Sports-Related Injuries Can Occur As the Result of a Single Traumatic Event, Such As an Impact Or Fall, Or from Repeated Overuse
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Shoulder Injuries: Dislocated Shoulder and Labral Tear
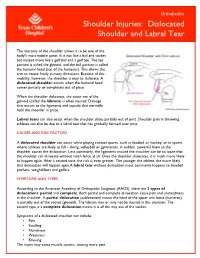
Orthopedics Shoulder Injuries: Dislocated Shoulder and Labral Tear The anatomy of the shoulder allows it to be one of the body's most mobile joints. It is not like a ball and socket but instead more like a golf ball and a golf tee. The tee portion is called the glenoid, and the ball portion is called the humeral head (top of the humerus). This allows the arm to rotate freely in many directions. Because of this mobility, however, the shoulder is easy to dislocate. A dislocated shoulder occurs when the humeral head comes partially or completely out of place. When the shoulder dislocates, the outer rim of the glenoid (called the labrum) is often injured. Damage also occurs to the ligaments and capsule that normally hold the shoulder in place. Labral tears can also occur when the shoulder slides partially out of joint. Shoulder pain in throwing athletes can also be due to a labral tear that has gradually formed over time. CAUSES AND RISK FACTORS A dislocated shoulder can occur while playing contact sports, such as football or hockey, or in sports where athletes are likely to fall – skiing, volleyball or gymnastics. A sudden, powerful blow to the shoulder causes the dislocation. Less commonly, the ligaments around the shoulder can be so loose that the shoulder can dislocate without much force at all. Once the shoulder dislocates, it is much more likely to happen again. After a second time, the risk is even greater. The younger the athlete, the more likely that dislocation will happen again.A labral tear without dislocation most commonly happens to baseball pitchers, weightlifters and golfers. -
The 7 Step Shin Splints Treatment System
The Step SShhiinn SSpplliinnttss Treatment System By Brad Walker TM The 7 Step Shin Splints Treatment System Fix Your Shin Splints Once and For All and get back to Pain Free Running Quickly and Safely. Walker, Bradley E., 1971 7 Step Shin Splints Treatment System™ Copyright © 2012 The Stretching Institute™ All rights reserved. Except under conditions described in the copyright act, no part of this publication may in any form or by any means (electronic, mechanical, micro copying, photocopying, recording or otherwise) be reproduced, stored in a retrieval system or transmitted without prior written permission from the copyright owner. Inquires should be addressed to the publisher. Disclaimers The exercises presented in this publication are intended as an educational resource and are not intended as a substitute for proper medical advice. Please consult your physician, physical therapist or sports coach before performing any of the exercises described in this publication, particularly if you are pregnant, elderly or have any chronic or recurring muscle or joint pain. Discontinue any exercise that causes you pain or severe discomfort and consult a medical expert. Cover picture/s supplied by iStockphoto. The Stretching Institute has purchased the non-exclusive, non-transferable, non-sub licensable right to reproduce the cover picture/s an unlimited number of times in online and electronic publications, and web advertisements. Exercise graphics used with permission from the Physigraphe V2 Pro Clip Art CD-ROM available at ExRx.net. Copyright -
Dislocated Shoulder -Orthoinfo - AAOS Page 1 of 2
Dislocated Shoulder -OrthoInfo - AAOS Page 1 of 2 Dislocated Shoulder The shoulder joint is the body's most mobile joint. It can turn in many directions. But, this advantage also makes the shoulder an easy joint to dislocate. A partial dislocation (subluxation) means the head of the upper arm bone (humerus) is partially out of the socket (glenoid). A complete dislocation means it is all the way out of the socket. Both partial and complete dislocation cause pain and unsteadiness in the shoulder. Shoulder instability Symptoms Symptoms to look for include: • Swelling • Numbness • Weakness • Bruising Sometimes dislocation may tear ligaments or tendons in the shoulder or damage nerves. The shoulder joint can dislocate forward, backward, or downward. A common type of shoulder dislocation is when the shoulder slips forward (anterior instability). This means the upper arm bone moved forward and down out of its joint. It may happen when the arm is put in a throwing position. Diagnosis The muscles may have spasms from the disruption, and this can make it hurt more. When the shoulder dislocates time and again, there is shoulder instability. The doctor will examine the shoulder and may order an X-ray. It is important that the doctor know how the dislocation happened and whether the shoulder had ever been dislocated before. Treatment http://orthoinfo.aaos.org/topic.cfm?topic=A00035 2/2/2015 Dislocated Shoulder -OrthoInfo - AAOS Page 2 of 2 The doctor will place the ball of the upper arm bone (humerus) back into the joint socket. This process is called closed reduction. Severe pain stops almost immediately once the shoulder joint is back in place. -

