Pantothenic Acid: an Overview Focused on Medical Aspects
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Cosmeceutical Products List
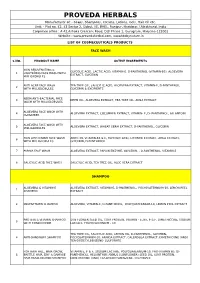
PROVEDA HERBALS Manufacturer of: - Soaps, Shampoos, Creams, Lotions, Gels, Hair Oil etc. Unit: - Plot no. 42, 43 Sector 2, Sidcul, IIE, BHEL, Ranipur, Haridwar, Uttrakhand, India Corporate office : A 42,Ashoka Crescent Road, DLF Phase 1, Gurugram, Haryana-122002 Website : www.provedaherbal.com, www.tbcbynature.in LIST OF COSMECEUTICALS PRODUCTS FACE WASH S.NO. PRODUCT NAME ACTIVE INGREDIENTS SKIN REJUVENATING & GLYCOLIC ACID, LACTIC ACID, VITAMIN-E, D-PANTHENOL (VITAMIN-B5), ALOEVERA 1 LIGHTENING FACE WASH WITH EXTRACT, GLYCERIN MILLIGLOBULES ANTI ACNE FACE WASH TEA TREE OIL, SALICYLIC ACID, ALOEVERA EXTRACT, VITAMIN-E, D-PANTHENOL, 2 WITH MILLIGLOBULES GLYCERIN & EXCIPIENTS NEEM ANTI-BACTERIAL FACE 3 NEEM OIL, ALOEVERA EXTRACT, TEA TREE OIL, AMLA EXTRACT WASH WITH MILLIGLOBULES ALOEVERA FACE WASH WITH 4 ALOEVERA EXTRACT, CUCUMBER EXTRACT, VITAMIN- E, D- PANTHENOL, ALLANTOIN CUCUMBER ALOEVERA FACE WASH WITH 5 ALOEVERA EXTRACT, WHEAT GERM EXTRACT, D-PANTHENOL, GLYCERIN MILLIGLOBULES SKIN LIGHTENING FACE WASH ARBUTIN, VITAMIN-B3 & E, GLYCOLIC ACID, LICORICE EXTRACT, AMLA EXTRACT, 6 WITH MILLIGLOBULES GLYCERIN, D-PANTHENOL 7 PAPAYA FACE WASH ALOEVERA EXTRACT, PAPAIN ENZYME, GLYCERIN, , D-PANTHENOL, VITAMIN-E 8 SALICYLIC ACID FACE WASH SALICYLIC ACID, TEA TREE OIL, ALOE VERA EXTRACT SHAMPOO ALOEVERA & VITAMIN-E ALOEVERA EXTRACT, VITAMIN-E, D-PANTHENOL, POLYQUATERNIUM-10, LEMON PEEL 1 SHAMPOO EXTRACT 2 MULTIVITAMIN SHAMPOO ALOEVERA, VITAMIN-E, D-PANTHENOL, POLYQUATERNIUM-10, LEMON PEEL EXTRACT PROTEIN & VITAMIN SHAMPOO SUN FLOWER SEED OIL, -

(12) Patent Application Publication (10) Pub. No.: US 2013/0034530 A1 Fantz (43) Pub
US 2013 0034530A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0034530 A1 Fantz (43) Pub. Date: Feb. 7, 2013 (54) DIETARY SUPPLEMENT COGNITIVE (52) U.S. Cl. ....................................... 424/94.2; 424/643 SUPPORT SYSTEM (57) ABSTRACT (75) Inventor: David Robert Fantz, Denver, CO (US) The present invention relates to a nutritional Supplement composition, comprising a therapeutically effective amounts of Vitamin C, Vitamin D3. Thiamin, Riboflavin, Niacin, Vita (73) Assignee: David R. Fantz, Denver, CO (US) min B6, Folic acid, Vitamin B12, Pantothenic acid, Calcium, Magnesium, Zinc, Chromium, Sugar, Protein, Acetyl-L-Car (21) Appl. No.: 13/456,287 nitine, Dimethylaminoethanol complex, Phosphatidylserine complex, L-Glutamine, N-Acetyl-L-Tyrosine, L-Phenylala nine, Taurine, Methionine, Valine, Isoleucine, 5 Hydrox (22) Filed: Apr. 26, 2012 ytryptophan, L-Taurine, N-Acetyl-Tyrosine, N-Acetyl-L- Cysteine, Alpha Lipoic Acid, Alpha Related U.S. Application Data Glycerylphosphoricholine complex, Bacopa Monnieri extract, Gingko Biloba extract, Passion flower, Lemon Balm, (60) Provisional application No. 61/480.372, filed on Apr. Gotu Kola, Ashwagandha, Choline Bitartrate complex, Panax 29, 2011. Ginseng extract, Turmeric, Organic freeze dried fruit juice blends (concord grape, red raspberry, pineapple, cranberry, Publication Classification acai, pomegranate, acerola cherry, bilberry, lingonberry, black currant, aronia, Sour cherry, black raspberry), Organic (51) Int. Cl. freeze dried greens blends (barley grass, broccoli, beet, car A6 IK33/30 (2006.01) rot, alfalfa, oat), and Protein digestive enzyme blends (Pro A6IP3/02 (2006.01) tease 4.5, peptidase, bromelain, protease 6.0, protease 3.0, L A6IP 25/00 (2006.01) planatrum, B bifidum) in a mixture to provide optimal cog A6 IK38/54 (2006.01) nitive function. -

