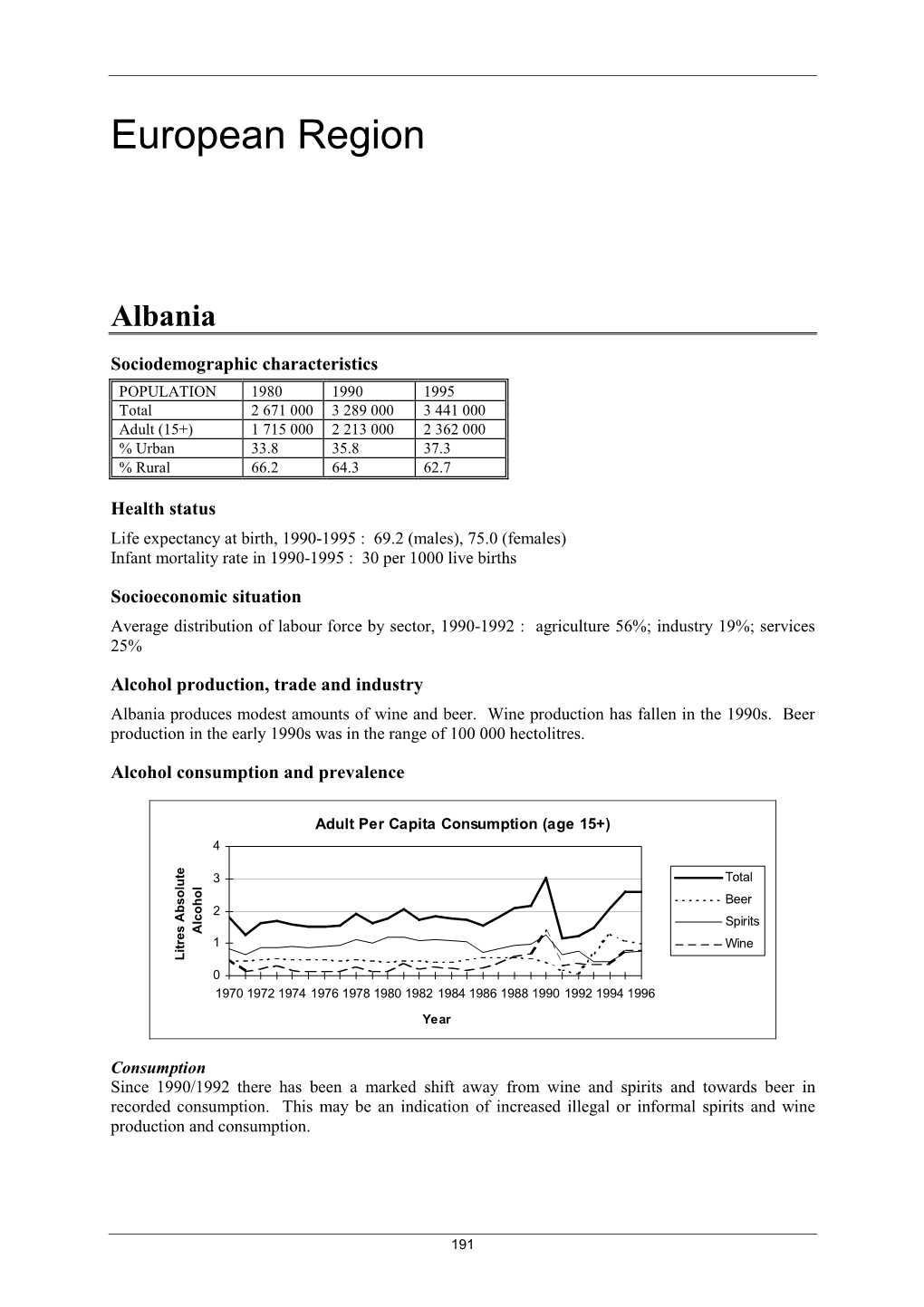
European Region
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Deity's Beer List.Xls
Page 1 The Deity's Beer List.xls 1 #9 Not Quite Pale Ale Magic Hat Brewing Co Burlington, VT 2 1837 Unibroue Chambly,QC 7% 3 10th Anniversary Ale Granville Island Brewing Co. Vancouver,BC 5.5% 4 1664 de Kronenbourg Kronenbourg Brasseries Stasbourg,France 6% 5 16th Avenue Pilsner Big River Grille & Brewing Works Nashville, TN 6 1889 Lager Walkerville Brewing Co Windsor 5% 7 1892 Traditional Ale Quidi Vidi Brewing St. John,NF 5% 8 3 Monts St.Syvestre Cappel,France 8% 9 3 Peat Wheat Beer Hops Brewery Scottsdale, AZ 10 32 Inning Ale Uno Pizzeria Chicago 11 3C Extreme Double IPA Nodding Head Brewery Philadelphia, Pa. 12 46'er IPA Lake Placid Pub & Brewery Plattsburg , NY 13 55 Lager Beer Northern Breweries Ltd Sault Ste.Marie,ON 5% 14 60 Minute IPA Dogfishhead Brewing Lewes, DE 15 700 Level Beer Nodding Head Brewery Philadelphia, Pa. 16 8.6 Speciaal Bier BierBrouwerij Lieshout Statiegeld, Holland 8.6% 17 80 Shilling Ale Caledonian Brewing Edinburgh, Scotland 18 90 Minute IPA Dogfishhead Brewing Lewes, DE 19 Abbaye de Bonne-Esperance Brasserie Lefebvre SA Quenast,Belgium 8.3% 20 Abbaye de Leffe S.A. Interbrew Brussels, Belgium 6.5% 21 Abbaye de Leffe Blonde S.A. Interbrew Brussels, Belgium 6.6% 22 AbBIBCbKE Lvivske Premium Lager Lvivska Brewery, Ukraine 5.2% 23 Acadian Pilsener Acadian Brewing Co. LLC New Orleans, LA 24 Acme Brown Ale North Coast Brewing Co. Fort Bragg, CA 25 Actien~Alt-Dortmunder Actien Brauerei Dortmund,Germany 5.6% 26 Adnam's Bitter Sole Bay Brewery Southwold UK 27 Adnams Suffolk Strong Bitter (SSB) Sole Bay Brewery Southwold UK 28 Aecht Ochlenferla Rauchbier Brauerei Heller Bamberg Bamberg, Germany 4.5% 29 Aegean Hellas Beer Atalanti Brewery Atalanti,Greece 4.8% 30 Affligem Dobbel Abbey Ale N.V. -

Draught Lager
46 Lager Draught Lager PREMIUM DRAUGHT LAGER 4378 Asahi 5.0 11 Gall (S) CO2 6380 Hop House 13 5.0 30 Litre (A) CO2 1259 Birra Moretti 4.6 50 Litre (S) CO2 4332 Kaltenberg Royal 4.1 11 Gall (S) CO2 4222 Birra Poretti 4.8 30 Litre (S) CO2 4249 Kingfisher 4.3 30 Litre (S) CO2 4370 Bitburger Pils 4.8 11 Gall (G) CO2 4346 Kingfisher Premium 4.3 11 Gall (S) CO2 4201 Brahma 5.0 10 Gall (U) CO2 4799 Kirin Ichiban 4.6 11 Gall (S) CO2 4244 Budvar Budweiser 5.0 11 Gall (S) CO2 7003 Konig Pilsner 4.9 11 Gall (G) CO2 4420 Budweiser 4.5 11 Gall (G) CO2 4695 Kozel Czech 4.0 11 Gall (S) CO2 0333 Caledonian Coast To Coast 4.6 30 Litre (S) CO2 