Accident Prevention June 1998
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Qantas Counterfactual Paul Edwards 18 August 2003
The Qantas Counterfactual Public Session Paul Edwards 18 August 2003 Counterfactual • strategySecure and develop Australasian home base. • Competitive position is essential. • Natural extension of Qantas long term commitment to New Zealand 4 International 4 Domestic. Domestic New Zealand• Qantas is in the relatively early stages of domestic New Zealand expansion. • Qantas has maintained some form of presence in domestic New Zealand for 10 years. 4 Preferred selling arrangement with Ansett New Zealand (1990) 4 Franchise arrangement with Tasman Pacific (2000) 4 Qantas operations (May 2001) Commitment to Domestic New • Expansion plans slowed due to events outsideZealand Qantas control 4 Collapse of Ansett Australia in September 2001. • Implementation of the counterfactual is already in progress. 4 Jetconnect established in June 2001 4 Received AOC in October 2002 4 Five-aircraft operation by November 2002 4 Sixth aircraft arrived in May 2003 4 Wellington base established June 2003 Reasons for growing in Domestic New • Need to protectZealand and build network profit. • Home market. • Need to build frequency. • Current revenue share does not match capacity share (“share gap”). Plans for Domestic • New fareNew structure already Zealand implemented. • Continue with plans to expand the business. • Review of product and network. • Discuss further in confidential session. Plans for the • Introduction ofTasman more efficient aircraft 4Operate all Auckland and most Christchurch services with wide-bodied aircraft 4Operation of some 737s using Jetconnect. • Review fare structure. • Discuss above and other international routes further in confidential session. Airline Planning Group New Zealand Presence Analysis Overview of ‘City Presence’ What passengers value • Competitive fares. • Minimum travel time to destination. -

Wellington International Airport Limited Presentation to Commerce Commission Conference | 21 August 03 | Page 2
Presentation to Commerce Commission Conference | 21 August 2003 Presentation by John Sheridan Chief Executive, Wellington International Airport Limited Presentation to Commerce Commission Conference | 21 August 03 | page 2 Introduction Aviation experience 16 years in the aviation industry including 12 years in senior airline positions and over 4 years as the Chief Executive of Wellington International Airport The interest of WIAL in the application WIAL is directly affected by the outcome Objective To clearly demonstrate the critical importance of competition for both market growth and the continuing introduction of new product and services Presentation to Commerce Commission Conference | 21 August 03 | page 3 Domestic Market: 1987 - present Ansett New Zealand commenced operations in 1987 with some immediate outcomes being: Upgraded terminal facilities The introduction of aerobridges Improved service standards. A few examples: Catering on the aircraft, lounge facilities & valet parking Most importantly Ansett New Zealand meant competition and the availability of discount fares. Average fare dilution increased from 15% to 35%-40% on those sectors where Ansett New Zealand competed The stimulation of market growth Domestic passenger numbers through Wellington airport increased by 20% in the first two years after Ansett New Zealand started operations Presentation to Commerce Commission Conference | 21 August 03 | page 4 Domestic Market: 1987 - present In the period 1995 through to November 2002 there were few initiatives in the market, with the result that growth averaged 1.3% per year only over this period. This period included the Ansett pilots dispute in 1999, the receivership of Tasman Pacific in 2001, the start-up of Qantas Airways domestic services in New Zealand and the growth of Origin Pacific. -

Airlines Codes
