Helicobacter Pylori Virulence Factors Exploiting Gastric Colonization and Its Pathogenicity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adaptive Clinical Trials: an Introduction
Adaptive clinical trials: an introduction What are the advantages and disadvantages of adaptive clinical trial designs? How and why were Introduction adaptive clinical Adaptive clinical trial design is trials developed? becoming a hot topic in healthcare research, with some researchers In 2004, the FDA published a report arguing that adaptive trials have the on the problems faced by the potential to get new drugs to market scientific community in developing quicker. In this article, we explain new medical treatments.2 The what adaptive trials are and why they report highlighted that the pace of were developed, and we explore both innovation in biomedical science is the advantages of adaptive designs outstripping the rate of advances and the concerns being raised by in the available technologies and some in the healthcare community. tools for evaluating new treatments. Outdated tools are being used to assess new treatments and there What are adaptive is a critical need to improve the effectiveness and efficiency of clinical trials? clinical trials.2 The current process for developing Adaptive clinical trials enable new treatments is expensive, takes researchers to change an aspect a long time and in some cases, the of a trial design at an interim development process has to be assessment, while controlling stopped after significant amounts the rate of type 1 errors.1 Interim of time and resources have been assessments can help to determine invested.2 In 2006, the FDA published whether a trial design is the most a “Critical Path Opportunities -

ﺑﺴﻢ اﷲ اﻟﺮﺣﻤﻦ اﻟﺮﺣﻴﻢ Molecular Characterization Of
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by KhartoumSpace ﺑﺴﻢ اﷲ اﻟﺮﺣﻤﻦ اﻟﺮﺣﻴﻢ Molecular Characterization of Pasteurella multocida Vaccine Strains By: Hajir Badawi Mohammed Ahmed B.V.M Khartoum University (2006) Supervisor: Dr. Awad A. Ibrahim A dissertation submitted to the University of Khartoum in partial fulfillment of the requirements for the degree of M. Sc. in Microbiology Department of Microbiology, Faculty of Veterinary Medicine, University of Khartoum June, 2010 Dedication To my mother Father Brother, sister and friends With great love Acknowledgments First and foremost, I would like to thank my Merciful Allah, the most beneficent for giving me strength and health to accomplish this work. Then I would like to deeply thank my supervisor Dr. Awad A. Ibrahim for his advice, continuous encouragement and patience throughout the period of this work. My gratitude is also extended to prof. Mawia M. Mukhtar and for Dr. Manal Gamal El-dein, Institute of Endemic Disease. My thanks extend to members of Department of Microbiology Faculty of Veterinary Medicine for unlimited assistant and for staff of Central Laboratory Soba. I am grateful to my family for their continuous support and standing beside me all times. My thanks also extended to all whom I didn’t mention by name and to the forbearance of my friends, and colleagues who helped me. Finally I am indebted to all those who helped me so much to make this work a success. Abstract The present study was carried out to study the national haemorrhagic septicaemia vaccine strains at their molecular level. -

Potential of Bacterial Cellulose Chemisorbed with Anti-Metabolites, 3-Bromopyruvate Or Sertraline, to Fight Against Helicobacter Pylori Lawn Biofilm
International Journal of Molecular Sciences Article Potential of Bacterial Cellulose Chemisorbed with Anti-Metabolites, 3-Bromopyruvate or Sertraline, to Fight against Helicobacter pylori Lawn Biofilm Paweł Krzy˙zek 1,* , Gra˙zynaGo´sciniak 1 , Karol Fijałkowski 2 , Paweł Migdał 3 , Mariusz Dziadas 4 , Artur Owczarek 5 , Joanna Czajkowska 6, Olga Aniołek 7 and Adam Junka 8 1 Department of Microbiology, Faculty of Medicine, Wroclaw Medical University, 50-368 Wroclaw, Poland; [email protected] 2 Department of Immunology, Microbiology and Physiological Chemistry, Faculty of Biotechnology and Animal Husbandry, West Pomeranian University of Technology in Szczecin, 70-311 Szczecin, Poland; karol.fi[email protected] 3 Department of Environment, Hygiene and Animal Welfare, Wroclaw University of Environmental and Life Sciences, 51-630 Wroclaw, Poland; [email protected] 4 Faculty of Chemistry, University of Wroclaw, 50-353 Wroclaw, Poland; [email protected] 5 Department of Drug Form Technology, Wroclaw Medical University, 50-556 Wroclaw, Poland; [email protected] 6 Laboratory of Microbiology, Polish Center for Technology Development PORT, 54-066 Wroclaw, Poland; [email protected] 7 Faculty of Medicine, Lazarski University, 02-662 Warsaw, Poland; [email protected] 8 Department of Pharmaceutical Microbiology and Parasitology, Wroclaw Medical University, 50-556 Wroclaw, Poland; [email protected] * Correspondence: [email protected] Received: 23 November 2020; Accepted: 11 December 2020; Published: 14 December 2020 Abstract: Helicobacter pylori is a bacterium known mainly of its ability to cause persistent inflammations of the human stomach, resulting in peptic ulcer diseases and gastric cancers. Continuous exposure of this bacterium to antibiotics has resulted in high detection of multidrug-resistant strains and difficulties in obtaining a therapeutic effect. -

