Rapid Assessment of a Global Health Security Agenda Project 1 ACKNOWLEDGMENTS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Week 16: 12-18 April 2021
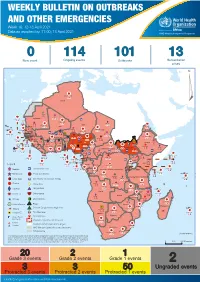
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 16: 12-18 April 2021 Data as reported by: 17:00; 18 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 114 101 13 New event Ongoing events Outbreaks Humanitarian crises 119 642 3 155 Algeria ¤ 36 13 110 0 5 694 170 Mauritania 7 2 13 070 433 110 0 7 0 Niger 17 129 453 Mali 3 491 10 567 0 6 0 2 079 4 4 706 169 Eritrea Cape Verde 39 782 1 091 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 20 466 191 973 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 242 028 3 370 0 164 233 2 061 Guinea 13 129 154 12 38 397 1 3 712 66 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 481 5 6 188 15 Sierra Leone Togo 3 473 296 61 731 919 52 14 Ghana 5 787 75 Côte d'Ivoire 10 473 114 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 97 17 25 0 21 612 260 45 560 274 91 709 771 Cameroon 7 0 28 676 137 5 330 13 151 653 2 481 655 2 43 0 119 12 6 1 488 6 4 028 79 12 533 7 259 106 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 066 85 41 378 338 Kenya Legend 7 611 95 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 275 35 23 888 325 Measles 21 858 133 Democratic Republic of the Congo 10 084 137 Burundi 3 612 6 Monkeypox Ebola virus disease Seychelles 28 956 745 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 190 0 4875 25 509 21 Cholera Yellow fever 1 349 5 6 257 229 24 389 561 cVDPV2 Dengue fever 90 918 1 235 Comoros Angola Malawi COVID-19 Chikungunya 33 941 1 138 862 0 3 815 146 Zambia 133 0 Mozambique -
Livelihood Zone Descriptions
Government of Senegal COMPREHENSIVE FOOD SECURITY AND VULNERABILITY ANALYSIS (CFSVA) Livelihood Zone Descriptions WFP/FAO/SE-CNSA/CSE/FEWS NET Introduction The WFP, FAO, CSE (Centre de Suivi Ecologique), SE/CNSA (Commissariat National à la Sécurité Alimentaire) and FEWS NET conducted a zoning exercise with the goal of defining zones with fairly homogenous livelihoods in order to better monitor vulnerability and early warning indicators. This exercise led to the development of a Livelihood Zone Map, showing zones within which people share broadly the same pattern of livelihood and means of subsistence. These zones are characterized by the following three factors, which influence household food consumption and are integral to analyzing vulnerability: 1) Geography – natural (topography, altitude, soil, climate, vegetation, waterways, etc.) and infrastructure (roads, railroads, telecommunications, etc.) 2) Production – agricultural, agro-pastoral, pastoral, and cash crop systems, based on local labor, hunter-gatherers, etc. 3) Market access/trade – ability to trade, sell goods and services, and find employment. Key factors include demand, the effectiveness of marketing systems, and the existence of basic infrastructure. Methodology The zoning exercise consisted of three important steps: 1) Document review and compilation of secondary data to constitute a working base and triangulate information 2) Consultations with national-level contacts to draft initial livelihood zone maps and descriptions 3) Consultations with contacts during workshops in each region to revise maps and descriptions. 1. Consolidating secondary data Work with national- and regional-level contacts was facilitated by a document review and compilation of secondary data on aspects of topography, production systems/land use, land and vegetation, and population density. -

2019-2020 CAS Research Report
CENTER FOR AFRICAN STUDIES RESEARCH REPORT 2019-2020 THE CENTER WOULD LIKE TO THANK Modesta Abugu for coordinating the project and Jenna Agres for design and layout. Cover photos courtesy of Sebastian Elischer, Yekatit Tsehayu, Frederick Madore, and Vincent Girier Dufournier. TABLEtable of contents OF CONTENTS ABOUT THE CENTER ..............................................................................................................................................................................................4 FROM THE DIRECTOR ............................................................................................................................................................................................6 NATURAL RESOURCE MANAGEMENT WORKING GROUP ...........................................................................................................8 CHINA-AFRICA WORKING GROUP ..............................................................................................................................................................9 WOMEN’S PARTICIPATION IN LIVESTOCK VACCINE VALUE CHAINS ...............................................................................10 CPET GLOBAL HEALTH INSTITUTE ............................................................................................................................................................11 RESEARCH TUTORIALS ABROAD ..............................................................................................................................................................12 -

