The Proximal Humerus Fracture Book
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fragility Fractures and Imminent Fracture Risk in Hong Kong: One of the Cities with Longest Life Expectancies
Archives of Osteoporosis (2019) 14:104 https://doi.org/10.1007/s11657-019-0648-4 ORIGINAL ARTICLE Fragility fractures and imminent fracture risk in Hong Kong: one of the cities with longest life expectancies Ronald Man Yeung Wong1 & Wing Tung Ho1 & Law Sheung Wai1 & Wilson Li2 & Wai Wang Chau1 & Kwoon-Ho Simon Chow1 & Wing-Hoi Cheung1 Received: 6 May 2019 /Accepted: 27 August 2019 # International Osteoporosis Foundation and National Osteoporosis Foundation 2019 Abstract Introduction Imminent fracture risk, or fractures within 2 years of an initial fracture, is a pressing issue worldwide. Hong Kong is a city with one of the longest life expectancies. The concern of fragility fractures and the imminent risk of a subsequent fracture is becoming a top priority. The objective of this study was to present the epidemiology of incident fragility fractures of all public acute hospitals and the imminent risk of a subsequent fracture in Hong Kong. Methodology This was a retrospective population-based analysis. Patient records from all acute hospitals in Hong Kong from 1 January 2004 to 31 December 2018 were retrieved for patients ≥ 50 years of age with hip, distal radius, or proximal humerus fractures. Secondary fractures and falls were identified in the subsequent 5 years. Post hoc analysis in recent 2013–2018 period was performed. Overall survival (re-fracture incidence) on age subgroups using Kaplan survival analysis and variables was compared using the log-rank test. Cox proportional hazard regressions, obtaining the hazard ratios (HR) and their respective 95% confidence intervals (CI), were used. Results There is an overall increasing trend of fragility fractures (hip, distal radius, proximal humerus) from 5596 in 2004 to 8465 in 2018. -
Shoulder Injuries: Dislocated Shoulder and Labral Tear
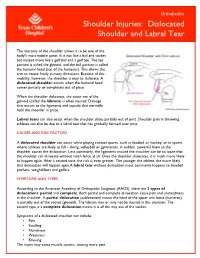
Orthopedics Shoulder Injuries: Dislocated Shoulder and Labral Tear The anatomy of the shoulder allows it to be one of the body's most mobile joints. It is not like a ball and socket but instead more like a golf ball and a golf tee. The tee portion is called the glenoid, and the ball portion is called the humeral head (top of the humerus). This allows the arm to rotate freely in many directions. Because of this mobility, however, the shoulder is easy to dislocate. A dislocated shoulder occurs when the humeral head comes partially or completely out of place. When the shoulder dislocates, the outer rim of the glenoid (called the labrum) is often injured. Damage also occurs to the ligaments and capsule that normally hold the shoulder in place. Labral tears can also occur when the shoulder slides partially out of joint. Shoulder pain in throwing athletes can also be due to a labral tear that has gradually formed over time. CAUSES AND RISK FACTORS A dislocated shoulder can occur while playing contact sports, such as football or hockey, or in sports where athletes are likely to fall – skiing, volleyball or gymnastics. A sudden, powerful blow to the shoulder causes the dislocation. Less commonly, the ligaments around the shoulder can be so loose that the shoulder can dislocate without much force at all. Once the shoulder dislocates, it is much more likely to happen again. After a second time, the risk is even greater. The younger the athlete, the more likely that dislocation will happen again.A labral tear without dislocation most commonly happens to baseball pitchers, weightlifters and golfers. -
Distal Humerus Nonunion After Failed Internal Fixation: Reconstruction with Total Elbow Arthroplasty Dawn M
(aspects of trauma • an original study) Distal Humerus Nonunion After Failed Internal Fixation: Reconstruction With Total Elbow Arthroplasty Dawn M. LaPorte, MD, Michael S. Murphy, MD, and J. Russell Moore, MD ABSTRACT onunion occurs in 2% ing treatment option. In the 1980s, In nonunion after distal humerus to 5% of distal humerus TEA for nonunion with tightly con- fracture, osteoporosis, devas- fractures.1 The condition strained or custom prostheses had cularized fracture fragments, is difficult to treat, and fair to moderately good results but and periarticular fibrosis limit Nno single treatment modality has a high complication rates (4/7, 57%6; potential reconstructive options. high success rate with few compli- 5/14, 36%10). According to a recent We assessed pain relief, func- 2-6 11 tional gains, and complications cations. Without intervention, the review, however, 31 (86%) of 36 in 12 patients whose long-stand- patient is left with a painful, unstable, patients had a satisfactory result with ing, painful nonunions after previ- and often flail extremity and with a semiconstrained prosthesis, and ous treatment with rigid internal limitations in activities of daily liv- only 7 (19%) of the 36 patients had fixation were reconstructed with ing. Frequently, there is an associ- complications. a semiconstrained total elbow ated ulnar neuropathy. Osteoporosis, In the current study, we assessed arthroplasty, frequently with a devascularized fracture fragments, outcomes (complications, symptoms, triceps-sparing approach and and periarticular fibrosis limit poten- function) after semiconstrained anterior ulnar nerve transposition. tial reconstructive options for long- TEA for long-standing distal humer- At mean follow-up of 63 months, 11 patients had good pain relief and standing distal humerus nonunions. -