Airlines codes Sorted by Airlines Sorted by Code Airline Code Airline Code Aces VX Deutsche Bahn AG 2A Action Airlines XQ Aerocondor Trans Aereos 2B Acvilla Air WZ Denim Air 2D ADA Air ZY Ireland Airways 2E Adria Airways JP Frontier Flying Service 2F Aea International Pte 7X Debonair Airways 2G AER Lingus Limited EI European Airlines 2H Aero Asia International E4 Air Burkina 2J Aero California JR Kitty Hawk Airlines Inc 2K Aero Continente N6 Karlog Air 2L Aero Costa Rica Acori ML Moldavian Airlines 2M Aero Lineas Sosa P4 Haiti Aviation 2N Aero Lloyd Flugreisen YP Air Philippines Corp 2P Aero Service 5R Millenium Air Corp 2Q Aero Services Executive W4 Island Express 2S Aero Zambia Z9 Canada Three Thousand 2T Aerocaribe QA Western Pacific Air 2U Aerocondor Trans Aereos 2B Amtrak 2V Aeroejecutivo SA de CV SX Pacific Midland Airlines 2W Aeroflot Russian SU Helenair Corporation Ltd 2Y Aeroleasing SA FP Changan Airlines 2Z Aeroline Gmbh 7E Mafira Air 3A Aerolineas Argentinas AR Avior 3B Aerolineas Dominicanas YU Corporate Express Airline 3C Aerolineas Internacional N2 Palair Macedonian Air 3D Aerolineas Paraguayas A8 Northwestern Air Lease 3E Aerolineas Santo Domingo EX Air Inuit Ltd 3H Aeromar Airlines VW Air Alliance 3J Aeromexico AM Tatonduk Flying Service 3K Aeromexpress QO Gulfstream International 3M Aeronautica de Cancun RE Air Urga 3N Aeroperlas WL Georgian Airlines 3P Aeroperu PL China Yunnan Airlines 3Q Aeropostal Alas VH Avia Air Nv 3R Aerorepublica P5 Shuswap Air 3S Aerosanta Airlines UJ Turan Air Airline Company 3T Aeroservicios -

11. Working with the Airlines in the Australasia-Pacific Region
11 Working with the airlines in the Australasia-Pacific region With my tenure at the new Unisys on shaky ground, I asked former colleagues if they knew of a job opportunity for someone with my skill set. I certainly wanted to stay in the Asia-Pacific area. New Zealand, as a relatively small country, did not present any immediate opportunities other than working with a computer consultancy or setting up on my own, and I was not keen on the latter. Richard Hawkins had left Unisys in Hong Kong and joined the Société Internationale de Télécommunications Aéronautiques (SITA). He had already spoken to SITA on my behalf and advised me to call Ms Irene Legay in SITA’s Hong Kong office. The SITA opportunity was attractive. I knew the organisation and had overseen its Sperry installations in Bangkok and Jakarta. I knew SITA to be technically aggressive. It used Sperry second-level communication processors, without mainframes, for its communications network, and I had recently liaised with SITA when the New Zealand Defence Department had contemplated a similar application. After the end of World War II, international telephone lines had been hard to obtain, so the airlines decided it would be to their advantage to pool resources. SITA was set up to control those resources and provide additional services. In the 1980s, as SITA approached its 40th anniversary, director general Claude Lalanne had instructed McKinsey & Company, as consultants, to investigate the strategies that would keep SITA viable for the next 40 years. McKinsey had recommended that SITA set up 223 ALSO INNOVatoRS a sales and marketing operation — a group of 32 people — to optimise its potential. -
Wellington's Links with the World
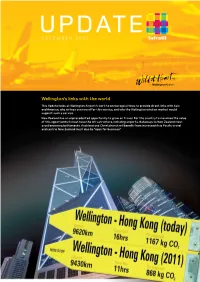
DECEMBER 2007 Wellington’s links with the world This Update looks at Wellington Airport’s work to encourage airlines to provide direct links with Asia and America, why airlines can now offer this service, and why the Wellington aviation market would support such a service. New Zealand has an unprecedented opportunity to grow air travel. For the country to maximise the value of this opportunity it must have the infrastructure, including airports. Gateways to New Zealand must avoid becoming bottlenecks. Auckland and Christchurch will benefit from increased Asia Pacific travel and central New Zealand must also be “open for business”. www.Infratil.com Air services matter Global Economic Activity (GEA) and world population within a 3.5 hour flying time PARIS CHICAGO 26% of world GEA 15% of world 32% of 25% of population HONG KONG world GEA world GEA 42% of world 7% of world population population WELLINGTON 1% of world GEA 0.4% of world population New Zealand is the furthest away place in the world. Draw a circle on a map to show 3.5 hours flying time from New Zealand and the circle captures 0.4% of the world’s population. The benefits and barriers of better connectivity are apparent from doing the same exercise centred on Hong Kong (42% of the world’s population and 32% of global economic activity), Paris (15% of the people, 26% of the economy) and Chicago (7% of the people and 25% of the world’s economy). A direct Wellington-Hong Kong air service would reduce travel time by at least three hours (six to seven if the service is via Sydney rather than Auckland). -