9736 Krombacher Pils 4.8 50 Litre (A) CO2 6661 Camden Hells Lager 4.6 30 Litre (A) CO2 4639 Kronenbourg 1664 5.0 22 Gall (S) CO2 4239 Carlsberg Export 5.0 30 Litre (S) CO2 4307 Kronenbourg 1664 5.0 11 Gall (S) CO2 4229 Carlsberg Export 5.0 11 Gall (S) CO2 4272 Leffe Blonde 6.6 20 Litre (S) CO2 4479 Chimay Gold 4.8 20 Litre (A) CO2 4216 Leffe Blonde 6.6 6 Litre (PD) CO2 4488 Cobra 4.3 11 Gall (G) CO2 4867 Löwenbrau 5.0 11 Gall (G) CO2 1352 Desperados 5.9 30 Litre (S) CO2 8199 Lucky Saint Unfiltered Lager LOW 0.5 30 Litre (S) CO2 4739 Dortmunder Pils 5.0 11 Gall (S) CO2 3603 Mahou 5.5 30 Litre (S) CO2 0445 Draught Master Angelo Poretti No9 5.9 20 Litre (DM) N/A 4223 Moretti 4.5 30 Litre (S) CO2 0449 Draught Master Brooklyn Lager 5.2 20 Litre (DM) N/A 4810 Moretti 'David' 4.6 20 Litre CO2 3209 Draught Master Carlsberg 3.8 20 Litre (DM) N/A 4524 Peroni Nastro Azzurro 5.2 11 Gall (S) CO2 0449 Draught Master Carlsberg Export -

Raport Odpowiedzialności Społecznej Grupy Żywiec Za Lata 2009-2011
Raport odpowiedzialności społecznej Grupy Żywiec za lata 2009-2011 Raport odpowiedzialności społecznej Grupy Żywiec za lata 2009-2011 List Prezesa Zarządu Szanowni Państwo, Trzymacie Państwo w ręku bezprecedensowe wydawnictwo. Grupa Żywiec jako pierwsza spółka w Polsce udostępnia swoim interesariuszom trzy dokumenty w jednej publikacji – Raport Roczny 2011, Raport „Wpływ Grupy Żywiec na oto- czenie społeczno-gospodarcze w latach 2010-2011” oraz Raport odpowiedzial- ności społecznej 2009-2011, będący pierwszym od trzech lat dokumentem podsumowującym zaangażowanie społeczne Grupy Żywiec. Zarówno Raport Roczny, jak i Raport odpowiedzialności społecznej zostały zbadane przez nieza- leżnych audytorów. Decyzja o wydaniu publikacji w formule „3 w 1” dowodzi naszego sposobu pa- trzenia na działalność gospodarczą. Uważamy, że warunkiem sine qua non udanej i efektywnej aktywności biznesowej jest jej nierozerwalny, synergiczny związek z otoczeniem zewnętrznym (środowiskiem naturalnym, lokalnymi spo- łecznościami, partnerami biznesowymi) i wewnętrznym (naszymi pracownikami). Mam świadomość, że odwoływanie się do społecznej odpowiedzialności biznesu jest dziś bardzo modne. Mamy nadzieję, że nasze podejście to nie tylko kwestia mody, ale wyrastająca z wnętrza organizacji chęć bycia prawdziwym liderem CSR w Polsce – firmą, która wyznacza standardy i dobre praktyki odpowiedzialnego biznesu na polskim rynku. Przede wszystkim uważamy, że odpowiedzialny biznes zaczyna się od aktywnego słuchania, dlatego wdrożyliśmy