Towards a Tourism and Community-Development Framework: an African Perspective
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bulawayo City Mpilo Central Hospital
Province District Name of Site Bulawayo Bulawayo City E. F. Watson Clinic Bulawayo Bulawayo City Mpilo Central Hospital Bulawayo Bulawayo City Nkulumane Clinic Bulawayo Bulawayo City United Bulawayo Hospital Manicaland Buhera Birchenough Bridge Hospital Manicaland Buhera Murambinda Mission Hospital Manicaland Chipinge Chipinge District Hospital Manicaland Makoni Rusape District Hospital Manicaland Mutare Mutare Provincial Hospital Manicaland Mutasa Bonda Mission Hospital Manicaland Mutasa Hauna District Hospital Harare Chitungwiza Chitungwiza Central Hospital Harare Chitungwiza CITIMED Clinic Masvingo Chiredzi Chikombedzi Mission Hospital Masvingo Chiredzi Chiredzi District Hospital Masvingo Chivi Chivi District Hospital Masvingo Gutu Chimombe Rural Hospital Masvingo Gutu Chinyika Rural Hospital Masvingo Gutu Chitando Rural Health Centre Masvingo Gutu Gutu Mission Hospital Masvingo Gutu Gutu Rural Hospital Masvingo Gutu Mukaro Mission Hospital Masvingo Masvingo Masvingo Provincial Hospital Masvingo Masvingo Morgenster Mission Hospital Masvingo Mwenezi Matibi Mission Hospital Masvingo Mwenezi Neshuro District Hospital Masvingo Zaka Musiso Mission Hospital Masvingo Zaka Ndanga District Hospital Matabeleland South Beitbridge Beitbridge District Hospital Matabeleland South Gwanda Gwanda Provincial Hospital Matabeleland South Insiza Filabusi District Hospital Matabeleland South Mangwe Plumtree District Hospital Matabeleland South Mangwe St Annes Mission Hospital (Brunapeg) Matabeleland South Matobo Maphisa District Hospital Matabeleland South Umzingwane Esigodini District Hospital Midlands Gokwe South Gokwe South District Hospital Midlands Gweru Gweru Provincial Hospital Midlands Kwekwe Kwekwe General Hospital Midlands Kwekwe Silobela District Hospital Midlands Mberengwa Mberengwa District Hospital . -

The Spatial Dimension of Socio-Economic Development in Zimbabwe
THE SPATIAL DIMENSION OF SOCIO-ECONOMIC DEVELOPMENT IN ZIMBABWE by EVANS CHAZIRENI Submitted in fulfillment of the requirements for the degree of MASTER OF ARTS in the subject GEOGRAPHY at the UNIVERSITY OF SOUTH AFRICA SUPERVISOR: MRS AC HARMSE NOVEMBER 2003 1 Table of Contents List of figures 7 List of tables 8 Acknowledgements 10 Abstract 11 Chapter 1: Introduction, problem statement and method 1.1 Introduction 12 1.2 Statement of the problem 12 1.3 Objectives of the study 13 1.4 Geography and economic development 14 1.4.1 Economic geography 14 1.4.2 Paradigms in Economic Geography 16 1.4.3 Development paradigms 19 1.5 The spatial economy 21 1.5.1 Unequal development in space 22 1.5.2 The core-periphery model 22 1.5.3 Development strategies 23 1.6 Research design and methodology 26 1.6.1 Objectives of the research 26 1.6.2 Research method 27 1.6.3 Study area 27 1.6.4 Time period 30 1.6.5 Data gathering 30 1.6.6 Data analysis 31 1.7 Organisation of the thesis 32 2 Chapter 2: Spatial Economic development: Theory, Policy and practice 2.1 Introduction 34 2.2. Spatial economic development 34 2.3. Models of spatial economic development 36 2.3.1. The core-periphery model 37 2.3.2 Model of development regions 39 2.3.2.1 Core region 41 2.3.2.2 Upward transitional region 41 2.3.2.3 Resource frontier region 42 2.3.2.4 Downward transitional regions 43 2.3.2.5 Special problem region 44 2.3.3 Application of the model of development regions 44 2.3.3.1 Application of the model in Venezuela 44 2.3.3.2 Application of the model in South Africa 46 2.3.3.3 Application of the model in Swaziland 49 2.4. -

Fact Sheet #14, Fiscal Year (Fy) 2019 August 12, 2019