(12) Patent Application Publication (10) Pub. No.: US 2006/0110449 A1 Lorber Et Al
US 200601 10449A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0110449 A1 LOrber et al. (43) Pub. Date: May 25, 2006 (54) PHARMACEUTICAL COMPOSITION Publication Classification (76) Inventors: Richard R. Lorber, Scotch Plains, NJ (US); Heribert W. Staudinger, Union, (51) Int. Cl. NJ (US); Robert E. Ward, Summit, NJ A6II 3/473 (2006.01) (US) A6II 3L/24 (2006.01) Correspondence Address: A6IR 9/20 (2006.01) SCHERING-PLOUGH CORPORATION (52) U.S. Cl. ........................... 424/464; 514/290: 514/540 PATENT DEPARTMENT (K-6-1, 1990) 2000 GALLOPNG HILL ROAD KENILWORTH, NJ 07033-0530 (US) (57) ABSTRACT (21) Appl. No.: 11/257,348 (22) Filed: Oct. 24, 2005 The present invention relates to formulations useful for Related U.S. Application Data treating respiratory disorders associated with the production of mucus glycoprotein, skin disorders, and allergic conjunc (60) Provisional application No. 60/622,507, filed on Oct. tivitis while substantially reducing adverse effects associ 27, 2004. Provisional application No. 60/621,783, ated with the administration of non-selective anti-cholin filed on Oct. 25, 2004. ergic agents and methods of use thereof. US 2006/01 10449 A1 May 25, 2006 PHARMACEUTICAL COMPOSITION example, Weinstein and Weinstein (U.S. Pat. No. 6,086,914) describe methods of treating allergic rhinitis using an anti CROSS REFERENCE TO RELATED cholinergic agent with a limited capacity to pass across lipid APPLICATION membranes, such as the blood-brain barrier, in combination with an antihistamine that is limited in both sedating and 0001. This application claims benefit of priority to U.S. -

An Overview of Biosynthesis Pathways – Inspiration for Pharmaceutical and Agrochemical Discovery
An Overview of Biosynthesis Pathways – Inspiration for Pharmaceutical and Agrochemical Discovery Alan C. Spivey [email protected] 19th Oct 2019 Lessons in Synthesis - Azadirachtin • Azadirachtin is a potent insect anti-feedant from the Indian neem tree: – exact biogenesis unknown but certainly via steroid modification: O MeO C OAc O 2 H O OH O H O OH 12 O O C 11 O 14 OH oxidative 8 O H 7 cleavage highly hindered C-C bond HO OH AcO OH AcO OH for synthesis! H H of C ring H MeO2C O AcO H tirucallol azadirachtanin A azadirachtin (cf. lanosterol) (a limanoid = tetra-nor-triterpenoid) – Intense synhtetic efforts by the groups of Nicolaou, Watanabe, Ley and others since structural elucidation in 1987. –1st total synthesis achieved in 2007 by Ley following 22 yrs of effort – ~40 researchers and over 100 person-years of research! – 64-step synthesis – Veitch Angew. Chem. Int. Ed. 2007, 46, 7629 (DOI) & Veitch Angew. Chem. Int. Ed. 2007, 46, 7633 (DOI) – Review ‘The azadirachtin story’ see: Veitch Angew. Chem. Int. Ed. 2008, 47, 9402 (DOI) Format & Scope of Presentation • Metabolism & Biosynthesis – some definitions, 1° & 2° metabolites • Shikimate Metabolites – photosynthesis & glycolysis → shikimate formation → shikimate metabolites – Glyphosate – a non-selective herbicide • Alkaloids – acetylCoA & the citric acid cycle → -amino acids → alkaloids – Opioids – powerful pain killers • Fatty Acids and Polyketides –acetylCoA → malonylCoA → fatty acids, prostaglandins, polyketides, macrolide antibiotics – NSAIDs – anti-inflammatory’s • Isoprenoids/terpenes -

Optimal Foods