unikalną platformę komunikacji – proces Dialogu Społecznego, realizowany według międzynarodo- wego standardu AA1000SES (AccountAbility 1000 Stakeholder Engagement Standard). Jesteśmy jedyną firmą w branży i jedną z nielicznych w Polsce, które uruchomiły ten proces na tak wielką skalę. Rozmowa i formułowanie wzajemnych oczekiwań pozwalają nam zarządzać firmą w sposób zrównoważony, z uwzględnieniem dłu- goterminowej perspektywy. Dzięki temu, wykorzystując dostępne dziś zasoby naturalne, nie pozbawiamy przyszłych pokoleń możliwości korzystania z nich. -

College Liquors Beer List
College Liquors Beer List 33 Export Alimony Ale IPA 3 Monts Amber Ale Allagash Hugh Malone 3 Monts Golden Ale Almaza Beer 4 + Brewing Punk’n Alvine Podge Imp. Stout 471 ESB Amacord La Mi Dona 5 Barrel Pale Ale Amacord La Putena A Keiths Brown Amacord La Tabachera A Keiths Lager Amacord Prima Donna A Keiths Pale Amager Fru Frederiks Abita Amber Amstel Light Abita Christmas Ale Anchor Christmas Ale Abita Jock IPA Anchor Liberty Ale Abita Mardi Gras Bock Anchor Old Foghorn Abita Purple Haze Anchor Porter Abita Save Our Shore Anchor Small Beer Abita Strawberry Anchor Steam Beer Abita Turbo Dog Anchor Summer Beer Ace Apple Honey Anchor X-mas Ale Ace Joker Cider Anderson Valley Hop Ottin’ IPA Ace Pear Cider Anderson Valley Bro Dav Doub Ace Pils Anderson Valley Bro Day Trip Ace Wild Berry Anderson Valley Summer Achel 8 Brown Anderson Valley Poleeko Admiral Nelsons Cherry Anderson Valley Amber Aecht Rauchbier Marzen Anderson Valley Brew IPA Aecht Schlenkeria Weizen Anderson Valley Imp. IPA Aecht Urbock Anderson Valley IPA Affigem Blond Anderson Valley Winter Affigem Dubbel Anderson Valley Boont Amber Affigem Noel Apcehajibhoe Extra Affigem Tripel Arron Dark Ale Aktien D Bock Buronat Asahi Aktien Dunkel Asahi Black Aktien Jubilaums Asahi Kuronama Black Aktien October Fest Asahi Super Dry Alaskan Amber Aspall Medium Cider Alaskan IPA Aspall Organic Cider Alaskan Smoked Porter Augustinerbrau Edelst Alaskan Stout Augustinebrau Maxi Alaskan Summer Avec Les Bons Dupont Alaskan White Avery 14’er ESB SGL BTL Alba Scots Pine Avery 14’er ESB Aldaris Gaisais -
Drinks Menu Gin