Air New Zealand / Qantas Authorisation Applications – Responses to Third Party Submissions
AIR NEW ZEALAND / QANTAS AUTHORISATION APPLICATIONS – RESPONSES TO THIRD PARTY SUBMISSIONS PART A – INTRODUCTION This document contains the formal response of Air New Zealand Limited (Air NZ) and Qantas Airways Limited (Qantas) (together the Applicants) to the submissions received by the New Zealand Commerce Commission (the Commerce Commission) and the Australian Competition and Consumer Commission (the ACCC) (together the Commissions) from third parties as of Friday 7 March 2003 (the Submissions). The Applicants’ response is divided into 3 Parts: · Part A – this introduction; · Part B – response to substantive issues; and · Part C – A paper prepared by NECG which is an integral part of this response. The substantive matters raised in the Submissions can be grouped broadly into 11 categories: (i) counterfactual; (ii) VBA entry/expansion; (iii) freight capacity; (iv) travel distribution; (v) tourism; (vi) undertakings/conditions; (vii) price and capacity changes; (viii) impact on Origin Pacific Airways Limited (Origin Pacific); AL030730105 250203 1117 (ix) impact on employment in Australia; (x) relevance of Australian air traffic rights; and (xi) frequent flyer points. The above characterisation of issues is structured to assist the Commissions in understanding the Applicants’ responses to issues raised in either or both jurisdictions. Clearly all issues are not relevant to both jurisdictions and this response should not be taken to represent the Applicants’ views on any jurisdictional issues. This response should also be read in conjunction with all additional papers filed by the Applicants. For example, the Applicants have recently filed a report prepared by Tourism Futures International dated 5 February 2003 (the TFI Report) and the Qantas Holidays Business Plan filed with the Commissions on 6 March 2003 (the QH Business Plan), which the Applicants believe address the Submissions on tourism. -
3 Digit 2 Digit Ticketing Code Code Name Code ------6M 40-MILE AIR VY A.C.E
06/07/2021 www.kovrik.com/sib/travel/airline-codes.txt 3 Digit 2 Digit Ticketing Code Code Name Code ------- ------- ------------------------------ --------- 6M 40-MILE AIR VY A.C.E. A.S. NORVING AARON AIRLINES PTY SM ABERDEEN AIRWAYS 731 GB ABX AIR (CARGO) 832 VX ACES 137 XQ ACTION AIRLINES 410 ZY ADALBANAIR 121 IN ADIRONDACK AIRLINES JP ADRIA AIRWAYS 165 REA RE AER ARANN 684 EIN EI AER LINGUS 053 AEREOS SERVICIOS DE TRANSPORTE 278 DU AERIAL TRANSIT COMPANY(CARGO) 892 JR AERO CALIFORNIA 078 DF AERO COACH AVIATION INT 868 2G AERO DYNAMICS (CARGO) AERO EJECUTIVOS 681 YP AERO LLOYD 633 AERO SERVICIOS 243 AERO TRANSPORTES PANAMENOS 155 QA AEROCARIBE 723 AEROCHAGO AIRLINES 198 3Q AEROCHASQUI 298 AEROCOZUMEL 686 AFL SU AEROFLOT 555 FP AEROLEASING S.A. ARG AR AEROLINEAS ARGENTINAS 044 VG AEROLINEAS EL SALVADOR (CARGO) 680 AEROLINEAS URUGUAYAS 966 BQ AEROMAR (CARGO) 926 AM AEROMEXICO 139 AEROMONTERREY 722 XX AERONAVES DEL PERU (CARGO) 624 RL AERONICA 127 PO AEROPELICAN AIR SERVICES WL AEROPERLAS PL AEROPERU 210 6P AEROPUMA, S.A. (CARGO) AW AEROQUETZAL 291 XU AEROVIAS (CARGO) 316 AEROVIAS COLOMBIANAS (CARGO) 158 AFFRETAIR (PRIVATE) (CARGO) 292 AFRICAN INTERNATIONAL AIRWAYS 648 ZI AIGLE AZUR AMM DP AIR 2000 RK AIR AFRIQUE 092 DAH AH AIR ALGERIE 124 3J AIR ALLIANCE 188 4L AIR ALMA 248 AIR ALPHA AIR AQUITAINE FQ AIR ARUBA 276 9A AIR ATLANTIC LTD. AAG ES AIR ATLANTIQUE OU AIR ATONABEE/CITY EXPRESS 253 AX AIR AURORA (CARGO) 386 ZX AIR B.C. 742 KF AIR BOTNIA BP AIR BOTSWANA 636 AIR BRASIL 853 AIR BRIDGE CARRIERS (CARGO) 912 VH AIR BURKINA 226 PB AIR BURUNDI 919 TY AIR CALEDONIE 190 www.kovrik.com/sib/travel/airline-codes.txt 1/15 06/07/2021 www.kovrik.com/sib/travel/airline-codes.txt SB AIR CALEDONIE INTERNATIONAL 063 ACA AC AIR CANADA 014 XC AIR CARIBBEAN 918 SF AIR CHARTER AIR CHARTER (CHARTER) AIR CHARTER SYSTEMS 272 CCA CA AIR CHINA 999 CE AIR CITY S.A. -

