Axial Skeleton Study Guide
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diapositiva 1
Thoracic Cage and Thoracic Inlet Professor Dr. Mario Edgar Fernández. Parts of the body The Thorax Is the part of the trunk betwen the neck and abdomen. Commonly the term chest is used as a synonym for thorax, but it is incorrect. Consisting of the thoracic cavity, its contents, and the wall that surrounds it. The thoracic cavity is divided into 3 compartments: The central mediastinus. And the right and left pulmonary cavities. Thoracic Cage The thoracic skeleton forms the osteocartilaginous thoracic cage. Anterior view. Thoracic Cage Posterior view. Summary: 1. Bones of thoracic cage: (thoracic vertebrae, ribs, and sternum). 2. Joints of thoracic cage: (intervertebral joints, costovertebral joints, and sternocostal joints) 3. Movements of thoracic wall. 4. Thoracic cage. Thoracic apertures: (superior thoracic aperture or thoracic inlet, and inferior thoracic aperture). Goals of the classes Identify and describe the bones of the thoracic cage. Identify and describe the joints of thoracic cage. Describe de thoracic cage. Describe the thoracic inlet and identify the structures passing through. Vertebral Column or Spine 7 cervical. 12 thoracic. 5 lumbar. 5 sacral 3-4 coccygeal Vertebrae That bones are irregular, 33 in number, and received the names acording to the position which they occupy. The vertebrae in the upper 3 regions of spine are separate throughout the whole of life, but in sacral anda coccygeal regions are in the adult firmly united in 2 differents bones: sacrum and coccyx. Thoracic vertebrae Each vertebrae consist of 2 essential parts: An anterior solid segment: vertebral body. The arch is posterior an formed of 2 pedicles, 2 laminae supporting 7 processes, and surrounding a vertebral foramen. -

Anatomical and Morphometric Study of Optic Foramen in North Indian Population
Published online: 26.06.2019 THIEME Original Article 53 Anatomical and Morphometric Study of Optic Foramen in North Indian Population Ajay Kumar1 Alok Tripathi1 Shilpi Jain1 Satyam Khare1 Ram Kumar Kaushik1 Hina Kausar1 Saurabh Arora1 1Department of Anatomy, Subharti Medical College, Swami Address for correspondence Alok Tripathi, MS, Department of Vivekanand Subharti, University, Meerut, Uttar Pradesh, India Anatomy, Subharti Medical College, Swami Vivekanand Subharti University, Meerut 250005, Uttar Pradesh, India (e-mail: [email protected]). Natl J Clin Anat 2019;8:53–56 Abstract Introduction Optic canal connects orbit to middle cranial fossa. Optic nerve and ophthalmic artery pass through this canal. The aim of the present study is to make morphometric and anatomical observations of endocranial opening of optic canal. Materials and Methods The observations were conducted on 30 dry adult human skulls. The observations were made on shape, margins, confluence, septations, dimensions, and distance of optic foramen from apex of petrous temporal bone. Result and Statistical Analysis On morphometric observation, transverse diameter (TD) was 6.00 mm and 6.15 mm on the left and the right side, respectively. The vertical diameter (VD) was 5.14 mm on the left side and 4.82 mm on the right side. The distance of optic foramen to apex of petrous temporal bone was 21.84 mm on the Keywords left side and 21.90 mm on the right side. The mean, standard deviation, range, and ► optic foramen p value were measured by using SPSS software version 19.00. ► dry skull Conclusion In the present study we attempt to provide a comprehensive anatomical ► morphometry and morphometric data of optic foramen that may help ophthalmologists and ► dimensions neurosurgeons during surgery. -

Septation of the Sphenoid Sinus and Its Clinical Significance
1793 International Journal of Collaborative Research on Internal Medicine & Public Health Septation of the Sphenoid Sinus and its Clinical Significance Eldan Kapur 1* , Adnan Kapidžić 2, Amela Kulenović 1, Lana Sarajlić 2, Adis Šahinović 2, Maida Šahinović 3 1 Department of anatomy, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina 2 Clinic for otorhinolaryngology, Clinical centre University of Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina 3 Department of histology and embriology, Medical faculty, University of Sarajevo, Čekaluša 90, 71000 Sarajevo, Bosnia and Herzegovina * Corresponding Author: Eldan Kapur, MD, PhD Department of anatomy, Medical faculty, University of Sarajevo, Bosnia and Herzegovina Email: [email protected] Phone: 033 66 55 49; 033 22 64 78 (ext. 136) Abstract Introduction: Sphenoid sinus is located in the body of sphenoid, closed with a thin plate of bone tissue that separates it from the important structures such as the optic nerve, optic chiasm, cavernous sinus, pituitary gland, and internal carotid artery. It is divided by one or more vertical septa that are often asymmetric. Because of its location and the relationships with important neurovascular and glandular structures, sphenoid sinus represents a great diagnostic and therapeutic challenge. Aim: The aim of this study was to assess the septation of the sphenoid sinus and relationship between the number and position of septa and internal carotid artery in the adult BH population. Participants and Methods: A retrospective study of the CT analysis of the paranasal sinuses in 200 patients (104 male, 96 female) were performed using Siemens Somatom Art with the following parameters: 130 mAs: 120 kV, Slice: 3 mm. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