beeR & g ft in a r L c I V E y k S P s i O h R T w S D C O O O T F T I S H MEAL AN’ ALE DRINKS MENU GIN #MCGINTYSABERDEEN WWW.MCGINTYSMEALANALE.CO.UK GIN ABERDEEN & SHIRE Esker Gin 42% Royal Deeside, Aberdeenshire ABV Orange peel – Crisp, clean & juniper led with notes of citrus & floral botanicals Indian Summer Gin 46% Huntly, Aberdeenshire ABV Sprig of thyme- Sweet & earthy saron infused gin Porter’s Gin 41.5% Aberdeen ABV Lime – Bold juniper with a fresh citrus profile Teasmith Gin 43% Udny, Aberdeenshire ABV Sprig of mint – Light on the palate, distinct crisp taste House of Elrick Gin 42% Newmacher, Aberdeenshire ABV Orange – Fresh, yet unearthy bold fusion of flavours with fresh loch ness water & rose petals ANGUS Arbikie Kirsty’s Gin 43% Inverkeilor, Angus ABV Blueberries – Smooth gin with blaeberries, kelp & thistle Gin Bothy Original 41% ANGUS ABV Slice of orange - Refreshing with heather, milk thistle, Scottish pine needles, hawthorn root & rosemary PAGE 3 ARGYLL Old Raj Red 47% Campbeltown ABV Orange Zest – Saron infused gin with a slight spicy flavour Hendrick’s Gin 40% Girvan, Ayrshire ABV Cucumber – Cucumber & rose petal infused with a sweet floral aroma EDINBURGH Daffy’s Gin 43.4% Edinburgh ABV Mint leaves – Lebanese mint taste with a crisp refreshing edge & smooth finish Edinburgh Gin 43% EDINBURGH ABV Orange – Classic gin with notes of heather & milk Edinburgh Elderflower Gin 20% EDINBURGH ABV Wedge of Lime - Crisp, fresh & sweet elderflower aromas Edinburgh Raspberry Gin 20% EDINBURGH ABV Raspberries – Infused with Perthshire -
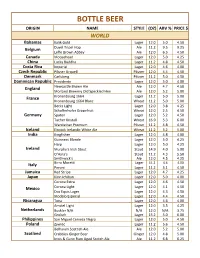
Half Wall Menu Beer
BOTTLE BEER ORIGIN NAME STYLE (OZ) ABV % PRICE $ WORLD Bahamas Kalik Gold Lager 12.0 5.0 4.50 Belgium Duvel Tripel Hop Ale 11.2 9.5 9.25 Leffe Brown Abbey Ale 12.0 6.5 4.50 Canada Moosehead Lager 12.0 5.0 4.25 China Lucky Buddha Lager 11.2 4.8 4.50 Costa Rica Imperial Lager 12.0 4.6 4.00 Czech Republic Pilsner Urquell Pilsner 12.0 4.4 4.50 Denmark Carlsberg Pilsner 11.2 5.0 4.50 Dominican Republic Presidente Lager 12.0 5.0 4.00 England Newcastle Brown Ale Ale 12.0 4.7 4.50 Morland Brewery Old Speckled Hen Ale 12.0 5.2 5.00 France Kronenbourg 1664 Lager 11.2 5.0 5.00 Kronenbourg 1664 Blanc Wheat 11.2 5.0 5.00 Becks Light Lager 12.0 3.8 4.25 Schofferhofer Grapefruit Wheat 12.0 2.5 4.50 Germany Spaten Lager 12.0 5.2 4.50 Tucher Kristall Wheat 16.9 5.3 6.00 Warsteiner Premium Pilsner 11.2 4.8 4.50 Iceland Einstok Icelandic White Ale Wheat 11.2 5.2 5.00 India Kingfisher Lager 12.0 4.8 4.00 Guinness Blonde Lager 12.0 5.0 4.25 Harp Lager 12.0 5.0 4.25 Ireland Murphy's Irish Stout Stout 14.9 4.0 5.00 O'Hara's Stout 11.2 4.3 5.50 Smithwick's Ale 12.0 4.5 4.25 Italy Birra Moretti Lager 11.2 4.6 4.00 Peroni Lager 11.2 5.1 4.50 Jamaica Red Stripe Lager 12.0 4.7 4.25 Japan Kirin Ichiban Lager 12.0 5.0 4.00 Corona EXtra Lager 12.0 4.6 4.50 Mexico Corona Light Lager 12.0 4.1 4.50 Dos Equis Lager Lager 12.0 4.3 4.50 Modelo Especial Lager 12.0 4.4 4.50 Nicaragua Tona Lager 12.0 4.6 4.00 Amstel Light Lager 12.0 3.5 4.25 Netherlands Buckler N/A N/A 12.0 N/A 3.75 Grolsch Lager 15.2 5.0 6.00 Philippines San Miguel Cerveza Negra Lager 12.0 5.0 4.50 Poland -