Dengue Fever in Senegal 6 - 7 Ongoing Events Ebola Virus Disease in the Democratic Republic of the Congo Humanitarian Crisis in Cameroon
Overview Contents This Weekly Bulletin focuses on selected acute public health emergencies occurring in the WHO African Region. The WHO Health Emergencies Programme is currently monitoring 58 events in the region. This week’s edition covers key new and ongoing events, including: 2 Overview Hepatitis E in Central African Republic 3 - 5 New events Monkeypox in Central African Republic Dengue fever in Senegal 6 - 7 Ongoing events Ebola virus disease in the Democratic Republic of the Congo Humanitarian crisis in Cameroon. 8 Summary of major issues challenges and For each of these events, a brief description, followed by public health proposed actions measures implemented and an interpretation of the situation is provided. 9 All events currently A table is provided at the end of the bulletin with information on all new and being monitored ongoing public health events currently being monitored in the region, as well as events that have recently been closed. Major issues and challenges include: The Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo has reached a critical juncture, marked by a precarious security situation, persistence of pockets of community resistance/ mistrust and expanding geographical spread of the disease. During the reporting week, there was an incident involving a response team performing burial activity in Butembo. This came barely days following a widespread community strike (“ville morte”) in Beni and several towns, and an earlier armed attack in Beni. These incidents severely disrupted most outbreak control interventions. Meanwhile, EVD cases have been confirmed in new areas with worse insecurity and in close proximity to the border with Uganda. -

Figure 4.1 Map of Dakar, Senegal...29
Public Disclosure Authorized Baseline and feasibility assessment for alternative cooking fuels in Senegal Public Disclosure Authorized May 2014 Public Disclosure Authorized Public Disclosure Authorized © 2014 The International Bank for Reconstruction and Development / The World Bank 1818 H Street NW, MSN U11-1102 Washington DC 20433 Telephone: 202-458-7955 Fax: 202-522-2654 Website: http:// www.worldbank.org All rights reserved The findings, interpretations, and conclusions expressed herein are those of the author(s) and do not necessarily reflect the views of the Board of Executive Directors of the World Bank or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of the World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Rights and Permissions The material in this work is copyrighted. Copying and/or transmitting portions or all of this work without permission may be a violation of applicable law. The World Bank encourages dissemination of its work and will normally grant permission promptly. Baseline and feasibility assessment for alternative cooking fuels in Senegal 2 Contents Acronyms and abbreviations ............................................................................................. 6 Acknowledgments ............................................................................................................. -

SENEGAL Last Updated: 2007-05-22
Vitamin and Mineral Nutrition Information System (VMNIS) WHO Global Database on Iodine Deficiency The database on iodine deficiency includes data by country on goitre prevalence and/or urinary iodine concentration SENEGAL Last Updated: 2007-05-22 Goitre Urinary iodine (µg/L) Notes prevalence (%) Distribution (%) Prevalence (%) Age Sample Grade Grade TGP <20 20-49 50-99100-299 >300 <100 Median Mean SD Reference General Line Level Date Region and sample descriptor Sex (years) size 1 2 D 2003 Véligara department: SAC by area: Urban B 6.00 - 12.99 65 53.8 12.7 5128 * Véligara department: SAC by area: Rural B 6.00 - 12.99 84 40.5 25.4 Vélingara department: SAC by area: Urban B 6.00 - 12.99 677 2.2 * Vélingara department: SAC by area: Rural B 6.00 - 12.99 878 1.2 Vélingara department: Women by area: Urban F NS 358 5.3 Vélingara department: Women by area: Rural F NS 306 4.2 Vélingara department: PW by area: Urban F NS 46 13.0 Vélingara department: PW by area: Rural F NS 61 11.5 L 1999P Casamance area: 6 villages: All B 5.00 - 60.99 109 97.0 20.0 1563 * 1 Casamance area: 6 villages: All B 5.00 - 60.99 160 30.0 10.6 40.6 * L 1997 Bambey, Kebemer and Koungheul: SAC B 6.00 - 12.99 400 15.0 28.0 38.0 81.0 5129 * S 1995 -1997 Tambacounda and Casamance regions: All: Total B 10.00 - 50.99 8797 21.5 24.5 18.3 64.4 5282 * Tambacounda and Casamance regions: PW F NS 462 50.0 All by region: Tambacounda urban B 10.00 - 50.99 866 17.7 25.1 24.2 67.0 61.1 All by region: Tambacounda rural B 10.00 - 50.99 793 43.6 37.2 12.8 93.6 23.0 All by department: Bakel B -
Creating Markets in Senegal
CREATING MARKETS SENEGAL IN CREATING A COUNTRY PRIVATE SECTOR DIAGNOSTIC SECTOR PRIVATE COUNTRY A A COUNTRY PRIVATE SECTOR DIAGNOSTIC CREATING MARKETS IN SENEGAL Sustaining growth in an uncertain environment APRIL 2020 About IFC IFC—a sister organization of the World Bank and member of the World Bank Group—is the largest global development institution focused on the private sector in emerging markets. We work with more than 2,000 businesses worldwide, using our capital, expertise, and influence to create markets and opportunities in the toughest areas of the world. In fiscal year 2018, we delivered more than $23 billion in long-term financing for developing countries, leveraging the power of the private sector to end extreme poverty and boost shared prosperity. For more information, visit www.ifc.org © International Finance Corporation 2020. All rights reserved. 2121 Pennsylvania Avenue, N.W. Washington, D.C. 20433 www.ifc.org The material in this report was prepared in consultation with government officials and the private sector in Senegal and is copyrighted. Copying and/or transmitting portions or all of this work without permission may be a violation of applicable law. IFC does not guarantee the accuracy, reliability or completeness of the content included in this work, or for the conclusions or judgments described herein, and accepts no responsibility or liability for any omissions or errors (including, without limitation, typographical errors and technical errors) in the content whatsoever or for reliance thereon. The findings, interpretations, views, and conclusions expressed herein are those of the authors and do not necessarily reflect the views of the Executive Directors of the International Finance Corporation or of the International Bank for Reconstruction and Development (the World Bank) or the governments they represent. -