SOUTHERN AFRICA – TROPICAL CYCLONES FACT SHEET #14, FISCAL YEAR (FY) 2019 AUGUST 12, 2019 NUMBERS AT HIGHLIGHTS HUMANITARIAN FUNDING A GLANCE Cyclone-affected areas of Mozambique, FOR THE SOUTHERN AFRICA CYCLONES & FLOODS RESPONSE IN FY 2019 Zimbabwe face acute food insecurity USAID/OFDA1 $52,789,705 More than 75,000 people remain 960 displaced in cyclone-affected areas of Number of Confirmed USAID/FFP2 $38,658,852 Mozambique as of July Deaths in Mozambique, Zimbabwe, and Malawi From Humanitarian access remains limited in 3 Tropical Cyclone Idai northern Mozambique due to ongoing State/PRM $1,500,000 OCHA – April 2019 insecurity and damaged infrastructure DoD4 $5,995,078 45 following Tropical Cyclone Kenneth $98,943,635 Number of Confirmed Deaths in Mozambique From Tropical Cyclone Kenneth GRM – May 2019 KEY DEVELOPMENTS Food security actors estimate that approximately 1.65 million people in Mozambique are 7 experiencing acute food insecurity caused by cyclone damage, drought, crop pests, and insecurity, according to the Integrated Food Security Phase Classification (IPC). In Number of Confirmed Deaths in Comoros From Zimbabwe, nearly 2.3 million people across most of the country are experiencing severe Tropical Cyclone Kenneth acute food insecurity earlier than usual due to poor crop production, compounded by Government of the Union of Comoros damage caused by Tropical Cyclone Idai in southeastern parts of the country, as well as – May 2019 Zimbabwe’s ongoing economic crisis. Food security outcomes in Mozambique, Zimbabwe, and southern Malawi are expected to deteriorate through March, the typical 1.65 end of the lean season. Tropical cyclones Idai and Kenneth—which made landfall in Mozambique on March 15 million and April 25, respectively—destroyed approximately 79,000 houses in the country, the UN reports. -

Promotion of Climate-Resilient Lifestyles Among Rural Families in Gutu
Promotion of climate-resilient lifestyles among rural families in Gutu (Masvingo Province), Mutasa (Manicaland Province) and Shamva (Mashonaland Central Province) Districts | Zimbabwe Sahara and Sahel Observatory 26 November 2019 Promotion of climate-resilient lifestyles among rural families in Gutu Project/Programme title: (Masvingo Province), Mutasa (Manicaland Province) and Shamva (Mashonaland Central Province) Districts Country(ies): Zimbabwe National Designated Climate Change Management Department, Ministry of Authority(ies) (NDA): Environment, Water and Climate Development Aid from People to People in Zimbabwe (DAPP Executing Entities: Zimbabwe) Accredited Entity(ies) (AE): Sahara and Sahel Observatory Date of first submission/ 7/19/2019 V.1 version number: Date of current submission/ 11/26/2019 V.2 version number A. Project / Programme Information (max. 1 page) ☒ Project ☒ Public sector A.2. Public or A.1. Project or programme A.3 RFP Not applicable private sector ☐ Programme ☐ Private sector Mitigation: Reduced emissions from: ☐ Energy access and power generation: 0% ☐ Low emission transport: 0% ☐ Buildings, cities and industries and appliances: 0% A.4. Indicate the result ☒ Forestry and land use: 25% areas for the project/programme Adaptation: Increased resilience of: ☒ Most vulnerable people and communities: 25% ☒ Health and well-being, and food and water security: 25% ☐ Infrastructure and built environment: 0% ☒ Ecosystem and ecosystem services: 25% A.5.1. Estimated mitigation impact 399,223 tCO2eq (tCO2eq over project lifespan) A.5.2. Estimated adaptation impact 12,000 direct beneficiaries (number of direct beneficiaries) A.5. Impact potential A.5.3. Estimated adaptation impact 40,000 indirect beneficiaries (number of indirect beneficiaries) A.5.4. Estimated adaptation impact 0.28% of the country’s total population (% of total population) A.6. -