Menu.20123845.Pdf
Catering Menu Family Owned & Operated since 1994 10% OFF CD BEER LIST Coming soon CD BEER LIST % Wine Delivery! All trays Serve 18 - 20 people 10 OFF CD Pizza And House of Brews Redd’s Blueberry Ale 12 PACK (PBR) 4.74% Any Online Now Delivering Beer….right to your door! Miller Brewing Co. 5% Bud Light 4.2% Presidente 5% We Take Custom Redd’s Peach Ale Budweiser 5% Catering Orders! Order Look on our website for the most up-to-date beer list. Seasonals are consistently Miller Brewing Co. 5% Redd’s Wicked rotating, if you don’t see it, we have access to over 150+ breweries and over 800 Cerveceria Corona Apple 8% Please call Nino for more details beer & malt products. Let us know how we can better serve your needs, we love Rolling Rock Variety Pack 4.6% Redd’s Wicked customer feedback. Labatt Brewing Co. Ltd. Coors Light 4.27% 4.5% Mango 8% Salad 717-652-8844 We deliver beer – must be paid for ahead of time with a credit card. Federal & Labatt Blue 4% Mention offer when ordering. No coupon State laws require purchasers of alcoholic beverages must be 21 years of age or Samuel Adams Seagram’s Escapes Chef 50.00 necessary. Not valid with other offers. Michelob Ultra 4.2% Varieties 3.2% Discount does not apply to alcohol. Limited older, and must provide valid photo identification at time of delivery. Boston Lager Antipasto 50.00 time offer Boston Beer Co. 5.4% Mike’s Hard Lemonade Smirnoff Ice Spiked Identification must match credit card used for purchase. -
2015 BJCP Beer Style Guidelines
BEER JUDGE CERTIFICATION PROGRAM 2015 STYLE GUIDELINES Beer Style Guidelines Copyright © 2015, BJCP, Inc. The BJCP grants the right to make copies for use in BJCP-sanctioned competitions or for educational/judge training purposes. All other rights reserved. Updates available at www.bjcp.org. Edited by Gordon Strong with Kristen England Past Guideline Analysis: Don Blake, Agatha Feltus, Tom Fitzpatrick, Mark Linsner, Jamil Zainasheff New Style Contributions: Drew Beechum, Craig Belanger, Dibbs Harting, Antony Hayes, Ben Jankowski, Andew Korty, Larry Nadeau, William Shawn Scott, Ron Smith, Lachlan Strong, Peter Symons, Michael Tonsmeire, Mike Winnie, Tony Wheeler Review and Commentary: Ray Daniels, Roger Deschner, Rick Garvin, Jan Grmela, Bob Hall, Stan Hieronymus, Marek Mahut, Ron Pattinson, Steve Piatz, Evan Rail, Nathan Smith,Petra and Michal Vřes Final Review: Brian Eichhorn, Agatha Feltus, Dennis Mitchell, Michael Wilcox TABLE OF CONTENTS 5B. Kölsch ...................................................................... 