Optimal Foods 1. Almonds: high in monounsaturated and polyunsaturated fats, with 20% of calories coming from protein and dietary fiber. Nutrients include potassium, magnesium, calcium, iron, zinc, vitamin E and an antioxidant flavonoid called amygdlin also known as laetrile. 2. Barley: Like oat bran it is high in beta-glucan fiber which helps to lower cholesterol. Nutrients include copper, magnesium, phosphorous and niacin. 3. Berries : The darker the berry the higher in anti-oxidants. Nutritionally they are an excellent source of flavonoids, especially anthocyanidins, vitamin C and both soluble and insoluble fiber. 4. Brussels Sprouts : Similar to broccoli, and a member of the cabbage family, it contains cancer fighting glucosinolates. Nutritionally it is an excellent source of vitamin C and K, the B vitamins, beta-carotene, potassium and dietary fiber. 5. Carrots: It contains the highest source of proviatamin A carotenes as well as vitamin K, biotin, vitamin C, B6, potassium, thiamine and fiber. 6. Dark Chocolate: It is rich in the flavonoids, similar to those found in berries and apples, that are more easily absorbed than in other foods. It also provides an amino acid called arginine that helps blood vessels to dilate hence regulating blood flow and helping to lower blood pressure. Choose high-quality semisweet dark chocolate with the highest cocoa content that appeals to your taste buds. 7. Dark leafy greens : Kale, arugula, spinach, mustard greens, chard, collards, etc: low calorie, anti-oxidant dense food with carotenes, vitamin C, folic acid, manganese, copper, vitamin E, copper, vitamin B6, potassium, calcium, iron and dietary fiber. Kale is a particularly excellent bioavailable source of calcium while spinach is not. -

Spectator Anion Seems to Alter the Hazard Index Only Marginally. Significant Differences in Asthmagenicity Are Not Observed Betw
STATEMENT OF INTEREST TABLE 1 Hazard indices of common vitamin compounds None declared. Vitamin Molecular mass Da Hazard index REFERENCES All-trans retinoic acid (A) 300.44 0.9329 1 Retinyl palmitate (A) 524.88 0.9974 Sripaiboonkij P, Phanprasit W, Jaakkola MS. Respiratory beta-carotene (provitamin A) 536.89 0.9970 effects of occupational exposures in a milk powder factory. Eur Respir J 2008; 31: 807–814. Ergocalciferol (D2) 396.66 0.9432 2 Drought VJ, Francis HC, Niven RMcL, Burge PS., Cholecalciferol (D3) 384.65 0.9355 Tocopherol acetate (E) 472.76 0.9036 Occupational asthma induced by thiamine in a vitamin Naphthoquinone (K) 158.16 0.1600 supplement for breakfast cereals. Allergy 2005; 60: 1213–1214. 3 Jarvis J, Seed MJ, Elton R, Sawyer L, Agius R. Relationship Phylloquinone (K1) 116.16 0.1157 between chemical structure and the occupational asthma Menaquinone (K2) 168.15 0.2958 Menadione (Provitamin K) 172.19 0.2044 hazard of low molecular weight organic compounds. Occup Environ Med 2005; 62: 243–250. Thiamine (B1) 263.34 0.9400 4 Seed MJ, Agius RM. Prediction of asthma hazard of Thiamine hydrochloride (B1) 338.28 0.9469 thiamine. Allergy 2006; 61: 648. Thiamine mononitrate (B1) 329.38 0.9548 Riboflavin (B2) 376.37 0.9987 DOI: 10.1183/09031936.00065108 Niacin (B3) 123.11 0.9169 Pantothenic acid (B5) 219.24 0.9896 Pyridoxine (B ) 169.18 0.0963 6 From the authors: Pyridoxine hydrochloride (B6) 205.64 0.0948 Biotin (H/B7) 244.31 0.9631 We recently reported results of a cross-sectional study of 167 Folic acid (B9) 441.41 1.0000 milk powder factory workers and 76 office workers from # Cyanocobalamin (B12) 1355.37 Thailand showing that production and packing workers Ascorbic acid (C) 176.13 0.0196 exposed to relatively low concentrations of milk powder experienced significantly increased risk of nasal symptoms #: high molecular weight unsuitable for quantitative structural activity and breathlessness, had clearly increased risk of wheezing and relationship model. -