Ankle Sprains Paediatric Management Advice Leaflet
Ankle Sprains Paediatric Management Advice Leaflet What is a sprained ankle? Ankle sprains occur when the ligaments around the foot and ankle are overstretched during an injury such as sudden twisting, which may cause some fibres to tear. The severity of the sprain will differ depending on how much stretch has occurred. What are the symptoms of a sprain? Pain around the joint. Swelling. Bruising. Pain when walking or moving. Pain relief Consult your GP or local pharmacist for advice as to which medication is suitable for your hil to take. Important signs and symptoms to look out for If your child experiences any of the following symptoms, please seek further urgent medical advice: Significant swelling Worsening, severe pain in the foot and ankle Severe night pain Night sweats Loss of sensation or persistent pins and needles/numbness in the foot/ankle/toes Abnormal weakness in the foot i.e. foot drop Altered colour or unusual sweating of the foot/ ankle Constant giving way or unable to weight bear through the foot/ankle Only continue to read if you have none of the above symptoms Paeds/Ankle sprain/ April 2020/ Page 1 of 4 Recovery and Rehabilitation Healing times Ankle sprains will usually heal within a few weeks with conservative management. Swelling and bruising may still be present for up to 10 days. Normal activity levels are usually restored after 6-8 weeks. The risk of re-injury is higher in the first 4-6 weeks. As your child completes the exercises provided they may notice some swelling and aching. -

Sports Injuries
Sports Injuries Lacrosse Lacrosse is America’s oldest game. It can be dated back to the Native Americans, and was used astraining for war. It is both played by boys and girls,however, some rules are drastically different between genders. Nonetheless, the combination of contact, a stick, a hard ball, and quick changes of direction, puts lacrosse players at risk for injury. Protective Equipment There is a wide range of equipment that lacrosse players wear. For girls, goggles and mouth pieces are mandatory. Lightweight gloves and headgear is optional. For boys, helmets with full face guards, shoulder pads, padded gloves, and mouth pieces are used. It is most important for this equipment to fit properly. If equipment does not fit properly it can actually cause injury. There is no helmet which has been proven through research that confused with a “dislocated shoulder,” which is when prevents concussions. the shoulder comes out of socket. Dislocated shoulders What are the most common types are not common in lacrosse. of lacrosse injuries? Concussions Contusions Concussions are quite common in lacrosse. For more information, please refer to our concussion handout. Because of the nature of the sport, bruises or contusions are very common in lacrosse. Contusions How can lacrosse injuries be prevented? are best initially treated with ice, compression, and elevation of the affected area. • Stay active year round Knee Injuries • Incorporate strength training and stretching into your normal routine Lacrosse players commonly injure their knees. Sprains of the medial and lateral collateral ligaments • Wear properly fitted equipment (MCL/LCL) occur. More serious injuries of the anterior and posterior cruciate ligaments (ACL/PCL) and to the • Hydrate adequately before, during, and menisci (cartilage of the knee) can also happen. -