8 INTRODUCTION TO THE 2015 GUIDELINES............................. IV 5C. German Helles Exportbier ...................................... 9 Styles and Categories .................................................... iv 5D. German Pils ............................................................ 9 Naming of Styles and Categories ................................. iv Using the Style Guidelines ............................................ v 6. AMBER MALTY EUROPEAN LAGER .................................... 10 Format of a -

Bierliste Ausland Biername Brauerei Stadt Land Note Birell Non-Alcoholic (Gebr
Bierliste Ausland Biername Brauerei Stadt Land Note Birell Non-Alcoholic (gebr. in Ägypten) Al Ahram Beverages Co. Giza Ägypten 4,5 Heineken Lager Premium Al Ahram Beverages Co. Giza Ägypten 3,5 Meister Lager Al Ahram Manufacturing and Filling Co. Giza Ägypten 3,5 Sakara Gold Lager Al Ahram Beverages Co. Giza Ägypten 3,6 Stella Export Lager Al Ahram Beverages Co. Giza Ägypten 3,8 Stella Lager Al Ahram Beverages Co. Giza Ägypten 3,3 Stella Lager 115 Years Al Ahram Beverages Co. Giza Ägypten 3,0 Patagonia Estilo Amber Lager Cerveceria Quilmes SAICAY Buenos Aires Argentinien 2,7 Quilmes Cerveza Cerveceria Malteria Quilmes Buenos Aires Argentinien 4,0 Quilmes Cerveza Cristal Cerveceria Malteria Quilmes Buenos Aires Argentinien 3,8 Bati Beer Lager Kombolcha Brewery Kombolcha Äthiopien 3,7 Castlemaine XXXX Gold Lager Castlemaine Perkins Milton Brisbane Australien 3,7 Coopers Sparkling Ale Coopers Brewery LTD. Regency Park Australien 3,3 Foster´s Lager Carlton & United Melbourne Australien 4,0 James Boag's Premium Lager J. Boag & Son Brewing Launceston Australien 3,7 Reschs Pilsener Carlton & United Breweries Sydney Australien 4,3 Victoria Bitter Lager Carlton & United Breweries Southbank Australien 4,0 Banks Caribbean Lager Banks Breweries LTD. Christ Church Barbados 2,7 400 Jaar Brandaris Terschelling door Brouwerij Van Steenberge Ertvelde Belgien 3,8 Abbaye d´Aulne Amber Brasserie Val de Sambre Gozee Belgien 4,4 Abbaye du Val-Dieu Biere de Noel Brasserie de l´Abbaye du Val-Dieu Aubel Belgien 3,3 Adelardus Trudoabdijbier Tripel Brouwerij Kerkom Sint-Truiden Belgien 3,8 Archivist Hell Brouwerij De Brabandere Bavikhove Belgien 3,5 Arend blond Brouwerij De Ryck Herzele Belgien 4,3 Baltimore-Washington Beer Works Route US 66 Brewery Strubbe Ichtegem Belgien 3,0 Barista Chocolate Quad Br. -