Quasi-Experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: a Systematic Review
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Infect Control Manuscript Author Hosp Epidemiol Manuscript Author . Author manuscript; available in PMC 2019 November 12. Published in final edited form as: Infect Control Hosp Epidemiol. 2018 February ; 39(2): 170–176. doi:10.1017/ice.2017.296. Quasi-experimental Studies in the Fields of Infection Control and Antibiotic Resistance, Ten Years Later: A Systematic Review Rotana Alsaggaf, MS, Lyndsay M. O’Hara, PhD, MPH, Kristen A. Stafford, PhD, MPH, Surbhi Leekha, MBBS, MPH, Anthony D. Harris, MD, MPH, CDC Prevention Epicenters Program Department of Epidemiology and Public Health, University of Maryland School of Medicine, Baltimore, Maryland. Abstract OBJECTIVE.—A systematic review of quasi-experimental studies in the field of infectious diseases was published in 2005. The aim of this study was to assess improvements in the design and reporting of quasi-experiments 10 years after the initial review. We also aimed to report the statistical methods used to analyze quasi-experimental data. DESIGN.—Systematic review of articles published from January 1, 2013, to December 31, 2014, in 4 major infectious disease journals. METHODS.—Quasi-experimental studies focused on infection control and antibiotic resistance were identified and classified based on 4 criteria: (1) type of quasi-experimental design used, (2) justification of the use of the design, (3) use of correct nomenclature to describe the design, and (4) statistical methods used. RESULTS.—Of 2,600 articles, 173 (7%) featured a quasi-experimental design, compared to 73 of 2,320 articles (3%) in the previous review (P<.01). Moreover, 21 articles (12%) utilized a study design with a control group; 6 (3.5%) justified the use of a quasi-experimental design; and 68 (39%) identified their design using the correct nomenclature. -
Identification of Pasteurella Species and Morphologically Similar Organisms
UK Standards for Microbiology Investigations Identification of Pasteurella species and Morphologically Similar Organisms Issued by the Standards Unit, Microbiology Services, PHE Bacteriology – Identification | ID 13 | Issue no: 3 | Issue date: 04.02.15 | Page: 1 of 28 © Crown copyright 2015 Identification of Pasteurella species and Morphologically Similar Organisms Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website https://www.gov.uk/uk- standards-for-microbiology-investigations-smi-quality-and-consistency-in-clinical- laboratories. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see https://www.gov.uk/government/groups/standards-for-microbiology-investigations- steering-committee). The contributions of many individuals in clinical, specialist and reference laboratories who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editing the medical content. For further information please contact us at: Standards Unit Microbiology Services Public Health England 61 Colindale Avenue London NW9 5EQ E-mail: [email protected] Website: https://www.gov.uk/uk-standards-for-microbiology-investigations-smi-quality- and-consistency-in-clinical-laboratories UK Standards for Microbiology Investigations are produced in association with: Logos correct at time of publishing. Bacteriology – Identification | ID 13 | Issue no: 3 | Issue date: 04.02.15 | Page: 2 of 28 UK Standards for Microbiology Investigations | Issued by the Standards Unit, Public Health England Identification of Pasteurella species and Morphologically Similar Organisms Contents ACKNOWLEDGMENTS ......................................................................................................... -