MUSCULOSKELETAL MRI Temporomandibular Joints (TMJ) Temporomandibular Joints (TMJ) MRI - W/O Contrast
MUSCULOSKELETAL MRI Temporomandibular Joints (TMJ) Temporomandibular joints (TMJ) MRI - W/O Contrast . CPT Code 70336 • Arthritis • TMJ disc abnormality • Osteonecrosis (AVN) Temporomandibular joints (TMJ) MRI - W and W/O Contrast . CPT Code 70336 • Arthritis/Synovitis • Mass/Tumor Chest Chest Wall/Rib, Sternum, Bilateral Pectoralis Muscles, Bilateral Clavicles MRI - W/O Contrast . CPT Code 71550 • Rib fracture, costochondral cartilage injury • Muscle, tendon or nerve injury Chest Wall/Rib, Sternum, Bilateral Pectoralis Muscles, Bilateral Clavicles MRI - W and W/O Contrast . CPT Code 71552 • Mass/Tumor • Infection Upper Extremity (Non-Joint) Scapula MRI - W/O Contrast . CPT Code 73218 • Fracture • Muscle, tendon or nerve injury Scapula MRI - W and W/O Contrast . CPT code 73220 • Mass/Tumor • Infection Humerus, Arm MRI - W/O Contrast . CPT Code 73218 • Fracture • Muscle, tendon or nerve injury Humerus, Arm MRI - W and W/O Contrast . CPT Code 73220 • Mass/Tumor • Infection Forearm MRI - W/O Contrast . CPT Code 73218 • Fracture • Muscle, tendon or nerve injury Forearm MRI - W and W/O Contrast . CPT Code 73220 • Mass/Tumor • Infection Hand MRI - W/O Contrast. CPT Code 73218 • Fracture • Muscle, tendon or nerve injury Hand MRI - W and W/O Contrast . CPT Code 73220 • Mass/Tumor • Infection • Tenosynovitis Finger(s) MRI - W/O Contrast. CPT Code 73218 • Fracture • Muscle, tendon or nerve injury Finger(s) MRI - W and W/O Contrast . CPT Code 73220 • Mass/Tumor • Infection • Tenosynovitis Upper Extremity (Joint) Shoulder MRI - W/O Contrast. CPT Code 73221 • Muscle, tendon (rotator cuff) or nerve injury • Fracture • Osteoarthritis Shoulder MRI - W Contrast (Arthrogram only; no IV contrast) . CPT Code 73222 • Labral (SLAP) tear • Rotator cuff tear Shoulder MRI - W and W/O Contrast . -

Meniscus Tear
291 North Fireweed Soldotna, AK 99669 907-262-6454 www.kenaipeninsulaortho.com ______________________________________________________________________________________ Orthopaedic Surgeon: Hand and Wrist Specialist: Henry G. Krull, M.D. Edwin D. Vyhmeister, M.D. Meniscus Tear The meniscus is the rubbery, soft cartilage cushion in the knee. There are two of the C-shaped cushions in each knee, a medial (inner) and lateral (outer) meniscus. They sit between the two bones that form the knee joint, and function to cushion and support the knee. The meniscus can tear with injury or degeneration, or a combination of both. The medial meniscus is torn about 10X more frequently than the lateral meniscus. In young people, the meniscus usually tears with an injury. In older people, the cartilage can degenerate (weaken) with age, and can tear with or without an injury; spontaneous tears can occur. Meniscal tears can occur in association with other injuries to the knee. Symptoms: Pain is the usual symptom of complaint with a meniscus tear. There is often a noticeable “pop.” Swelling and stiffness can also occur. Mechanical symptoms are common—clicking, popping, and locking. Sometimes there is just a feeling that something is wrong inside the knee. Pain can be sharp, or can be dull and aching. Meniscus tears do not heal, but sometimes the symptoms dissipate. Chronic, intermittent symptoms is very common. Meniscal tears can cause a feeling of instability, or can cause the knee to buckle or give way. Cause: Injuries, particularly with sports, are a common cause of meniscal tears in young people. As people age, the meniscus tissue weakens through the normal degenerative process, and tears can occur spontaneously, or with simple activities, such as getting up from a chair, and changing direction while walking. -

