane, tendons, ligaments, and enthesis. Figure 1. Small wound at patient’s left elbow. -

Heel Enthesopathy of Diffuse Idiopathic Skeletal Hyperostosis
Images in Rheumatology Heel Enthesopathy of Diffuse Idiopathic Skeletal Hyperostosis Resembling Enthesitis of Spondyloarthritis IGNAZIO OLIVIERI, MD, SALVATORE D’ANGELO, MD, Rheumatology Department of Lucania, San Carlo Hospital, Contrada Macchia Romana, 85100 Potenza, Italy; and Madonna delle Grazie Hospital; FRANCESCO BORRACCIA, Researcher, Radiology Department, San Carlo Hospital; ANGELA PADULA, MD, Senior Researcher, Rheumatology Department of Lucania, San Carlo Hospital, and Madonna delle Grazie Hospital, Matera, Italy. Address correspondence to Dr. Olivieri; E-mail: [email protected]. J Rheumatol 2010;37:192–3; doi.10.3899/jrheum.090514 Diffuse idiopathic skeletal hyperostosis (DISH) and anky- tendons, resembling the typical fusiform soft tissue swelling losing spondylitis (AS) are 2 clearly different disease enti- of Achilles enthesitis of spondyloarthritis5 (Figure 1). ties having in common the involvement of the axial skeleton However, palpation of the region did not reveal any inflam- and the peripheral entheses1,2. Both diseases produce bone matory findings of enthesitis but did reveal bone prolifera- proliferation in the spine and at the extraspinal entheseal tion due to large spurs, a condition confirmed by radio- sites in the later phases of their course. Although the aspects graphs (Figure 2). A sacroiliac joint computed tomography of the bone proliferations of the 2 diseases are dissimilar, (CT) scan showed the normal aspect of joint space and bony confusion of radiographic differential diagnosis between the margins together with the presence of capsular ossifications 2 diseases exists, partly as a consequence of a lack of aware- (Figure 3). ness of their respective characteristic features2,3. It has been pointed out that the differential diagnosis between DISH and REFERENCES longstanding advanced AS is not limited to the radiologic 1. -
Sports-Related Injuries Can Occur As the Result of a Single Traumatic Event, Such As an Impact Or Fall, Or from Repeated Overuse
COMMON SPORTS INJURIES Sports-related injuries can occur as the result of a single traumatic event, such as an impact or fall, or from repeated overuse and strain on muscles, tendons, and/or ligaments. Here are a few of the most common sports injuries. BICEPS FEMORIS (LONG HEAD) PULLING YOUR LEG Strains and sprains make up the bulk of sports injuries. Strains happen when muscles or SEMITENDINOSUS tendons are overstretched or torn - if someone has a pulled muscle, that means they have a muscle strain. The most commonly strained muscles are the hamstrings. SEMIMEMBRANOSUS Strains are best prevented by proper stretching, strengthening, and proper warm-ups before athletic activity. 2 SPRAIN, SPRAIN GO AWAY ANTERIOR TALOFIBULAR LIGAMENT Sprains happen when ligaments (PARTIALLY TORN) are overstretched or torn. Sprained ankles often happen when a fall or awkward landing from a jump forces the ankle joint to move in an unusual way, stressing or possibly tearing the ligaments surrounding it. Walking, running, or jumping on an uneven surface can also cause a sprained ankle. Stretching, strengthening, and balance exercises (as well as supportive footwear) can help reduce the risk of ankle sprains. 3 YOU’RE FEMUR TEARING ME APART! Many other muscles, tendons, and ligaments frequently tear. ACL (anterior cruciate ligament tears tend to happen in sports that put stress on the knees through jumping, sudden stops, and rapid changes in direction. Keeping the strength of hamstring PATELLA and quadriceps muscles balanced and (KNEECAP) TIBIA practicing safe landing and pivoting techniques can help prevent ACL tears. Factoid! Around 55% of sports-related injuries involve the knees. -

Acute Management of Soft Tissue Injuries
www.acpsm.org Acute Management of Soft Tissue Injuries Protection, Rest, Ice, Compression, and Elevation Guidelines www.acpsm.org Management of acute soft tissue injury using Protection Rest Ice Compression and Elevation: Recommendations from the Association of Chartered Physiotherapists in Sports and Exercise Medicine (ACPSM) Chris M Bleakley1, Philip D Glasgow2, Nicola Phillips2, Laura Hanna2, Michael J Callaghan2, Gareth W Davison3, Ty J Hopkins3, Eamonn Delahunt3 1Lead author and guarantor 2ACPSM consensus panel 3External authors and contributors Acknowledgements to other ACPSM contributors: Lynn Booth, Nicola Combarro, Sian Knott, Chris McNicholl and Colin Paterson for their assistance with literature searching, data extraction, and interpretation of outcomes. This work was funded by the Association of Chartered Physiotherapists in Sports and Exercise Medicine (ACPSM). The guidelines are endorsed by the Chartered Society of Physiotherapy’s Supporting Knowledge in Physiotherapy Practice Programme (SKIPP), after peer review from their Good Practice Panel in October 2010. CONTENTS Chapter 1: Project methods Chapter 2: What is the magnitude and depth of cooling associated with ice? Chapter 3: Can PRICE decrease the infl ammatory response after acute soft tissue injury? Chapter 4: What effect does mechanical loading have on infl ammation and soft tissue healing after acute injury? Chapter 5: Do the physiological effects of local tissue cooling affect function, sporting performance and injury risk? Chapter 6: Which components of PRICE are effective in the clinical management of acute soft tissue injury? Chapter 7: Executive summary Chapter 8: Appendices Chapter 1 Project methods Background The need for guidelines Soft tissue injury is a common problem in sport, recreational and physical activities.