A Description of the Geological Context, Discrete Traits, and Linear Morphometrics of the Middle Pleistocene Hominin from Dali, Shaanxi Province, China
AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 150:141–157 (2013) A Description of the Geological Context, Discrete Traits, and Linear Morphometrics of the Middle Pleistocene Hominin from Dali, Shaanxi Province, China Xinzhi Wu1 and Sheela Athreya2* 1Laboratory for Human Evolution, Institute of Vertebrate Paleontology and Paleoanthropology, Chinese Academy of Sciences, Beijing 100044, China 2Department of Anthropology, Texas A&M University, College Station, TX 77843 KEY WORDS Homo heidelbergensis; Homo erectus; Asia ABSTRACT In 1978, a nearly complete hominin Afro/European Middle Pleistocene Homo and align it fossil cranium was recovered from loess deposits at the with Asian H. erectus.Atthesametime,itdisplaysa site of Dali in Shaanxi Province, northwestern China. more derived morphology of the supraorbital torus and It was subsequently briefly described in both English supratoral sulcus and a thinner tympanic plate than and Chinese publications. Here we present a compre- H. erectus, a relatively long upper (lambda-inion) occi- hensive univariate and nonmetric description of the pital plane with a clear separation of inion and opis- specimen and provide comparisons with key Middle thocranion, and an absolute and relative increase in Pleistocene Homo erectus and non-erectus hominins brain size, all of which align it with African and Euro- from Eurasia and Africa. In both respects we find pean Middle Pleistocene Homo. Finally, traits such as affinities with Chinese H. erectus as well as African the form of the frontal keel and the relatively short, and European Middle Pleistocene hominins typically broad midface align Dali specifically with other referred to as Homo heidelbergensis.Specifically,the Chinese specimens from the Middle Pleistocene Dali specimen possesses a low cranial height, relatively and Late Pleistocene, including H. -

Introduction to the Skeletal System and the Axial Skeleton 155
chapter Introduction to the 7 Skeletal System and the Axial Skeleton CHAPTER OVERVIEW OBJECTIVES 7.1 Introduction to the Skeletal System ……………… 153 1. Describe the gross anatomy and structure of a long 7.2 Bone Structure ………………………………………… 154 bone 7.3 Bone Histology ………………………………………… 155 2. Describe and compare the underlying histology of spongy and compact bone. 7.4 The Human Skeleton: Axial and Appendicular Divisions …………………………………………………… 156 3. List the five general shapes of bones. 7.5 Bone Classification and Markings ………………… 157 4. Describe and compare the different kinds of bone markings visible on the skeleton. 7.6 Axial Skeleton …………………………………………… 159 7.6a Cranium 5. Identify the components of the axial skeleton: cranial, 7.6b Facial facial, hyoid, vertebra, ribs and sternum. 7.6c Hyoid Bone 7.6d Vertebral Column 7.6e Thoracic Cage 7.1 Introduction to the Skeletal System The skeletal system serves to support the body’s soft tissues and to protect the body’s soft internal organs. Another important function that the bones have is to store materials such as calcium, phosphorus and lipids. Additionally, blood cells are synthesized in the red bone marrow to be released into the bloodstream. Bones serve as levers for the muscular system, working with them to produce movement and maintain posture. The human body contains 2 major kinds of bone tissue: compact and spongy. Compact bone (dense bone) is found on the outer surface of bones and serves as a place to absorb most of the stress on the bones. Spongy bone (cancellous tissue) is found on the inside of the compact bone layer. -