Bayesian Spatial Models Applied to Malaria Epidemiology
Bayesian spatial models applied to malaria epidemiology INAUGURALDISSERTATION zur Erlangung der W¨urdeeines Doktors der Philosophie vorgelegt der Philosophisch-Naturwissenschaftlichen Fakult¨at der Universit¨atBasel von Federica Giardina aus Pescara, Italien Basel, December 2015 Original document stored on the publication server of the University of Basel edoc.unibas.ch Genehmigt von der Philosophisch-Naturwissenschaftlichen Fakult¨atauf Antrag von Prof. Dr. M. Tanner, P.D. Dr. P. Vounatsou, and Prof. Dr. A. Biggeri. Basel, den 10 December 2013 Prof. Dr. J¨orgSchibler Dekan Science is built up with facts, as a house is with stones. But a collection of facts is no more a science than a heap of stones is a house. (Henri Poincar´e) iv Summary Malaria is a mosquito-borne infectious disease caused by parasitic protozoans of the genus Plasmodium and transmitted to humans via the bites of infected female Anopheles mos- quitoes. Although progress has been seen in the last decade in the fight against the disease, malaria remains one of the major cause of morbidity and mortality in large areas of the developing world, especially sub-Saharan Africa. The main victims are children under five years of age. The observed reductions are going hand in hand with impressive increases in international funding for malaria prevention, control, and elimination, which have led to tremendous expansion in implementing national malaria control programs (NMCPs). Common interventions include indoor residual spraying (IRS), the use of insecticide treated nets (ITN) and environmental measures such as larval control. Specific targets have been set during the last decade. The Millennium Development Goal (MDG) 6 aims to halve malaria incidence by 2015 as compared to 1990 and to achieve universal ITN coverage and treatment with appropriate antimalarial drugs. -

Final Report Assessment of Health Related Investment and Financing Opportunities in Senegal
FINAL REPORT ASSESSMENT OF HEALTH RELATED INVESTMENT AND FINANCING OPPORTUNITIES IN SENEGAL Financing Growth Work Order 2014-03 Contract No. AID-EEM-E-00-08-00002 Order No. AID-OAA-BC-14-00030 March 2015 This document was prepared by Banyan Global under Financing Growth: Assessment of Health Related Investment and Financing Opportunities in Senegal. ASSESSMENT OF HEALTHCARE RELATED INVESTMENT AND FINANCING OPPORTUNITIES IN SENEGAL FINAL REPORT MARCH 2015 Contract No.: AID-EEM-E-00-08-00002 Order No: AID-OAA-BC-14-0030 Work Order No. 2014-03 Submitted to: Lawrence Camp, COR Director USAID, Millennium Challenge Corporation DISCLAIMER The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development (USAID) or the United States Government. PROJECT OVERVIEW Financing Growth: Assessment of Healthcare Related Name Investment and Financing Opportunities in Senegal Contract Number AID-EEM-E-00-08-00002 Order Number AID-OAA-BC-14-0030 Work Order Number 2014-03 Start Date January 21, 2015 End Date February 28, 2015 Geographic Coverage Senegal Quarterly Progress Report #1, October - December 2014 CONTENTS Acronyms.........................................................................................................................................i 1. Introduction ........................................................................................................................... 2 2. Project Tasks and Activities ................................................................................................ -