Chapitre IV: Bacilles Gram Négatifs Aéro- Anaérobie Facultatifs ______Les Entérobactéries, Cours De Microbiologie Systématique Dr
Chapitre IV: Bacilles Gram négatifs aéro- anaérobie facultatifs __________________________________________Les entérobactéries, Cours de Microbiologie Systématique Dr. BOUSSENA 1. Enterobacteriaceae 1.1. Définition Les entérobactéries sont une famille très hétérogène pour ce qui est de leur pathogénie et de leur écologie. Les espèces qui composent cette famille sont en effet soit parasites (Shigella, Yersinia pestis), soit commensales (Escherichia coli, Proteus mirabilis, Klebsiella sp), soit encore saprophytes (Serratia sp, Enterobacter sp). 1.2. Habitat et pouvoir pathogène Le domaine des entérobactéries commensales ne se limite pas à l’intestin : on les trouve aussi dans la cavité buccale, au niveau des voies aériennes supérieures et sur les organes génitaux. Les entérobactéries sont présentes dans le monde entier et elles ont un habitat très large : eau douce, eau de mer (Alterococcus agarolyticus), sol, végétaux, animaux et elles peuvent contaminer des denrées alimentaires. Certaines espèces sont responsables de diarrhée et/ou d'infections opportunistes (infections urinaires, infections respiratoires, surinfections des plaies, septicémies, méningites...). 1.3. Répartition en genres Au sein des entérobactéries, on distingue de nombreux genres (Shigella, Escherichia, Enterobacter, Serratia, etc…) (tableau 3-1 et 3-2). La distinction entre les genres se fait par l'étude des caractères biochimiques dont les plus importants sont : fermentation du lactose, production d'indole, production d'uréase, production d'acetoïne (réaction dite VP+), utilisation du citrate, désamination du tryptophane. 1.4. Caractérisation des espèces Au sein de chaque genre, on individualise des espèces, par l'étude des caractères biochimiques ou antigéniques. Les entérobactéries possèdent toutes des antigènes de paroi (« somatiques ») ou antigènes O. Les entérobactéries mobiles possèdent en plus des antigènes de flagelle (« flagellaires ») ou antigènes H. -

Gastroenteritis and Transmission of Helicobacter Pylori Infection in Households1 Sharon Perry,* Maria De La Luz Sanchez,* Shufang Yang,* Thomas D
Gastroenteritis and Transmission of Helicobacter pylori Infection in Households1 Sharon Perry,* Maria de la Luz Sanchez,* Shufang Yang,* Thomas D. Haggerty,* Philip Hurst,† Guillermo Perez-Perez,‡ and Julie Parsonnet* The mode of transmission of Helicobacter pylori gastrointestinal infections, infection is associated with infection is poorly characterized. In northern California, conditions of crowding and poor hygiene (7,8) and with 2,752 household members were tested for H. pylori infec- intrafamilial clustering (9–12). The organism has been tion in serum or stool at a baseline visit and 3 months later. recovered most reliably from vomitus and from stools dur- Among 1,752 person considered uninfected at baseline, ing rapid gastrointestinal transit (13). These findings raise 30 new infections (7 definite, 7 probable, and 16 possible) occurred, for an annual incidence of 7% overall and 21% the hypothesis that gastroenteritis episodes provide the in children <2 years of age. Exposure to an infected opportunity for H. pylori transmission. household member with gastroenteritis was associated Household transmission of gastroenteritis is common in with a 4.8-fold (95% confidence interval [CI] 1.4–17.1) the United States, particularly in homes with small chil- increased risk for definite or probable new infection, with dren (14). If H. pylori is transmitted person to person, one vomiting a greater risk factor (adjusted odds ratio [AOR] might expect rates of new infection to be elevated after 6.3, CI 1.6–24.5) than diarrhea only (AOR 3.0, p = 0.65). exposure to persons with H. pylori–infected cases of gas- Of probable or definite new infections, 75% were attributa- troenteritis. -