An Osteologic Study of Cranial Opening of Optic Canal in Gujarat Region
Original Article DOI: 10.7860/JCDR/2016/22110.8929 An Osteologic Study of Cranial Opening of Optic Canal in Section Gujarat Region Anatomy BINITA JIGNESHKUMAR PUROHIT1, PRAVEEN R SINGH2 ABSTRACT Similarly, morphologic features related with the canal were studied Introduction: Optic canal is a bony canal situated in between the by calculating frequency and proportions of various parameters. roots of lesser wings of sphenoid, lateral to body of sphenoid. Results: Optic canal was present in all 150 skulls studied bilaterally. It transmits optic nerve and ophthalmic artery, surrounded by The mean maximum dimension of the canal at cranial opening was meninges. Various authors have studied variations in skull foramina Keywords: ??????????????????????????????????5.03±0.72 mm on right side and 5.02±0.76 mm on left side. The and correlated clinically, as variants in the body structures have shape of the canal was ovoid at cranial opening in all the skulls been found to be associated with many inherited or acquired studied. Duplication of optic canal was present in one skull on left diseases. side. Recess was found in 105(35%) sides of total skulls observed. Aim: The present study aimed to examine morphologic and Fissure was found in 20(6.67%) sides and notch was observed in morphometric variations in cranial openings of optic canals. 30(10%) sides of total skulls. Materials and Methods: The study was undertaken in total 150 Conclusion: The optic canal showed variability in various dry adult human skulls. The variations in size, shape, presence or parameters. Knowledge regarding variations in size, shape and absence and duplication or multiplication if any, in optic canal were unusual features on cranial opening of optic canal can be helpful observed bilaterally. -

Anatomical Variations of Sphenoid Sinus: a Radiological Evaluation
ADDIS ABABA UNIVERSITY, COLLEGE OF HEALTH SCIENCES, SCHOOL OF MEDICINE, DEPARTMENT OF ANATOMY Anatomical Variations of Sphenoid Sinus: A Radiological Evaluation BY: Tizita Kinfe (BSc.) JUNE, 2019 Addis Ababa, Ethiopia Anatomical Variations of Sphenoid Sinus: A Radiological Evaluation Thesis submitted to Department of Anatomy, School of Medicine, College of Health Sciences, Addis Ababa University for the partial fulfillment of the requirements for the Degree of Masters of Science (MSc.) in Human Anatomy. By: Tizita Kinfe (BSc.) April, 2019 Addis Ababa, Ethiopia IDENTIFICATION Name of investigator: Tizita Kinfe (BSc.) Advisors: Principal Advisor: Abay Mulu (Ass. Prof. in Anatomy), Department of Anatomy, School of Medicine, College of Health Sciences, AAU Co advisors: 1. Dr Tequam Debebe (Ass. Prof. in Radiology, Consultant Neuroradiologist), Department of Radiology, School of Medicine, CHS, AAU. 2. Dr Seife Teferi (Aso. Prof. in Radiology, Radiation Physist), Department of Radiology, School of Medicine, CHS, AAU. Full title of project: Anatomic Variations of Sphenoid Sinus: A Radiological Evaluation Address of Investigator: AAU, College of Health Sciences, School of Medicine, Department of Anatomy Cell phone: +251-910603204 E-mail: [email protected] P.O. Box: 9086 Addis Ababa University School of Graduate Studies Declaration This is to certify that the thesis prepared by Tizita Kinfe, entitled, “Anatomic Variations of Sphenoid Sinus: A Radiological Evaluation” and submitted in partial fulfillment of the requirements for degree of Masters of Science in Anatomy complies with the regulation of the University and meets the accepted standards with respect to originality and quality. This thesis has not been presented for degree any other University, and that all sources of materials used for the thesis have been fully acknowledged. -

Topographical Anatomy and Morphometry of the Temporal Bone of the Macaque
Folia Morphol. Vol. 68, No. 1, pp. 13–22 Copyright © 2009 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Topographical anatomy and morphometry of the temporal bone of the macaque J. Wysocki 1Clinic of Otolaryngology and Rehabilitation, II Medical Faculty, Warsaw Medical University, Poland, Kajetany, Nadarzyn, Poland 2Laboratory of Clinical Anatomy of the Head and Neck, Institute of Physiology and Pathology of Hearing, Poland, Kajetany, Nadarzyn, Poland [Received 7 July 2008; Accepted 10 October 2008] Based on the dissections of 24 bones of 12 macaques (Macaca mulatta), a systematic anatomical description was made and measurements of the cho- sen size parameters of the temporal bone as well as the skull were taken. Although there is a small mastoid process, the general arrangement of the macaque’s temporal bone structures is very close to that which is observed in humans. The main differences are a different model of pneumatisation and the presence of subarcuate fossa, which possesses considerable dimensions. The main air space in the middle ear is the mesotympanum, but there are also additional air cells: the epitympanic recess containing the head of malleus and body of incus, the mastoid cavity, and several air spaces on the floor of the tympanic cavity. The vicinity of the carotid canal is also very well pneuma- tised and the walls of the canal are very thin. The semicircular canals are relatively small, very regular in shape, and characterized by almost the same dimensions. The bony walls of the labyrinth are relatively thin. -