Ingredients & Nutritional Information
PRODUCT INGREDIENTS NUTRITION FACTS* HEINEKEN LAGER 5.0% ABV; Water, malted barley and hop Calories 142; Carbohydrates 11g; extract Fat 0g; Protein 2g HEINEKEN LIGHT 3.3% ABV; Water, malted barley, glucose, hops Calories 99; Carbohydrates 7g; Fat 0g; Protein 1g and hop extract HEINEKEN 0.0% 0.0% ABV#; Water, malted barley and hop Calories 69; Carbohydrates 16g; extract Fat 0g; Protein 0g AMSTEL LIGHT 3.5% ABV; Water, malted barley, glucose and Calories 95; Carbohydrates 5g; hop extract Fat 0g; Protein 1g BUCKLER <0.5% ABV; Water, malted barley and hop Calories 99; Carbohydrates 20g; extract Fat 0g; Protein 1g DOS EQUIS LAGER 4.2% ABV; Water, malted barley, corn starch Calories 131; Carbohydrates 11g; Fat 0g; Protein 1g and hop extract DOS EQUIS AMBAR 4.7% ABV; Water, malted barley, corn starch Calories 146; Carbohydrates 14g; and hop extract Fat 0g; Protein 1g DOS EQUIS 5.5% ABV; MEXICAN PALE ALE Calories 175; Carbohydrates 15g; Water, malted barley, corn starch Fat 0g; Protein 2g and hops TECATE ORIGINAL 4.5% ABV; Water, malted barley, corn starch Calories 142; Carbohydrates 14g; Fat 0g; Protein 1g and hops TECATE LIGHT 3.9% ABV; Water, malted barley, corn starch Calories 106; Carbohydrates 7g; and hop extract Fat 0g; Protein 1g MICHELADA DIABLO 3.5% ABV; Water, malted barley, corn syrup, Calories 135; Carbohydrates 15g; tomato juice, citric acid, hop extract, Fat 0g; Protein 1g salt, natural flavors and ascorbic acid TECATE TITANIUM 7.5% ABV; Water, malted barley, corn starch Calories 194; Carbohydrates 10g; and hops Fat 0g; Protein -

HEINEKEN Listing Références 26042021
Liste des références Durée Code DDM Nouvelle DDM Marque Designation Extension Heineken (en mois) (en mois) (en mois) 33 EXPORT 1000025711 33 Exp / Biere De Luxe Fut 30 L Ndg 6 2 8 AFFLIGEM 1000026904 AFFLIGEM BLADE 8L 9 2 11 AFFLIGEM 1000027437 AFFLIGEM Fût 30 L 9 1 10 AFFLIGEM 1000027439 AFFLIGEM Fût 20 L 9 1 10 AFFLIGEM 1000027438 AFFLIGEM Fût 20 L David 9 1 10 AFFLIGEM 1000026904 AFFLIGEM BLADE 8L 9 2 11 AFFLIGEM AMBRE 1000027399 AFFLIGEM Ambrée Fût 20L 6 2 8 AFFLIGEM CARMIN 1000026283 Affligem Cuvee Carmin2 Fut 20 L 6 2 8 AFFLIGEM CARMIN 1000026924 AFFLIGEM CARMIN BLADE 8L 9 2 11 AFFLIGEM CUVEE LEGERE 1000026851 Affligem Cuvee