A Guide to Systematic Review and Meta-Analysis of Prediction Model Performance
RESEARCH METHODS AND REPORTING A guide to systematic review and meta-analysis of prediction model performance Thomas P A Debray,1,2 Johanna A A G Damen,1,2 Kym I E Snell,3 Joie Ensor,3 Lotty Hooft,1,2 Johannes B Reitsma,1,2 Richard D Riley,3 Karel G M Moons1,2 1Cochrane Netherlands, Validation of prediction models is diagnostic test accuracy studies. Compared to therapeu- University Medical Center tic intervention and diagnostic test accuracy studies, Utrecht, PO Box 85500 Str highly recommended and increasingly there is limited guidance on the conduct of systematic 6.131, 3508 GA Utrecht, Netherlands common in the literature. A systematic reviews and meta-analysis of primary prognosis studies. 2Julius Center for Health review of validation studies is therefore A common aim of primary prognostic studies con- Sciences and Primary Care, cerns the development of so-called prognostic predic- University Medical Center helpful, with meta-analysis needed to tion models or indices. These models estimate the Utrecht, PO Box 85500 Str 6.131, 3508 GA Utrecht, summarise the predictive performance individualised probability or risk that a certain condi- Netherlands of the model being validated across tion will occur in the future by combining information 3Research Institute for Primary from multiple prognostic factors from an individual. Care and Health Sciences, Keele different settings and populations. This Unfortunately, there is often conflicting evidence about University, Staffordshire, UK article provides guidance for the predictive performance of developed prognostic Correspondence to: T P A Debray [email protected] researchers systematically reviewing prediction models. For this reason, there is a growing Additional material is published demand for evidence synthesis of (external validation) online only. -
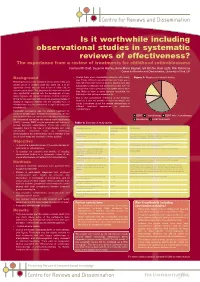
Is It Worthwhile Including Observational Studies in Systematic Reviews of Effectiveness?
CRD_mcdaid05_Poster.qxd 13/6/05 5:12 pm Page 1 Is it worthwhile including observational studies in systematic reviews of effectiveness? The experience from a review of treatments for childhood retinoblastoma Catriona Mc Daid, Suzanne Hartley, Anne-Marie Bagnall, Gill Ritchie, Kate Light, Rob Riemsma Centre for Reviews and Dissemination, University of York, UK Background • Overall there were considerable problems with quality Figure 1: Mapping of included studies (see Table). Without randomised allocation there was a Retinoblastoma is a rare malignant tumour of the retina and high risk of selection bias in all studies. Studies were also usually occurs in children under two years old. It is an susceptible to detection and performance bias, with the aggressive tumour that can lead to loss of vision and, in retrospective studies particularly susceptible as they were extreme cases, death. The prognoses for vision and survival less likely to have a study protocol specifying the have significantly improved with the development of more intervention and outcome assessments. timely diagnosis and improved treatment methods. Important • Due to the considerable limitations of the evidence clinical factors associated with prognosis are age and stage of identified, it was not possible to make meaningful and disease at diagnosis. Patients with the hereditary form of robust conclusions about the relative effectiveness of retinoblastoma may be predisposed to significant long-term different treatment approaches for childhood complications. retinoblastoma. Historically, enucleation was the standard treatment for unilateral retinoblastoma. In bilateral retinoblastoma, the eye ■ ■ ■ with the most advanced tumour was commonly removed and EBRT Chemotherapy EBRT with Chemotherapy the contralateral eye treated with external beam radiotherapy ■ Enucleation ■ Local Treatments (EBRT). -

How to Get Started with a Systematic Review in Epidemiology: an Introductory Guide for Early Career Researchers
Denison et al. Archives of Public Health 2013, 71:21 http://www.archpublichealth.com/content/71/1/21 ARCHIVES OF PUBLIC HEALTH METHODOLOGY Open Access How to get started with a systematic review in epidemiology: an introductory guide for early career researchers Hayley J Denison1*†, Richard M Dodds1,2†, Georgia Ntani1†, Rachel Cooper3†, Cyrus Cooper1†, Avan Aihie Sayer1,2† and Janis Baird1† Abstract Background: Systematic review is a powerful research tool which aims to identify and synthesize all evidence relevant to a research question. The approach taken is much like that used in a scientific experiment, with high priority given to the transparency and reproducibility of the methods used and to handling all evidence in a consistent manner. Early career researchers may find themselves in a position where they decide to undertake a systematic review, for example it may form part or all of a PhD thesis. Those with no prior experience of systematic review may need considerable support and direction getting started with such a project. Here we set out in simple terms how to get started with a systematic review. Discussion: Advice is given on matters such as developing a review protocol, searching using databases and other methods, data extraction, risk of bias assessment and data synthesis including meta-analysis. Signposts to further information and useful resources are also given. Conclusion: A well-conducted systematic review benefits the scientific field by providing a summary of existing evidence and highlighting unanswered questions. For the individual, undertaking a systematic review is also a great opportunity to improve skills in critical appraisal and in synthesising evidence. -