Factors Influencing the Articular Eminence of the Temporomandibular Joint (Review)
EXPERIMENTAL AND THERAPEUTIC MEDICINE 22: 1084, 2021 Factors influencing the articular eminence of the temporomandibular joint (Review) MARIA JUSTINA ROXANA VÎRLAN1, DIANA LORETA PĂUN2, ELENA NICOLETA BORDEA3, ANGELO PELLEGRINI3, ARSENIE DAN SPÎNU4, ROXANA VICTORIA IVAȘCU5, VICTOR NIMIGEAN5 and VANDA ROXANA NIMIGEAN1 1Discipline of Oral Rehabilitation, Faculty of Dental Medicine; 2Discipline of Endocrinology, Faculty of Medicine; 3Department of Specific Disciplines, Faculty of Midwifery and Nursing;4 Discipline of Urology, ‘Dr Carol Davila’ Central Military Emergency University Hospital, Faculty of Medicine; 5Discipline of Anatomy, Faculty of Dental Medicine, ‘Carol Davila’ University of Medicine and Pharmacy, 020021 Bucharest, Romania Received April 28, 2021; Accepted May 28, 2021 DOI: 10.3892/etm.2021.10518 Abstract. The temporomandibular joint (TMJ), the most 4. Factors influencing the inclination of the articular eminence complex and evolved joint in humans, presents two articular 5. Biological sex surfaces: the condyle of the mandible and the articular eminence 6. Age (AE) of the temporal bone. AE is the anterior root of the zygo‑ 7. Edentulism matic process of the temporal bone and has an anterior and 8. Conclusions a posterior slope, the latter being also known as the articular surface. AE is utterly important in the biomechanics of the TMJ, as the mandibular condyle slides along the posterior slope 1. Introduction of the AE while the mandible moves. The aim of this review was to assess significant factors influencing the inclination of The temporomandibular joint (TMJ), the most complex and the AE, especially modifications caused by aging, biological evolved joint in humans, is defined by the paired joints that sex or edentulism. -
The Axial Skeleton Visual Worksheet
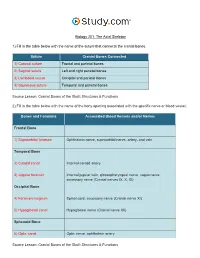
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -

The Temporomandibular Joint: Pneumatic Temporal Cells Open Into the Articular and Extradural Spaces C
CORE Metadata, citation and similar papers at core.ac.uk Provided by Via Medica Journals Folia Morphol. Vol. 78, No. 3, pp. 630–636 DOI: 10.5603/FM.a2018.0111 O R I G I N A L A R T I C L E Copyright © 2019 Via Medica ISSN 0015–5659 journals.viamedica.pl The temporomandibular joint: pneumatic temporal cells open into the articular and extradural spaces C. Bichir, M.C. Rusu, A.D. Vrapciu, N. Măru “Carol Davila” University of Medicine and Pharmacy of Bucharest, Romania [Received: 1 October 2018; Accepted: 22 November 2018] The pneumatisation of the articular tubercle (PAT) of the temporal squama is a rare condition that modifies the barrier between the temporomandibular joint (TMJ) space and the middle cranial fossa. During a routine examination of the cone-beam computed tomography (CBCT) files of patients who were scanned for dental medical purposes, we identified a case with multiple rare anatomic variations. First, the petrous apex was bilaterally pneumatised. Moreover, bilateral and multilocular PAT were observed, while on one side it was further found that the pneumatic cells were equally dehiscent towards the extradural space and the superior joint space. To the best of our knowledge, such dehiscence has not pre- viously been reported. The two temporomastoid pneumatisations were extended with occipital pneumatisations of the lateral masses and occipital condyles, the latter being an extremely rare evidence. The internal dehiscence of the mandibular canal in the right ramus of the mandible was also noted. Additionally, double mental foramen and impacted third molars were found on the left side.