Regenexx Corporate Brochure
COMMON CONDITIONS TREATED • neck and back bulging, collapsed, herniated, ruptured, slipped, or torn disc; degenerative disc disease; disc extrusion or protrusion; chronic back, neck, disc, or nerve pain • shoulder arthritis, labral tear or degeneration, recurrent shoulder dislocation, rotator cuff tear, rotator cuff tendonitis, joint replacement • elbow arthritis, instability, nerve entrapment (ulnar nerve), tennis elbow or golfer’s elbow • hand and wrist arthritis, carpal tunnel syndrome, instability, trigger finger, cml joint • hip arthritis, osteonecrosis, bursitis, labral/labrum tear, tendinopathy, joint replacement, avascular necrosis • knee arthritis; instability; sprain or tear of the ACL/PCL, MCL/LCL; meniscus tear, tendinopathy, joint replacement • ankle and foot instability, arthritis, bunions, ligament sprain or tear, plantar fasciitis, achilles tendinopathy Regenexx is the pioneer of interventional orthopedic National Clinic Network to Support Client treatments for musculoskeletal conditions in the Needs United States. These non-surgical procedures use a • FDA Compliant (CFR21 Part 1271) patient’s adult stem cells or blood platelets to initiate • Standardized Procedures and Protocol Quality healing of damaged tissues, tendons, ligaments, Assurance Program cartilage, spinal disc and bone. Our orthobiologic • Nationwide network of clinics and physicians to approach is the result of scientific advancements to support corporate client operations heal orthopedic injuries, treat arthritis and repair • Flexible Lab Platform delivering multiple joint degenerative conditions without the need for customized protocols surgery. • Experienced partners with self-funded companies Regenexx procedures use precisely guided, needle Research and Data Driven To Continuously based injections to concentrate healing factors in Improve Efficacy the precise area of damage while leaving a patient’s • Published over 30 times more research than any musculoskeletal structure intact. -

Common Disorders of the Knee
7/27/2017 Common Disorders of Disclosures the Knee Carlin Senter, MD I have nothing to disclose. Associate Professor Primary Care Sports Medicine UCSF Medicine and Orthopaedics UCSF Essentials of Primary Care August 8, 2017 Knee: Top 3 referral diagnoses from Objectives primary care IM to ortho (at UCSF in 2011) 1. Osteoarthritis (OA) Upon completion of this session, participants should be able to: 2. Anterior knee pain 1. List 4 exam maneuvers for meniscus tear • Patellofemoral pain syndrome 2. List the diagnostic criteria for knee OA • Chondromalacia patella 3. Identify 5 non operative treatment options for knee OA • Patellar tendinopathy 4. Identify indications for surgery for patient with meniscus tear 3. Meniscus tear ‒ Without knee OA ‒ With knee OA 5. Generate a differential diagnosis for chronic anterior knee pain 1 7/27/2017 Case #1 All of the following tests, if positive, would raise concern for a meniscus tear except… 25 y/o man with medial-sided pain and swelling of the R knee for 6 A. Joint line tenderness weeks since he twisted the knee playing soccer. No locking, no instability. B. Pain when he stands and pivots on the knee C. Pain when you axially load and rotate the knee D. Pain when you flex the R knee and extend the R hip with the patient lying on his left side. E. Pain when he squats 4 tests for meniscus tear Joint line tenderness 1. Isolated joint line tenderness 2. McMurray 3. Thessaly 4. Squat Medial: Sensitivity 83%, Specificity 76% Lateral: Sensitivity 68%, Specificity 97% (Konan et al. -