The Biosynthetic Gene Cluster for the Anticancer Drug Bleomycin From
Journal of Industrial Microbiology & Biotechnology (2001) 27, 378–385 D 2001 Nature Publishing Group 1367-5435/01 $17.00 www.nature.com/jim The biosynthetic gene cluster for the anticancer drug bleomycin from Streptomyces verticillus ATCC15003 as a model for hybrid peptide–polyketide natural product biosynthesis B Shen, L Du, C Sanchez, DJ Edwards, M Chen and JM Murrell Department of Chemistry, University of California, Davis, One Shields Avenue, Davis, CA 95616, USA The hybrid peptide–polyketide backbone of bleomycin (BLM) is assembled by the BLM megasynthetase that consists of both nonribosomal peptide synthetase (NRPS) and polyketide synthase (PKS) modules. BlmIX/BlmVIII/BlmVII constitute a natural hybrid NRPS/PKS/NRPS system, serving as a model for both hybrid NRPS/PKS and PKS/NRPS systems. Sequence analysis and functional comparison of domains and modules of BlmIX/BlmVIII/BlmVII with those of nonhybrid NRPS and PKS systems suggest that (1) the same catalytic sites appear to be conserved in both hybrid NRPS–PKS and nonhybrid NRPS or PKS systems, with the exception of the KS domains in the hybrid NRPS/PKS systems that are unique; (2) specific interpolypeptide linkers may play a critical role in intermodular communication to facilitate transfer of the growing intermediates between the interacting NRPS and/or PKS modules; and (3) posttranslational modification of the BLM megasynthetase has been accomplished by a single PPTase with a broad substrate specificity toward the apo forms of both acyl carrier proteins (ACPs) and peptidyl carrier -

Toxicological and Pharmacological Profile of Amanita Muscaria (L.) Lam
Pharmacia 67(4): 317–323 DOI 10.3897/pharmacia.67.e56112 Review Article Toxicological and pharmacological profile of Amanita muscaria (L.) Lam. – a new rising opportunity for biomedicine Maria Voynova1, Aleksandar Shkondrov2, Magdalena Kondeva-Burdina1, Ilina Krasteva2 1 Laboratory of Drug metabolism and drug toxicity, Department “Pharmacology, Pharmacotherapy and Toxicology”, Faculty of Pharmacy, Medical University of Sofia, Bulgaria 2 Department of Pharmacognosy, Faculty of Pharmacy, Medical University of Sofia, Bulgaria Corresponding author: Magdalena Kondeva-Burdina ([email protected]) Received 2 July 2020 ♦ Accepted 19 August 2020 ♦ Published 26 November 2020 Citation: Voynova M, Shkondrov A, Kondeva-Burdina M, Krasteva I (2020) Toxicological and pharmacological profile of Amanita muscaria (L.) Lam. – a new rising opportunity for biomedicine. Pharmacia 67(4): 317–323. https://doi.org/10.3897/pharmacia.67. e56112 Abstract Amanita muscaria, commonly known as fly agaric, is a basidiomycete. Its main psychoactive constituents are ibotenic acid and mus- cimol, both involved in ‘pantherina-muscaria’ poisoning syndrome. The rising pharmacological and toxicological interest based on lots of contradictive opinions concerning the use of Amanita muscaria extracts’ neuroprotective role against some neurodegenerative diseases such as Parkinson’s and Alzheimer’s, its potent role in the treatment of cerebral ischaemia and other socially significant health conditions gave the basis for this review. Facts about Amanita muscaria’s morphology, chemical content, toxicological and pharmacological characteristics and usage from ancient times to present-day’s opportunities in modern medicine are presented. Keywords Amanita muscaria, muscimol, ibotenic acid Introduction rica, the genus had an ancestral origin in the Siberian-Be- ringian region in the Tertiary period (Geml et al. -