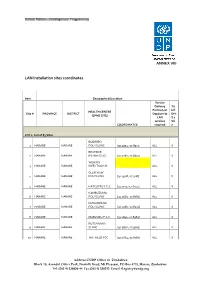
LAN Installation Sites Coordinates
ANNEX VIII LAN Installation sites coordinates Item Geographical/Location Service Delivery Tic Points (List k if HEALTH CENTRE Site # PROVINCE DISTRICT Dept/umits DHI (EPMS SITE) LAN S 2 services Sit COORDINATES required e LOT 1: List of 83 Sites BUDIRIRO 1 HARARE HARARE POLYCLINIC [30.9354,-17.8912] ALL X BEATRICE 2 HARARE HARARE RD.INFECTIO [31.0282,-17.8601] ALL X WILKINS 3 HARARE HARARE INFECTIOUS H ALL X GLEN VIEW 4 HARARE HARARE POLYCLINIC [30.9508,-17.908] ALL X 5 HARARE HARARE HATCLIFFE P.C.C. [31.1075,-17.6974] ALL X KAMBUZUMA 6 HARARE HARARE POLYCLINIC [30.9683,-17.8581] ALL X KUWADZANA 7 HARARE HARARE POLYCLINIC [30.9285,-17.8323] ALL X 8 HARARE HARARE MABVUKU P.C.C. [31.1841,-17.8389] ALL X RUTSANANA 9 HARARE HARARE CLINIC [30.9861,-17.9065] ALL X 10 HARARE HARARE HATFIELD PCC [31.0864,-17.8787] ALL X Address UNDP Office in Zimbabwe Block 10, Arundel Office Park, Norfolk Road, Mt Pleasant, PO Box 4775, Harare, Zimbabwe Tel: (263 4) 338836-44 Fax:(263 4) 338292 Email: [email protected] NEWLANDS 11 HARARE HARARE CLINIC ALL X SEKE SOUTH 12 HARARE CHITUNGWIZA CLINIC [31.0763,-18.0314] ALL X SEKE NORTH 13 HARARE CHITUNGWIZA CLINIC [31.0943,-18.0152] ALL X 14 HARARE CHITUNGWIZA ST.MARYS CLINIC [31.0427,-17.9947] ALL X 15 HARARE CHITUNGWIZA ZENGEZA CLINIC [31.0582,-18.0066] ALL X CHITUNGWIZA CENTRAL 16 HARARE CHITUNGWIZA HOSPITAL [31.0628,-18.0176] ALL X HARARE CENTRAL 17 HARARE HARARE HOSPITAL [31.0128,-17.8609] ALL X PARIRENYATWA CENTRAL 18 HARARE HARARE HOSPITAL [30.0433,-17.8122] ALL X MURAMBINDA [31.65555953980,- 19 MANICALAND -

Cultural Practices Associated with Death in the North Nyanga District of Zimbabwe and Their Impact on Widows and Orphans +
The African e-Journals Project has digitized full text of articles of eleven social science and humanities journals. This item is from the digital archive maintained by Michigan State University Library. Find more at: http://digital.lib.msu.edu/projects/africanjournals/ Available through a partnership with Scroll down to read the article. Journal of Social Development in Africa (1996), 11,1, 79-86 Cultural Practices Associated with Death in the North Nyanga District of Zimbabwe and their Impact on Widows and Orphans + DREW, R S *; FOSTER, G *; CHITIMA, J ** ABSTRACT This survey examines the cultural practices associated with death in the Nyanga North area of Zimbabwe and their impact on widows and orphans in 211 families. In addition to the concepts of pre-planning for death, property and wife inheritance, relevant aspects of life such as marriage, patriarchal succession and sickness are also considered. It is unclear what pattern of care and support for widows is emerging to replace the declining practice of wife inheritance. The implication of these factors on the planning of effective intervention strategies is considered. Introduction AIDS has been spreading rapidly through Zimbabwe as in other sub-Saharan African countries. Serosurveillance studies (MOH, 1993) carried out in antenatal mothers have shown HIV prevalence levels of over 30% in urban areas and around 20% in rural areas. The Elim Pentecostal Church of Zimbabwe (EPCZ) administers a church centre in the communal lands in the northern part of Nyanga District in the north-eastern part of Zimbabwe close to the border with Mozambique. This centre provides educational and health services to the community in the surrounding area. -
Blue Swallow Survey Report November