Legere Fut 30L 6 2 8 AFFLIGEM CUVEE LEGERE 1000026925 AFFLIGEM LEGERE BLADE 8L 9 2 11 AFFLIGEM DE NOËL 1000025518 AFFLIGEM De Noël Fût 30L FR 6 2 8 AFFLIGEM DE NOËL 1000027442 AFFLIGEM DE NOËL BLADE 8L 9 2 11 AFFLIGEM TRIPLE 1000026473 Affligem Triple Fut 20 L 6 2 8 AMSTEL 1000027436 AMSTEL Fût 30 L 9 1 10 BIRRA MORETTI 1000026846 BIRRA MORETTI BLADE 8L 9 2 11 BRIXTON LOW VOLTAGE 1000027350 Brixton Low Volt. S.Ipa Fut 20L 6 2 8 BUCKLER 1000026368 Buckler Fut 20L 6 2 8 BUCKLER 1000026370 Buckler Fut 20 L David 6 2 8 CINEY BLONDE 1000026194 Ciney Blonde Fut 20 L 6 2 8 CINEY BRUNE 1000026782 Ciney Brune Fut 20 L 6 2 8 CRUZCAMPO 1000025521 Cruzcampo Fut 30 L 6 2 8 DESPERADOS 1000025523 Desperados Fut 20 L 6 2 8 DESPERADOS 1000026905 DESPERADOS BLADE 8L 9 2 11 EDELWEISS 1000025515 Edelweiss Fut 20 L 6 2 8 EDELWEISS 1000026906 EDELWEISS BLADE 8L 9 2 11 FISCHER DE NOËL 1000025529 FISCHER De Noël Fût 30L FR 6 2 8 FISCHER -

Product Ingredients Nutrition
PRODUCT INGREDIENTS NUTRITION FACTS* HEINEKEN LAGER 5.0% ABV; Water, malted barley and hop Calories 142; Carbohydrates 11g; extract Fat 0g; Protein 2g HEINEKEN LIGHT 3.3% ABV; Water, malted barley, glucose, hops Calories 99; Carbohydrates 7g; Fat 0g; Protein 1g and hop extract AMSTEL LIGHT 3.5% ABV; Water, malted barley, glucose and Calories 99; Carbohydrates 5g; hop extract Fat 0g; Protein 1g AMSTEL XLIGHT 4.2% ABV; Water, malted barley, glucose and Calories 90; Carbohydrates 2g; hop extract Fat 0g; Protein 0g BUCKLER <0.5% ABV; Water, malted barley and hop Calories 99; Carbohydrates 20g; extract Fat 0g; Protein 1g H41 WILD LAGER 5.3% ABV; Water, malted barley and hop Calories 192; Carbohydrates 19g; Fat 0g; Protein 2g extract DOS EQUIS LAGER 4.2% ABV; Water, malted barley, corn Calories 131; Carbohydrates 11g; Fat 0g; Protein 1g starch/syrup and hop extract DOS EQUIS AMBAR 4.7% ABV; Water, malted barley, corn Calories 146; Carbohydrates 14g; starch/syrup and hop extract Fat 0g; Protein 1g TECATE ORIGINAL 4.5% ABV; Water, malted barley, corn Calories 142; Carbohydrates 14g; Fat 0g; Protein 1g starch/syrup and hops TECATE LIGHT 3.9% ABV; Water, malted barley, corn Calories 106; Carbohydrates 7g; starch/syrup and hop extract Fat 0g; Protein 1g MICHELADA DIABLO 3.5% ABV; Water, malted barley, corn syrup, Calories 135; Carbohydrates 15g; tomato juice, citric acid, hop extract, Fat 0g; Protein 1g salt, natural flavors and ascorbic acid BOHEMIA PILSEN 4.7% ABV; Water, malted barley, corn Calories 150; Carbohydrates 13g; starch/syrup and hops