The Effect of Vitamin Supplementation on Subclinical
molecules Review The Effect of Vitamin Supplementation on Subclinical Atherosclerosis in Patients without Manifest Cardiovascular Diseases: Never-ending Hope or Underestimated Effect? Ovidiu Mitu 1,2,* , Ioana Alexandra Cirneala 1,*, Andrada Ioana Lupsan 3, Mircea Iurciuc 4 , 5 5 2, Ivona Mitu , Daniela Cristina Dimitriu , Alexandru Dan Costache y , Antoniu Octavian Petris 1,2 and Irina Iuliana Costache 1,2 1 Department of Cardiology, Clinical Emergency Hospital “Sf. Spiridon”, 700111 Iasi, Romania 2 1st Medical Department, University of Medicine and Pharmacy “Grigore T. Popa”, 700115 Iasi, Romania 3 Department of Cardiology, University of Medicine, Pharmacy, Science and Technology, 540139 Targu Mures, Romania 4 Department of Cardiology, University of Medicine and Pharmacy “Victor Babes”, 300041 Timisoara, Romania 5 2nd Morpho-Functional Department, University of Medicine and Pharmacy “Grigore T. Popa”, 700115 Iasi, Romania * Correspondence: [email protected] (O.M.); [email protected] (I.A.C.); Tel.: +40-745-279-714 (O.M.) Medical Student, University of Medicine and Pharmacy “Grigore T. Popa”, 700115 Iasi, Romania. y Academic Editors: Raluca Maria Pop, Ada Popolo and Stefan Cristian Vesa Received: 25 March 2020; Accepted: 7 April 2020; Published: 9 April 2020 Abstract: Micronutrients, especially vitamins, play an important role in the evolution of cardiovascular diseases (CVD). It has been speculated that additional intake of vitamins may reduce the CVD burden by acting on the inflammatory and oxidative response starting from early stages of atherosclerosis, when the vascular impairment might still be reversible or, at least, slowed down. The current review assesses the role of major vitamins on subclinical atherosclerosis process and the potential clinical implications in patients without CVD. -

Vitamin and Mineral Requirements in Human Nutrition
P000i-00xx 3/12/05 8:54 PM Page i Vitamin and mineral requirements in human nutrition Second edition VITPR 3/12/05 16:50 Page ii WHO Library Cataloguing-in-Publication Data Joint FAO/WHO Expert Consultation on Human Vitamin and Mineral Requirements (1998 : Bangkok, Thailand). Vitamin and mineral requirements in human nutrition : report of a joint FAO/WHO expert consultation, Bangkok, Thailand, 21–30 September 1998. 1.Vitamins — standards 2.Micronutrients — standards 3.Trace elements — standards 4.Deficiency diseases — diet therapy 5.Nutritional requirements I.Title. ISBN 92 4 154612 3 (LC/NLM Classification: QU 145) © World Health Organization and Food and Agriculture Organization of the United Nations 2004 All rights reserved. Publications of the World Health Organization can be obtained from Market- ing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permis- sion to reproduce or translate WHO publications — whether for sale or for noncommercial distri- bution — should be addressed to Publications, at the above address (fax: +41 22 791 4806; e-mail: [email protected]), or to Chief, Publishing and Multimedia Service, Information Division, Food and Agriculture Organization of the United Nations, 00100 Rome, Italy. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization and the Food and Agriculture Organization of the United Nations concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -
A Computational Approach for Identifying Plant-Based Foods for Addressing Vitamin Deficiency Diseases