Identification of Human Enteric Pathogens in Gull Feces at Southwestern Lake Michigan Bathing Beaches
1006 Identification of human enteric pathogens in gull feces at Southwestern Lake Michigan bathing beaches Julie Kinzelman, Sandra L. McLellan, Ashley Amick, Justine Preedit, Caitlin O. Scopel, Ola Olapade, Steve Gradus, Ajaib Singh, and Gerald Sedmak Abstract: Ring-billed (Larus delawarensis Ord, 1815) and herring (Larus argentatus Pontoppidan, 1763) gulls are predom- inant species of shorebirds in coastal areas. Gulls contribute to the fecal indicator burden in beach sands, which, once transported to bathing waters, may result in water quality failures. The importance of these contamination sources must not be overlooked when considering the impact of poor bathing water quality on human health. This study examined the occurrence of human enteric pathogens in gull populations at Racine, Wisconsin. For 12 weeks in 2004 and 2005, and 7 weeks in 2006, 724 gull fecal samples were examined for pathogen occurrence on traditional selective media (BBL CHROMagar-Salmonella, Remel Campy-BAP, 7% horse blood agar) or through the use of novel isolation techniques (Campylobacter, EC FP5-funded CAMPYCHECK Project), and confirmed using polymerase chain reaction (PCR) for pathogens commonly harbored in gulls. An additional 226 gull fecal samples, collected in the same 12-week period in 2004, from a beach in Milwaukee, Wisconsin, were evaluated with standard microbiological methods and PCR. Five iso- lates of Salmonella (0.7%), 162 (22.7%) isolates of Campylobacter, 3 isolates of Aeromonas hydrophila group 2 (0.4%), and 28 isolates of Plesiomonas shigelloides (3.9%) were noted from the Racine beach. No occurrences of Salmonella and 3 isolates of Campylobacter (0.4%) were found at the Milwaukee beach. -

Use of the Diagnostic Bacteriology Laboratory: a Practical Review for the Clinician
148 Postgrad Med J 2001;77:148–156 REVIEWS Postgrad Med J: first published as 10.1136/pmj.77.905.148 on 1 March 2001. Downloaded from Use of the diagnostic bacteriology laboratory: a practical review for the clinician W J Steinbach, A K Shetty Lucile Salter Packard Children’s Hospital at EVective utilisation and understanding of the Stanford, Stanford Box 1: Gram stain technique University School of clinical bacteriology laboratory can greatly aid Medicine, 725 Welch in the diagnosis of infectious diseases. Al- (1) Air dry specimen and fix with Road, Palo Alto, though described more than a century ago, the methanol or heat. California, USA 94304, Gram stain remains the most frequently used (2) Add crystal violet stain. USA rapid diagnostic test, and in conjunction with W J Steinbach various biochemical tests is the cornerstone of (3) Rinse with water to wash unbound A K Shetty the clinical laboratory. First described by Dan- dye, add mordant (for example, iodine: 12 potassium iodide). Correspondence to: ish pathologist Christian Gram in 1884 and Dr Steinbach later slightly modified, the Gram stain easily (4) After waiting 30–60 seconds, rinse with [email protected] divides bacteria into two groups, Gram positive water. Submitted 27 March 2000 and Gram negative, on the basis of their cell (5) Add decolorising solvent (ethanol or Accepted 5 June 2000 wall and cell membrane permeability to acetone) to remove unbound dye. Growth on artificial medium Obligate intracellular (6) Counterstain with safranin. Chlamydia Legionella Gram positive bacteria stain blue Coxiella Ehrlichia Rickettsia (retained crystal violet).