A Look Into the Varying Usage Patterns of Traditional and Western Medicine Within Senegal’S Urban Centers
SIT Graduate Institute/SIT Study Abroad SIT Digital Collections Independent Study Project (ISP) Collection SIT Study Abroad Spring 2020 A Look into the Varying Usage Patterns of Traditional and Western Medicine Within Senegal’s Urban Centers Sarah Smith SIT Study Abroad Follow this and additional works at: https://digitalcollections.sit.edu/isp_collection Part of the African Languages and Societies Commons, African Studies Commons, Alternative and Complementary Medicine Commons, Health Communication Commons, Medicine and Health Commons, and the Social and Cultural Anthropology Commons Recommended Citation Smith, Sarah, "A Look into the Varying Usage Patterns of Traditional and Western Medicine Within Senegal’s Urban Centers" (2020). Independent Study Project (ISP) Collection. 3274. https://digitalcollections.sit.edu/isp_collection/3274 This Unpublished Paper is brought to you for free and open access by the SIT Study Abroad at SIT Digital Collections. It has been accepted for inclusion in Independent Study Project (ISP) Collection by an authorized administrator of SIT Digital Collections. For more information, please contact [email protected]. L’Union fait la force: A Look into the Varying Usage Patterns of Traditional and Western Medicine Within Senegal’s Urban Centers Smith, Sarah Academic Director: Brodnicka, Monika Project Advisor: Kante, Fode Swarthmore College Peace and Conflict Studies Senegal, Dakar and Thiès Submitted in partial fulfillment of the requirements for SIT Senegal: Global Security and Religious Pluralism, SIT Study Abroad, Spring 2020 0 TABLE OF CONTENTS Acknowledgments 1 Abstract 1 Introduction 2 Literature Review 3 Methods 11 Ethics 12 Findings and Analysis 13 Conclusion 20 Works Cited 22 Acknowledgments I would like to thank the staff of SIT Senegal for their support of this project, particularly with participant recruitment. -

Neoliberal Effects As Seen in Village Health Dispensaries Within the Kedougou Region of Southeast Senegal Samantha Salter Iowa State University
Iowa State University Capstones, Theses and Graduate Theses and Dissertations Dissertations 2018 Neoliberal effects as seen in village health dispensaries within the Kedougou Region of Southeast Senegal Samantha Salter Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/etd Part of the African Languages and Societies Commons, African Studies Commons, Health and Medical Administration Commons, and the Social and Cultural Anthropology Commons Recommended Citation Salter, Samantha, "Neoliberal effects as seen in village health dispensaries within the Kedougou Region of Southeast Senegal" (2018). Graduate Theses and Dissertations. 16664. https://lib.dr.iastate.edu/etd/16664 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Neoliberal effects as seen in village health dispensaries within the Kedougou Region of Southeast Senegal by Samantha Salter A thesis submitted to the graduate faculty in partial fulfillment of the requirements for the degree of MASTER OF ARTS Major: Anthropology Program of Study Committee: Nell Gabiam, Major Professor Sebastian Braun Donna Winham The student author, whose presentation of the scholarship herein was approved by the program of study committee, is solely responsible for the content of this thesis. The Graduate College will ensure this thesis is globally accessible and will not permit alterations after a degree is conferred. Iowa State University Ames, Iowa 2018 Copyright © Samantha Salter, 2018. -

SÉNÉGAL Rapport Spécial
SENEGAL Special Report August 31, 2015 Poor start to the agropastoral season in central and northern areas KEY MESSAGES This year, farmers are resorting to short-cycle varieties of cowpea and Souna millet crops more than usual as a strategy to limit the negative effects of the late start of the rains on crop production in order to ensure near-average crop yields. With the likely downsizing of the land area planted in groundnuts, Senegal’s main cash crop, household incomes between December and March will likely be below average. The poor pastoral conditions between February and June severely affected pastoral incomes, which have been well below-average as a result of the decline in animal production and livestock prices. The larger than usual numbers of animal deaths have adversely affected the livelihoods of pastoral households, limiting their food access on local markets. However, the recent recovery of pastures and replenishment of watering holes have helped improve the situation in many pastoral areas. Food assistance from the government and its humanitarian partners is easing poor households’ food insecurity. Humanitarian food and non-food assistance and cash transfer programs will limit the use of atypical coping strategies (ex. borrowing and reducing food and nonfood expenditures) by recipient households. An examination of food prices on domestic markets shows prices for locally grown millet still slightly above-average and prices for regular broken rice, the main foodstuff consumed by Senegalese households, at below-average levels. However, despite these prices, the below-average incomes of poor agropastoral households is preventing many households from adequating accessing these food items.