University of Vermont ScholarWorks @ UVM UVM Honors College Senior Theses Undergraduate Theses 2015 A Computational Approach for Identifying Plant-Based Foods for Addressing Vitamin Deficiency Diseases Christina Yu University of Vermont Indra Neil Sarkar University of Vermont Follow this and additional works at: https://scholarworks.uvm.edu/hcoltheses Recommended Citation Yu, Christina and Sarkar, Indra Neil, "A Computational Approach for Identifying Plant-Based Foods for Addressing Vitamin Deficiency Diseases" (2015). UVM Honors College Senior Theses. 212. https://scholarworks.uvm.edu/hcoltheses/212 This Honors College Thesis is brought to you for free and open access by the Undergraduate Theses at ScholarWorks @ UVM. It has been accepted for inclusion in UVM Honors College Senior Theses by an authorized administrator of ScholarWorks @ UVM. For more information, please contact [email protected]. A Computational Approach for Identifying Plant-Based Foods for Addressing Vitamin Deficiency Diseases Christina Yu1 and Indra Neil Sarkar2,3 Key words: computing methodologies, vitamin deficiency diseases, vegetarian diet 1 Undergraduate Program in Biochemistry, University of Vermont, Burlington, VT 2 Department of Microbiology and Molecular Genetics, University of Vermont, Burlington, VT 3 Center for Clinical and Translational Science, University of Vermont, Burlington, VT 1 ABSTRACT Vitamins are nutrients that are essential to human health, and deficiencies have been shown to cause severe diseases. In this study, a computational approach was used to identify vitamin deficiency diseases and plant-based foods with vitamin content. Data from the United States Department of Agriculture Standard Reference (SR27), National Library of Medicine's Medical Subject Headings and MEDLINE, and Wikipedia were combined to identify vitamin deficiency diseases and vitamin content of plant-based foods. -

Vitamins a and E and Carotenoids
Fat-Soluble Vitamins & Micronutrients: Vitamins A and E and Carotenoids Vitamins A (retinol) and E (tocopherol) and the carotenoids are fat-soluble micronutrients that are found in many foods, including some vegetables, fruits, meats, and animal products. Fish-liver oils, liver, egg yolks, butter, and cream are known for their higher content of vitamin A. Nuts and seeds are particularly rich sources of vitamin E (Thomas 2006). At least 700 carotenoids—fat-soluble red and yellow pigments—are found in nature (Britton 2004). Americans consume 40–50 of these carotenoids, primarily in fruits and vegetables (Khachik 1992), and smaller amounts in poultry products, including egg yolks, and in seafoods (Boylston 2007). Six major carotenoids are found in human serum: alpha-carotene, beta-carotene, beta-cryptoxanthin, lutein, trans-lycopene, and zeaxanthin. Major carotene sources are orange-colored fruits and vegetables such as carrots, pumpkins, and mangos. Lutein and zeaxanthin are also found in dark green leafy vegetables, where any orange coloring is overshadowed by chlorophyll. Trans-Lycopene is obtained primarily from tomato and tomato products. For information on the carotenoid content of U.S. foods, see the 1998 carotenoid database created by the U.S. Department of Agriculture and the Nutrition Coordinating Center at the University of Minnesota (http://www.nal.usda.gov/fnic/foodcomp/Data/car98/car98.html). Vitamin A, found in foods that come from animal sources, is called preformed vitamin A. Some carotenoids found in colorful fruits and vegetables are called provitamin A; they are metabolized in the body to vitamin A. Among the carotenoids, beta-carotene, a retinol dimer, has the most significant provitamin A activity.