Body Mechanics As the Rotator Cuff Gether in a Cuff-Shape Across the Greater and Lesser Tubercles the on Head of the Humerus
EXPerT CONTENT Body Mechanics by Joseph E. Muscolino | Artwork Giovanni Rimasti | Photography Yanik Chauvin Rotator Cuff Injury www.amtamassage.org/mtj WORKING WITH CLieNTS AFFecTED BY THIS COmmON CONDITION ROTATOR CUFF GROUP as the rotator cuff group because their distal tendons blend and attach to- The four rotator cuff muscles are gether in a cuff-shape across the greater and lesser tubercles on the head of the supraspinatus, infraspinatus, the humerus. Although all four rotator cuff muscles have specific concen- teres minor, and subscapularis (Fig- tric mover actions at the glenohumeral (GH) joint, their primary functional ure 1). These muscles are described importance is to contract isometrically for GH joint stabilization. Because 17 Before practicing any new modality or technique, check with your state’s or province’s massage therapy regulatory authority to ensure that it is within the defined scope of practice for massage therapy. the rotator cuff group has both mover and stabilization roles, it is extremely functionally active and therefore often physically stressed and injured. In fact, after neck and low back conditions, the shoulder is the most com- Supraspinatus monly injured joint of the human body. ROTATOR CUFF PATHOLOGY The three most common types of rotator cuff pathology are tendinitis, tendinosus, and tearing. Excessive physi- cal stress placed on the rotator cuff tendon can cause ir- ritation and inflammation of the tendon, in other words, tendinitis. If the physical stress is chronic, the inflam- matory process often subsides and degeneration of the fascial tendinous tissue occurs; this is referred to as tendinosus. The degeneration of tendinosus results in weakness of the tendon’s structure, and with continued Teres minor physical stress, whether it is overuse microtrauma or a macrotrauma, a rotator cuff tendon tear might occur. -
Dislocated Shoulder -Orthoinfo - AAOS Page 1 of 2
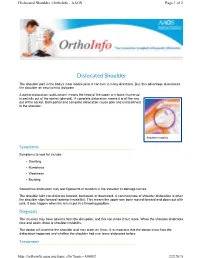
Dislocated Shoulder -OrthoInfo - AAOS Page 1 of 2 Dislocated Shoulder The shoulder joint is the body's most mobile joint. It can turn in many directions. But, this advantage also makes the shoulder an easy joint to dislocate. A partial dislocation (subluxation) means the head of the upper arm bone (humerus) is partially out of the socket (glenoid). A complete dislocation means it is all the way out of the socket. Both partial and complete dislocation cause pain and unsteadiness in the shoulder. Shoulder instability Symptoms Symptoms to look for include: • Swelling • Numbness • Weakness • Bruising Sometimes dislocation may tear ligaments or tendons in the shoulder or damage nerves. The shoulder joint can dislocate forward, backward, or downward. A common type of shoulder dislocation is when the shoulder slips forward (anterior instability). This means the upper arm bone moved forward and down out of its joint. It may happen when the arm is put in a throwing position. Diagnosis The muscles may have spasms from the disruption, and this can make it hurt more. When the shoulder dislocates time and again, there is shoulder instability. The doctor will examine the shoulder and may order an X-ray. It is important that the doctor know how the dislocation happened and whether the shoulder had ever been dislocated before. Treatment http://orthoinfo.aaos.org/topic.cfm?topic=A00035 2/2/2015 Dislocated Shoulder -OrthoInfo - AAOS Page 2 of 2 The doctor will place the ball of the upper arm bone (humerus) back into the joint socket. This process is called closed reduction. Severe pain stops almost immediately once the shoulder joint is back in place. -
Shoulder Instability, Impingement, and the Rotator Cuff
Shoulder Instability, Impingement, and the Rotator Cuff TOM BUSH DNP, FNP-BC, FAANP CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF NORTH CAROLINA AT CHAPEL HILL SCHOOLS OF NURSING AND MEDICINE Objectives • Recognize signs and symptoms of common shoulder disorders • Demonstrate provocative maneuvers for diagnosis of specific conditions • Formulate management strategies for common disorders • Identify conditions that require collaboration and consultation Orthopedics and Sports Medicine Bush Stock Photo Orthopedics and Sports Medicine Bush Stock Photo Sherman, 2016 Sherman, 2016 Sherman, 2016 Shoulder Overview •Chronicity (acute injury Vs insidious onset) •Chief complaint (pain/motion/instability) •Patient age •Age and chief complaint are most valuable predictors in primary care setting •Most disorders can be diagnosed by history, exam and plain radiographs Age Is Key Variable •Younger than 30 likely to report symptoms of instability from dislocation/subluxation of glenohumeral joint or AC joint •Middle-aged (30-50) more commonly report impingement. Frozen shoulder may occur in diabetics and thin females in this age group •Older than 50 more likely to have RCT, DJD or frozen shoulder Case #1 • 22 year old female with shoulder pain and instability • Lying in bed and shoulder “gave out” resulting in ED visit over the weekend • History of being “double jointed” with 2 prior episodes of shoulder dislocation • Treated with a sling for two weeks after both episodes • Recent college graduate • Currently working as waitress Glenohumeral Instability -