Ankle Sprain
ANKLE SPRAIN What Is an Ankle Sprain? n ankle sprain is an injury to Anterior talofibular one or more ligaments in the Posterior A ligament ankle, usually on the outside of the talofibular ligament ankle. Ligaments are bands of tissue—like rubber bands—that Calcaneofibular ligament connect one bone to another and bind the joints together. In the ankle joint, ligaments provide stability by shoes, or walking or running on an surgeon for an appointment as limiting side-to-side movement. uneven surface. soon as possible. In the meantime, Some ankle sprains are much Sometimes ankle sprains occur immediately begin using the “R.I.C.E.” worse than others. The severity of because of weak ankles, a condition method—Rest, Ice, Compression, an ankle sprain depends on whether that some people are born with. and Elevation—to help reduce the ligament is stretched, partially Previous ankle or foot injuries can also swelling, pain, and further injury. torn, or completely torn, as well as on weaken the ankle and lead to sprains. the number of ligaments involved. Why Prompt Medical Ankle sprains are not the same as Signs and Symptoms Attention Is Needed strains, which affect muscles rather The signs and symptoms of ankle There are four key reasons why an than ligaments. sprains may include: ankle sprain should be promptly •Pain or soreness evaluated and treated by a foot and What Causes a •Swelling ankle surgeon: Sprained Ankle? • Bruising • First, an untreated ankle sprain Sprained ankles often result from a • Difficulty walking may lead to chronic ankle fall, a sudden twist, or a blow that • Stiffness in the joint instability,a condition marked by forces the ankle joint out of its persistent discomfort and a “giving normal position. -

Shin Splints
A Patient’s Guide to Shin Splints Orthopedic and Sports Physical Therapy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 Compliments of: Orthopedic and Sports Physical Therapy DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments orA treatments.Patient's The information Guide shouldto Shin NOT be Splints used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. Orthopedic and Sports Physical Therapy Thank you for requesting your Orthopaedic and Sports Physical Therapy Patient Guide and giving us the opportunity to help you better understand your condition. Once you've had a chance to review the information provided, you may have additional questions. If that's the case, we would like to offer you a FREE consultation to discuss your condition more fully, answer all of your questions, and give you our best advice on how you can resolve your pain quickly and easily. To arrange your FREE consultation, please contact us at 337.232.5301 and begin feeling good again! Call today and begin feeling better tomorrow. The OSPT Team Orthopedic and Sports Physical Therapy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 www.ospt.net All materials within these pages are the sole property of Medical Multimedia Group, LLC and are used herein by permission. -

Physical Examination of the Knee: Meniscus, Cartilage, and Patellofemoral Conditions
Review Article Physical Examination of the Knee: Meniscus, Cartilage, and Patellofemoral Conditions Abstract Robert D. Bronstein, MD The knee is one of the most commonly injured joints in the body. Its Joseph C. Schaffer, MD superficial anatomy enables diagnosis of the injury through a thorough history and physical examination. Examination techniques for the knee described decades ago are still useful, as are more recently developed tests. Proper use of these techniques requires understanding of the anatomy and biomechanical principles of the knee as well as the pathophysiology of the injuries, including tears to the menisci and extensor mechanism, patellofemoral conditions, and osteochondritis dissecans. Nevertheless, the clinical validity and accuracy of the diagnostic tests vary. Advanced imaging studies may be useful adjuncts. ecause of its location and func- We have previously described the Btion, the knee is one of the most ligamentous examination.1 frequently injured joints in the body. Diagnosis of an injury General Examination requires a thorough knowledge of the anatomy and biomechanics of When a patient reports a knee injury, the joint. Many of the tests cur- the clinician should first obtain a rently used to help diagnose the good history. The location of the pain injured structures of the knee and any mechanical symptoms were developed before the avail- should be elicited, along with the ability of advanced imaging. How- mechanism of injury. From these From the Division of Sports Medicine, ever, several of these examinations descriptions, the structures that may Department of Orthopaedics, are as accurate or, in some cases, University of Rochester School of have been stressed or compressed can Medicine and Dentistry, Rochester, more accurate than state-of-the-art be determined and a differential NY.