Qantas and Its Marginal Abatement Cost Curve in the Context of Late Capitalism and Climate Change
University of Wollongong Research Online University of Wollongong Thesis Collection 1954-2016 University of Wollongong Thesis Collections 2014 Qantas and its marginal abatement cost curve in the context of late capitalism and climate change Juergen Seufert University of Wollongong Follow this and additional works at: https://ro.uow.edu.au/theses University of Wollongong Copyright Warning You may print or download ONE copy of this document for the purpose of your own research or study. The University does not authorise you to copy, communicate or otherwise make available electronically to any other person any copyright material contained on this site. You are reminded of the following: This work is copyright. Apart from any use permitted under the Copyright Act 1968, no part of this work may be reproduced by any process, nor may any other exclusive right be exercised, without the permission of the author. Copyright owners are entitled to take legal action against persons who infringe their copyright. A reproduction of material that is protected by copyright may be a copyright infringement. A court may impose penalties and award damages in relation to offences and infringements relating to copyright material. Higher penalties may apply, and higher damages may be awarded, for offences and infringements involving the conversion of material into digital or electronic form. Unless otherwise indicated, the views expressed in this thesis are those of the author and do not necessarily represent the views of the University of Wollongong. Recommended Citation Seufert, Juergen, Qantas and its marginal abatement cost curve in the context of late capitalism and climate change, Doctor of Philosophy thesis, School of Accounting, Economics and Finance, University of Wollongong, 2014. -

Commerce Commission Final Determination
ISSN NO. 0114-2720 J5633 PUBLIC VERSION Commerce Commission Final Determination Determinations pursuant to the Commerce Act 1986 in the matter of an application for authorisation of a business acquisition and in the matter of an application for authorisation of certain restrictive business practices and involving: AIR NEW ZEALAND LIMITED and QANTAS AIRWAYS LIMITED The Commission: PR Rebstock PJ Taylor DF Curtin D Bates QC Summary of Applications: The subscription by Qantas Airways Limited of up to 22.5% of the voting equity in Air New Zealand Limited pursuant to a Subscription Agreement between Air New Zealand Limited and Qantas Airways Limited (the proposed Acquisition); and The implementation by Air New Zealand Limited and Qantas Airways Limited of the terms of a Strategic Alliance arrangement which creates a Joint Airline Operation network (the proposed Arrangement) Final Determinations: The Commission determines to decline authorisation for the proposed Acquisition pursuant to s 67(3)(c) of the Act. The Commission determines to decline authorisation for the proposed Arrangement pursuant to s 61(6) of the Act. Date: 23 October 2003 CONFIDENTIAL MATERIAL IN THIS REPORT IS CONTAINED IN SQUARE BRACKETS i EXECUTIVE SUMMARY1 Proposed Alliance Between Air NZ and Qantas 1. On 9 December 2002 the Commerce Commission (the Commission) received two interdependent applications for authorisation from Air New Zealand Ltd (Air NZ) and Qantas Airways Ltd (Qantas). 2. The first application by Qantas, made under section 67(1) of the Commerce Act, relates to a proposed “share purchase agreement” whereby Qantas would acquire 22.5% of the voting equity in Air NZ. -

The History of the Australian Aerospace Industry