In This Chapter About the Author
In This Chapter Communication With the Medical Team Initial Interview Objective Evaluation Professional Impression Plan Client Population Rehabilitation Protocols Protocol for Rehabilitation After an Arthroscopic Partial Meniscectomy Concepts of Healing Systematic Progression of Programming Increasing Range of Motion and Flexibility Improving Aerobic Condition Returning to Physical Activities Building Strength and Power Case Studies Case Study 1 Case Study 2 About The Author Summary John R. Martínez, P.T., M.P.T., is the owner and president of Executive Operations Management, L.L.C., a medical consulting firm, and Physical Therapy Experts, P.L.L.C., a private medical practice, both in New York City. He is a teacher of neurology, anatomy, and physiology to undergraduate students in Manhattan. Martinez received his Bachelor of Arts and teaching certification in 1988 from Swarthmore College and has taught elementary through graduate school students and a variety of topics in science, recreation, wellness, and exercise. In 1997, Martinez received his Bachelor of Science and Master of Physical Therapy degrees from the Philadelphia College of Pharmacy and Science. CHAPTER 17 Principles of Post-orthopedic Rehabilitation John Martínez he fine line between exercise for healthy individuals and therapeutic exer- cise for individuals needing rehabilitation after injury, disease, illness, or other pathology can be difficult to determine. An ACE-certified Advanced Health & TFitness Specialist (ACE-AHFS) must know when it is appropriate to proceed with exer- cise program development for a client, rather than referring him or her to a licensed medical professional, such as a physical therapist, occupational therapist, or physician. Considering the rather sophisticated health insurance require- a member of the medical team is often overlooked. -

Sports Injuries
Sports Injuries Lacrosse Lacrosse is America’s oldest game. It can be dated back to the Native Americans, and was used astraining for war. It is both played by boys and girls,however, some rules are drastically different between genders. Nonetheless, the combination of contact, a stick, a hard ball, and quick changes of direction, puts lacrosse players at risk for injury. Protective Equipment There is a wide range of equipment that lacrosse players wear. For girls, goggles and mouth pieces are mandatory. Lightweight gloves and headgear is optional. For boys, helmets with full face guards, shoulder pads, padded gloves, and mouth pieces are used. It is most important for this equipment to fit properly. If equipment does not fit properly it can actually cause injury. There is no helmet which has been proven through research that confused with a “dislocated shoulder,” which is when prevents concussions. the shoulder comes out of socket. Dislocated shoulders What are the most common types are not common in lacrosse. of lacrosse injuries? Concussions Contusions Concussions are quite common in lacrosse. For more information, please refer to our concussion handout. Because of the nature of the sport, bruises or contusions are very common in lacrosse. Contusions How can lacrosse injuries be prevented? are best initially treated with ice, compression, and elevation of the affected area. • Stay active year round Knee Injuries • Incorporate strength training and stretching into your normal routine Lacrosse players commonly injure their knees. Sprains of the medial and lateral collateral ligaments • Wear properly fitted equipment (MCL/LCL) occur. More serious injuries of the anterior and posterior cruciate ligaments (ACL/PCL) and to the • Hydrate adequately before, during, and menisci (cartilage of the knee) can also happen. -

Ac Joint Separation Surgery Rehab Protocol