Blue Swallow Survey Report November 2013- March 2014 By Fadzai Matsvimbo (BirdLife Zimbabwe) with assistance from Tendai Wachi ( Zimbabwe Parks and Wildlife Management Authority) Background The Blue Swallow Hirundo atrocaerulea is one of Africa’s endemics, migrating between East and Central to Southern Africa where it breeds in the summer. These breeding grounds are in Zimbabwe, South Africa, Swaziland, Mozambique, Malawi, southern Tanzania and south eastern Zaire, Zambia. The bird winters in northern Uganda, north eastern Zaire and Western Kenya (Keith et al 1992).These intra-african migrants arrive the first week of September and depart in April In Zimbabwe (Snell 1963.).There are reports of the birds returning to their wintering grounds in May (Tree 1990). In Zimbabwe, the birds are restricted to the Eastern Highlands where they occur in the Afromontane grasslands. The Blue Swallow is distributed from Nyanga Highlands southwards through to Chimanimani Mountains and are known to breed from 1500m - 2200m (Irwin 1981). Montane grassland with streams forming shallow valleys and the streams periodically disappearing underground and forming shallow valleys is the preferred habitat (Snell 1979). Whilst birds have been have only ever been located in the Eastern Highlands there is a solitary record from then Salisbury now Harare (Brooke 1962). The Blue Swallow is a medium sized swallow of about 20- 25 cm in body length. The males and females can be told apart by the presence of the long tail retrices in the male. The tail streamers in the males measure twice as long as the females (Maclean 1993). The adults are a shiny blue-black with a black tail with blue green gloss and whitish feather shafts. -

Zimbabwe Market Study: Masvingo Province Report
©REUTERS/Philimon Bulawayo Bulawayo ©REUTERS/Philimon R E S E A R C H T E C H N I C A L A S S I S T A N C E C E N T E R January 2020 Zimbabwe Market Study: Masvingo Province Report Dominica Chingarande, Gift Mugano, Godfrey Chagwiza, Mabel Hungwe Acknowledgments The Research team expresses its gratitude to the various stakeholders who participated in this study in different capacities. Special gratitude goes to the District Food and Nutrition Committee members, the District Drought Relief Committee members, and various market actors in the province for providing invaluable local market information. We further express our gratitude to the ENSURE team in Masvingo for mobilizing beneficiaries of food assistance who in turn shared their lived experiences with food assistance. To these food assistance beneficiaries, we say thank you for freely sharing your experiences. Research Technical Assistance Center The Research Technical Assistance Center is a world-class research consortium of higher education institutions, generating rapid research for USAID to promote evidence-based policies and programs. The project is led by NORC at the University of Chicago in partnership with Arizona State University, Centro de Investigacin de la Universidad del Pacifico (Lima, Peru), Davis Management Group, the DevLab@Duke University, Forum One, the Institute of International Education, the Notre Dame Initiative for Global Development, Population Reference Bureau, the Resilient Africa Network at Makerere University (Kampala, Uganda), the United Negro College Fund, the University of Chicago, and the University of Illinois at Chicago. The Research Technical Assistance Center (RTAC) is made possible by the generous support of the American people through the United States Agency for International Development (USAID) under the terms of contract no. -
Census Results in Brief