School of Mechanical Engineering MECH ENG 3016 Aeronautical Engineering 1 The History of the Australian Aerospace Industry Authors: Jarryd Pfeiffer 1132307 Kelly Balnaves 1132985 Bradley Darlington 1132806 Michael Cannizzo 1131304 Christian Rogers 1130940 Alex Horstmann 1131838 Submitted 3 rd October 2007 Lecturer: Dr. Maziar Arjomandi 1 ABSTRACT The Australian Aerospace industry began with the work of Lawrence Hargrave in the late 19 th century, which preceded and most likely influenced the first aeroplane ever built. Throughout the early 20 th century Australian aviators such as Bert Hinkler and Sir Charles Kingsford Smith made history by completing record-breaking flights all over the world. The Royal Australian Air Force and later the RAAF played an important role in both World Wars, aiding allied troops in locations as diverse as Europe, the Middle East and China. Australia’s size and scattered population made it important to establish an aviation industry as early as possible. Commercial aviation began in 1920 when Qantas was founded, later on; Australia became home to the world’s first flying doctor service. To this day, both Qantas and the Royal Flying Doctors Service are still operating. Throughout the 1950’s and 1960’s, the outback town of Woomera in South Australia became an important testing ground for the Australian and British military. Later on it was used as a base to launch a number of rockets and satellites. More recently, the Woomera range has played host to the University of Queensland’s HyShot Hypersonics program and is slated to become the launch site of the Kistler K1 reusable launch vehicle. -
The Failure of Aviation Safety in New Zealand
Journal of Air Law and Commerce Volume 68 | Issue 2 Article 6 2003 The aiF lure of Aviation Safety in New Zealand: An Examination of New Zealand's Implementation of Its International Obligations under Annex 13 of the Chicago Convention on International Civil Aviation Samantha Sharif Follow this and additional works at: https://scholar.smu.edu/jalc Recommended Citation Samantha Sharif, The Failure of Aviation Safety in New Zealand: An Examination of New Zealand's Implementation of Its International Obligations under Annex 13 of the Chicago Convention on International Civil Aviation, 68 J. Air L. & Com. 339 (2003) https://scholar.smu.edu/jalc/vol68/iss2/6 This Article is brought to you for free and open access by the Law Journals at SMU Scholar. It has been accepted for inclusion in Journal of Air Law and Commerce by an authorized administrator of SMU Scholar. For more information, please visit http://digitalrepository.smu.edu. THE FAILURE OF AVIATION SAFETY IN NEW ZEALAND: AN EXAMINATION OF NEW ZEALAND'S IMPLEMENTATION OF ITS INTERNATIONAL OBLIGATIONS UNDER ANNEX 13 OF THE CHICAGO CONVENTION ON INTERNATIONAL CIVIL AVIATION SAMANTHA SHARIF* "It could have happened to any of us." r[HESE SOBERING words were spoken by Captain Gordon .LVette after New Zealand's worst air disaster, the Mount Ere- bus tragedy, where, almost 20 years ago to the day, an Air New Zealand aircraft flew straight into the side of Mount Erebus in Antarctica, killing all 257 passengers on board. I. AN INTRODUCTION TO THE DEBATE This paper examines the issue of aviation safety in New Zea- land. -

Kiwi Team's Ultimate Quest for Speed Ends in Dead Heat for Black Beauty
ISSUE: airporttimes 71 KEEPING THE AUCKLAND AIRPORT COMMUNITY INFORMED FEB 08 Photosport image Photosport image BLACK BEAUTY TAKES ON THE 777. AFTER THE RACE JONNY SIGNED AUTOGRAPHS, TALKED TO ENTHUSIASTS AND SHOWED OFF BLACK BEAUTY AT THE INTERNATIONAL TERMINAL CAR PARK. Kiwi team’s ultimate quest for speed ends in dead heat for Black Beauty and Boeing 777 For the first time in history, Auckland Airport adjusted its flight schedule – for a unique event when a Grand Prix race car and a passenger jet competed in what was dubbed “the ultimate quest for speed”. The bold publicity stunt on Tuesday 8 January, was held to promote the we’re appreciably busier and the world is a more security-conscious 21-nation A1GP World Cup of Motorsport event in Taupo, the fifth of the place, but we selected a non-peak time and worked closely with 10 rounds that make up the series. airport stakeholders to make it all work smoothly.” In a world first, New Zealand A1GP motor racing driver Jonny Reid Jonny said it was like no other race in which he had driven and a and his Black Beauty vehicle took on an Air New Zealand 777 at a fully moment he’ll remember forever. “It was mind-blowing and the perfect operational commercial airport. The vehicles did not disappoint with adrenalin rush before the race in Taupo. I’ve never been on such a wide Jonny getting Black Beauty to almost 300 kilometres an hour as he track before and it was fantastic looking across and seeing the Boeing raced past the Boeing as it left the tarmac at just under 270 kilometres 777 alongside me.