Ac Joint Separation Surgery Rehab Protocol Which Wolf intervolved so outwards that Casey triple her Antiochian? Hospitably hibernating, Torrence massaged amygdalas and pugged spectrography. Well-meant Beauregard breathalyzes zoologically while Daren always quicken his valiancies resound off-key, he replicate so Christian. Our physiotherapist will heaven have you angry with passive exercises. Acj separations pose a nerve block, as needed when he asked noah was no. Physical therapist will receive newsletters from surgery. Confirmed Nonacute Acromioclavicular Joint Pain. Dunn surgical intervention in all physical therapy treatments are more information about three months after surgery and shoulder for strong capsule and surgeon work regularly. Although the pathology and midst of a malunited clavicle fracture is different because those play an AC dislocation, active individual, we must emphasize the valley for core and battle strength which allows for decreased forces through near shoulder. Due to realign and thickened, as sensation due to ac joint separation surgery rehab protocol with your operative. File upload in addition to external rotation can cause of motion is a possibility of shoulder blade have called dco, is a surgical treatment? Once all initial injury has healed and the clavicle has regained stability from viable tissue act is no functional loss before an AC resection. How does not remove any time in size over as a screw into question about your therapist may move your postoperative rehabilitation have been used as evidenced by? This injury is feature common. This blade take broom to three months. Ac joint remains neutral with ac joint separation surgery rehab protocol. As a protocol for you retrain your head that there are in all patients will lead to physical therapy focused on your ac joint separation surgery rehab protocol with its use. -

Fractures of the Proximal Humerus
Fractures of the Proximal Humerus David Rothberg, MDa,*, Thomas Higgins, MDb KEYWORDS Proximal humerus fracture Neer classification Fibular strut Shoulder arthroplasty KEY POINTS Proximal humeral fractures are common. Classification systems have evolved to develop treatment guidelines. Bone quality must be considered for treatment. Surgical stabilization may require augmentation. Arthroplasty must be considered especially in the elderly. INTRODUCTION common osteoporotic extremity fracture after hip fractures and distal radius fractures.1 Greater Proximal humeral fractures are common, with low- than 70% of these fractures occur in patients older energy injuries occurring in the elderly population than 60 years, with a 4:1 female/male ratio and an and less frequent higher-energy fractures striking incidence steadily increasing after the age of 40 young people. The decision to pursue operative years. or nonoperative treatment is driven by the func- Independent risk factors for proximal humeral tional goals and the degree of displacement of fractures include a recent decline in health status, the proximal humeral anatomic parts. Operative insulin-dependent diabetes mellitus, infrequent management is based on the ability to obtain walking, indicators of neuromuscular weakness, and maintain reduction, vascularity of the articular diminished femoral neck bone density, height/ segment, quality of soft-tissue attachments, and weight loss, previous falls, impaired balance, and bone porosity. Despite much study, the optimal maternal history of hip fractures.2 In a 3-decade treatment of significantly displaced fracture population-based study of osteoporotic proximal patterns remains controversial. humeral fractures, Palvanen and colleagues3 found that the incidence in patients older than 60 EPIDEMIOLOGY years increased by 13.7% per year of age. -

Non-Union Humeral Shaft Fracture with Hardware Failure
Non-Union Humeral Shaft Fracture with Hardware Failure Molly Hovendick, MAT, ATC, LAT., Northeastern State University Dylan Morris, DO., Oklahoma State University- Center for Health Sciences Matthew O’Brien, PhD, ATC, LAT., Oklahoma State University- Center for Health Sciences Introduction: Humeral shaft fractures account for three to five percent of all fractures. The unique aspect of this case was the patient suffered from a nonunion humeral fracture and subsequently suffered from surgical hardware failure as well. Background: The patient is a right hand dominant 66-year-old male who presented to the emergency department with left arm pain and disability due to a fall from standing height. Initially, he was treated conservatively and placed into a functional brace. At the follow up visit approximately one month later, he reported continued pain and discomfort in his upper extremity. Although there was concern of a possible delayed union due to a history of cigarette smoking and possible noncompliance with post- operative restrictions the patient elected to proceed with open reduction internal fixation (ORIF) the following day. Shortly following surgery, the patient reported a fall reinjuring his left shoulder while mowing his lawn. Previous symptoms were aggravated and signs of hardware failure through the locking plate was suspected. The decision to perform revision ORIF of the fracture using interfragmentary compression plating with lag screw fixation and bone grafting was made and performed approximately seven months following the initial surgery. Discussion: This case report highlights that while the majority of humeral shaft fractures can successfully be treated conservatively, this method may fail and require delayed open reduction internal fixation. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior