Mature Placenta Reproductive System > Physiology > Physiology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Fetal Brain Vascularity Visualized by Conventional 2D and 3D Power
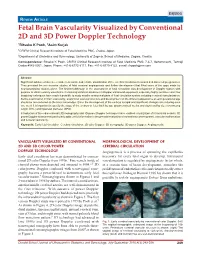
DSJUOG Fetal Brain Vascularity Visualized by Conventional 2D and 3D Power Doppler Technology REVIEW ARTICLE Fetal Brain Vascularity Visualized by Conventional 2D and 3D Power Doppler Technology 1Ritsuko K Pooh, 2Asim Kurjak 1CRIFM Clinical Research Institute of Fetal Medicine PMC, Osaka, Japan 2Department of Obstetrics and Gynecology, University of Zagreb, School of Medicine, Zagreb, Croatia Correspondence: Ritsuko K Pooh, CRIFM Clinical Research Institute of Fetal Medicine PMC 7-3-7, Uehommachi, Tennoji Osaka #543-0001, Japan, Phone: +81-6-6775-8111, Fax: +81-6-6775-8122, e-mail: [email protected] Abstract Significant advances have been made in accurate and reliable visualization of the cerebral circulation in normal and abnormal pregnancies. They provided the non-invasive studies of fetal cerebral angiogenesis and further development that filled some of the gaps made by neuroanatomical studies alone. The first breakthrough in the assessment of fetal circulation was development of Doppler system with purpose to obtain velocity waveforms. Continuing technical advances in Doppler ultrasound equipment, especially highly sensitive color flow imagining techniques have made it possible to study smaller anatomical parts of fetal circulation system including cerebral vascularization. Before examination of brain vascularity, anatomical vascular structure and development on the different appearance at each gestational age should be remembered as the basic knowledge. Since the development of the embryo is rapid and significant changes occur during even one week it is important to specify the stage of the embryo or fetus both by age (postmenstrual weeks and days) and by size (crownrump length (CRL) and biparietal diameter (BPD). Introduction of three-dimensional (3D) sonography and 3D power Doppler techniques have enabled visualization of intracranial vessels. -

Defective Decidualization During and After Severe Preeclampsia Reveals a Possible Maternal Contribution to the Etiology
Defective decidualization during and after severe preeclampsia reveals a possible maternal contribution to the etiology Tamara Garrido-Gomeza,b,c,d, Francisco Dominguezb, Alicia Quiñonerob, Patricia Diaz-Gimenob, Mirhan Kapidzicc,d, Matthew Gormleyc,d, Katherine Onac,d, Pablo Padilla-Isertee, Michael McMasterf, Olga Genbacevc,d, Alfredo Peralese,g, Susan J. Fisherc,d,h,i,1,2, and Carlos Simóna,b,g,j,1,2 aFundación Igenomix, 46980 Valencia, Spain; bInstituto Universitario IVI, Instituto de Investigación Sanitaria Hospital Clinico de Valencia INCLIVA, 46010 Valencia, Spain; cCenter for Reproductive Sciences, University of California, San Francisco, CA 94143; dDepartment of Obstetrics, Gynecology, and Reproductive Sciences, University of California, San Francisco, CA 94143; eDepartment of Obstetrics and Gynecology, Hospital Universitario La Fe, 46026 Valencia, Spain; fDepartment of Cell and Tissue Biology, University of California, San Francisco, CA 94143; gDepartment of Obstetrics and Gynecology, School of Medicine, Valencia University, 46010 Valencia, Spain; hThe Eli & Edythe Broad Center for Regeneration Medicine and Stem Cell Research, University of California, San Francisco, CA 94143; iDepartment of Anatomy, University of California, San Francisco, CA 94143; and jDepartment of Obstetrics and Gynecology, School of Medicine, Stanford University, Palo Alto, CA 94305 Edited by R. Michael Roberts, University of Missouri-Columbia, Columbia, MO, and approved August 11, 2017 (received for review April 20, 2017) In preeclampsia (PE), cytotrophoblast (CTB) invasion of the uterus in studying the CTB subpopulation that invades the uterine wall in and spiral arteries is often shallow. Thus, the placenta’s role has the context of this syndrome. Targeted analyses of particular mo- been a focus. In this study, we tested the hypothesis that decidual lecular families, such as the vascular-type adhesion molecules that defects are an important determinant of the placental phenotype. -

Decidua Produces a Protein That Inhibits Choriogonadotrophin Release from Human Trophoblasts
Decidua produces a protein that inhibits choriogonadotrophin release from human trophoblasts. S G Ren, G D Braunstein J Clin Invest. 1991;87(1):326-330. https://doi.org/10.1172/JCI114990. Research Article To test the hypothesis that uterine decidua may modulate trophoblast function, trophoblasts and decidual cells were isolated from term placentas by enzymatic digestion and Percoll gradient centrifugation. Placental trophoblasts were cocultured with decidual cells and trophoblasts or JEG-3 choriocarcinoma cells were incubated with medium conditioned by decidual cells (DCM) for 72-96 h. In cocultures decidual cells inhibited choriogonadotropin (hCG) release from trophoblasts by 75% in comparison with controls (P less than 0.001). The DCM contained a factor that markedly inhibited hCG release from trophoblasts and JEG cells in vitro compared with controls. The inhibitory effect of the factor on hCG release was dose dependent, and could be eliminated by boiling the DCM for 30 min or proteolytic enzyme treatment. Ultrafiltration and Sephadex G-50 fractionation of the DCM indicated that the apparent molecular mass was 7,000-10,000 D. DCM also inhibited the stimulatory effect of exogenous cAMP on hCG secretion by JEG-3 cells, suggesting that DCM may interfere with activation of the cAMP-dependent protein kinases or transcription of hCG genes. These results suggest that the release of trophoblast hCG is under local paracrine control, regulated in part by a protein released by decidual cells. Find the latest version: https://jci.me/114990/pdf Decidua Produces a Protein that Inhibits Choriogonadotrophin Release from Human Trophoblasts Song-Guang Ren and Glenn D. -