116 Appendix 1a: Census Questionnaire 117 118 119 120 Appendix 1b: Census Questionnaire Code List Question 6-8 and 10 Census District Country code MANICALAND 1 Sanyati 407 Shurugwi 726 Rural Districts Urban Areas MASVINGO 8 Buhera 101 Chinhoyi 421 Rural Districts Chimanimani 102 Kadoma 422 Bikita 801 Chipinge 103 Chegutu 423 Chiredzi 802 Makoni 104 Kariba 424 Chivi 803 Mutare Rural 105 Norton 425 Gutu 804 Mutasa 106 Karoi 426 Masvingo Rural 805 Nyanga 107 MATABELELAND NORTH 5 Mwenezi 806 Urban Areas Rural Districts Zaka 807 Mutare 121 Binga 501 Urban Areas Rusape 122 Bubi 502 Masvingo Urban 821 Chipinge 123 Hwange 503 Chiredzi Town 822 MASHONALAND CENTRAL 2 Lupane 504 Rural Districts Nkayi 505 HARARE 9 Bindura 201 Tsholotsho 506 Harare Rural 901 Centenary 202 Umguza 507 Harare Urban 921 Guruve 203 Urban Areas Chitungwiza 922 Mazowe 204 Hwange 521 Epworth 923 Mount Darwin 205 Victoria Falls 522 BULAWAYO 0 Rushinga 206 MATABELELAND SOUTH 6 Bulawayo Urban 21 Shamva 207 Rural Districts AFRICAN COUNTRIES Mbire 208 Beitbridge Rural 601 Zimbabwe 0 Urban Areas Bulilima 602 Botswana 941 Bindura 221 Mangwe 603 Malawi 942 Mvurwi 222 Gwanda Rural 604 Mozambique 943 MASHONALAND EAST 3 Insiza 605 South Africa 944 Rural Districts Matobo 606 Zambia 945 Chikomba 301 Umzingwane 607 Other African Countries 949 Goromonzi 302 Urban Areas OUTSIDE AFRICA Hwedza 303 Gwanda 621 United Kingdom 951 Marondera 304 Beitbridge Urban 622 Other European Countries 952 Mudzi 305 Plumtree 623 American Countries 953 Murehwa 306 MIDLANDS 7 Asian Countries 954 Mutoko 307 Rural Districts Other Countries 959 701 Seke 308 Chirumhanzu Uzumba-Maramba-Pfungwe 309 Gokwe North 702 Urban Areas Gokwe South 703 Marondera 321 Gweru Rural 704 Chivhu Town Board 322 Kwekwe Rural 705 Ruwa Local Board 323 Mberengwa 706 MASHONALAND WEST 4 Shurugwi 707 Rural Districts Zvishavane 708 Chegutu 401 Urban Areas Hurungwe 402 Gweru 721 Mhondoro-Ngezi 403 Kwekwe 722 Kariba 404 Redcliff 723 Makonde 405 Zvishavane 724 Gokwe Centre 725 . -

Zimbabwean Government Gazette
ZIMBABWEAN GOVERNMENT GAZETTE Publishedby Authority Vol. LXVI,No. 11 : 26th FEBRUARY, 1988 . Price 40¢, General Notice 115of 1988. a ‘{c) depart Sagambe- Saturday 5 am., atrive Mutare - ROAD MOTOR TRANSPORTATION ACT [CHAPTER262] . 9,20. 2.02.5 . 7 (d) depart. Sagambe Sunday 10 am., arrive Harare Applications in Connexion 715 pm So o with Road ServicePermits (e) depart Harare Monday,Wednesday: and Friday 6 a.m., . arrive Sagambe 3.15 p.m.; Po . IN terms of ‘subsection (4) of section 7 of the Road Motor | (f) depart Mutare Thursday and Saturday 10.50 a.m., arrive Transportation Act [Chapter 262], notice is-hereby. giventhat .Sagambe 3.15 p.m. Ss . the applications. detailed in the ‘Schédule, for the issue or The _. amendment of road service .permits, have been received for the service to operate as follows— | ~ “eonsideration of the Controller ‘of. Road.Motor ‘Transportation. (a). depart Sagambe Tuesday andThursday 4 am, atrive — Harare 12,30 p.m.; Any personwishing to object to:any ‘such: application must lodge with the Controller of {b) depart Sagambe Saturday 5 am., arrive Mutare Road Motor’ Transportation, 8.45 a.m; P.O. Box 8332, Causeway-— oe . ‘(c) depart Sagambe Sunday 7.a.m., arrive Harare 3.30 p.m; {a) a notice, in writing, of hie intention to object, soas to (d) depart Harare Monday andWednesday 6 a.m., arrive ~ yeach the Controller’s office not later than the 18th Sagambe3.15 ip.m.; . March, :.1988; @ depart Harare Friday 4 p.m., arrive Sagambe ‘Saturday (b) his’ objection and the grounds therefor, on form R.M.T. -

Zimbabwe HIV Care and Treatment Project Baseline Assessment Report
20 16 Zimbabwe HIV Care and Treatment Project Baseline Assessment Report '' CARG members in Chipinge meet for drug refill in the community. Photo Credits// FHI 360 Zimbabwe'' This study is made possible through the support of the American People through the United States Agency for International Development (USAID.) The contents are the sole responsibility of the Zimbabwe HIV care and Treatment (ZHCT) Project and do not necessarily reflect the views of USAID or the U.S. Government. FOREWORD The Government of Zimbabwe (GoZ) through the Ministry of Health and Child Care (MoHCC) is committed to strengthening the linkages between public health facilities and communities for HIV prevention, care and treatment services provision in Zimbabwe. The Ministry acknowledges the complementary efforts of non-governmental organisations in consolidating and scaling up community based initiatives towards achieving the UNAIDS ‘90-90-90’ targets aimed at ending AIDS by 2030. The contribution by Family Health International (FHI360) through the Zimbabwe HIV Care and Treatment (ZHCT) project aimed at increasing the availability and quality of care and treatment services for persons living with HIV (PLHIV), primarily through community based interventions is therefore, lauded and acknowledged by the Ministry. As part of the multi-sectoral response led by the Government of Zimbabwe (GOZ), we believe the input of the ZHCT project will strengthen community-based service delivery, an integral part of the response to HIV. The Ministry of Health and Child Care however, has noted the paucity of data on the cascade of HIV treatment and care services provided at community level and the ZHCT baseline and mapping assessment provides valuable baseline information which will be used to measure progress in this regard. -

DCA in Zimbabwe
Zimbabwe OPERATIONAL CONTEXT AND KEY RESULTS: DanChurchAid is working in Zimbabwe, a country facing the serious negative impact of climate change, protracted economic and political crisis. In response to the operational context DCA works with local implementing local partners to achieve the following: Resilience building, supporting 48.000 households translating to approximately 240.000 individuals Climate change related disaster response including drought and cyclones 240 000 individuals Interventions to address Food Insecurity facing 29.000 individuals. These include cash transfers to improve food purchasing power in peri-urban settings such as Epworth near Harare DCA works with partners in supporting smallholder farmers to enhance food and income security, reaching a total of 48 000 households FACTS: In 2019 DCA in coordination with other agencies fed 5 million people facing ● DCA operated in Zimbabwe from the early to the late 1980s providing food shortages in both rural and urban settings support to refugees following the war of independence. In 2014, DCA reopened its offices to respond to the worsening economic and DCA is working with churches to promote social cohesion humanitarian situation in the country. through peace building initiatives ● Offices in country: The country office is in Harare, with a field office located in Bulawayo. WHAT WE DO: ● Beneficiaries in 2019: 240 000 individuals In Zimbabwe DCA focuses primarily on three programmatic areas namely; ● Turnover in 2019: EUR 5,973,687 ● Projects: 9 Right to Food: DCA supports smallholder farmer households to improve production and productivity while ● Employees: 58 mainstreaming resilience building, value chain development, climate change adaptation and mitigation. ● Partners: Future of Hope Foundation, Pro Africa, Institute for Rural Technologies (IRT), Organisation of Rural Associations for Progress Humanitarian Work: In Zimbabwe, DCA supports individuals affected by disasters including drought, flooding and (ORAP), ProAfrica, CCBICA, Midlands State University.