Development of Right Ventricle
DEVELOPMENT OF THE HEART II. David Lendvai M.D., Ph.D. Mark Kozsurek, M.D., Ph.D. • Septation of the common atrioventricular (AV) orifice. • Formation of the interatrial septum. • Formation of the muscular interventricular septum. • Appearance of the membranous interventricular septum and the spiral aorticopulmonary septum. right left septum primum septum primum septum primum septum primum septum primum septum primum foramen primum foramen primum septum primum septum primum foramen primum foramen primum septum primum septum primum foramen secundum foramen secundum foramen primum foramen primum septum primum foramen secundum septum primum foramen secundum foramen primum foramen primum septum primum septum primum foramen secundum foramen secundum septum secundum septum secundum foramen secundum foramen ovale foramen ovale septum primum septum primum septum secundum septum secundum foramen secundum foramen ovale foramen ovale septum primum septum primum septum secundum septum secundum foramen secundum septum primum foramen ovale foramen ovale septum primum SUMMARY • The septation of the common atrium starts with the appearance of the crescent-shaped septum primum. The opening of this septum, the foramen primum, becomes progressively smaller. • Before the foramen primum completly closes, postero-superiorly several small openings appear on the septum primum. These perforations coalesce later and form the foramen secundum. • On the right side of the septum primum a new septum, the septum secundum, starts to grow. The orifice of the septum secundum is the foramen ovale. • Finally two crescent-like, incomplete, partially overlapping septa exist with one hole on each. Septum secundum is more rigid and the septum primum on its left side acts as a valve letting the blood flow exclusively from the right to the left. -

Fetal Circulation
The Fetal Circulation Dr. S. Mathieu, Specialist Registrar in Anaesthesia Dr. D. J. Dalgleish, Consultant Anaesthetist Royal Bournemouth and Christchurch Hospitals Trust, UK Questions 1. In the fetal circulation: a) There are two umbilical arteries and one umbilical vein? b) Over 90% of blood passes the liver via the ductus venosus c) The foramen ovale divides the left and right ventricle d) The umbilical artery carries oxygenated blood from the placenta to the fetus e) The foramen ovale allows oxygenated blood to bypass the pulmonary circulation 2. In the fetal circulation: a) The oxygen dissociation curve of fetal haemoglobin is shifted to the left compared with adult haemoglobin ensuring oxygen delivery to the fetus despite low oxygen partial pressures b) It is the presence of the ductus arteriosus and large pulmonary vascular resistance which ensures most of the right ventricular output passes into the aorta c) The patency of the ductus arteriosus is maintained by high oxygen tensions d) The patency of the ductus arteriosus is maintained by the vasodilating effects of prostaglandin G2 e) 2,3-DPG levels are higher in fetal haemoglobin compared with adult haemaglobin 3. Changes at birth include: a) a fall in pulmonary vascular resistance b) a rise in systemic vascular resistance with clamping of the cord c) an increase in hypoxic pulmonary vasoconstriction d) a rise in left atrial pressure e) closure of the ductus arteriosus within 24 hours 4. The following congenital heart lesions are cyanotic: a) Ventricular septal defect b) Atrial septal defect c) Patent ductus arteriosus d) Tetralogy of Fallot e) Transposition of the great arteries MCQ answers at end Key points • The fetal circulation supplies the fetal tissues with oxygen and nutrients from the placenta. -
The Levels of Angiogenic and Anti-Angiogenic Molecule Concentrations in Pregnancy Based Disorders in the Maternal and Fetal Circ
Master of Philosophy THE LEVELS OF ANGIOGENIC AND ANTI-ANGIOGENIC MOLECULE CONCENTRATIONS IN PREGNANCY BASED DISORDERS IN THE MATERNAL AND FETAL CIRCULATION Islam Afzal Supervisor: Professor Asif Ahmed Department of Reproductive and Vascular Biology November 2012 University of Birmingham Research Archive e-theses repository This unpublished thesis/dissertation is copyright of the author and/or third parties. The intellectual property rights of the author or third parties in respect of this work are as defined by The Copyright Designs and Patents Act 1988 or as modified by any successor legislation. Any use made of information contained in this thesis/dissertation must be in accordance with that legislation and must be properly acknowledged. Further distribution or reproduction in any format is prohibited without the permission of the copyright holder. Islam Afzal Contents Table of Figures ............................................................................................... 5 Abbreviations ................................................................................................... 7 Acknowledgements .......................................................................................... 9 Abstract .......................................................................................................... 10 Introduction .................................................................................................... 11 Preeclampsia ................................................................................................ -

MA 5.4 NUMA SI GA RBHAVIKA S KRAM Completed Fetus in Prsava- Vastha Rasanufj*^SIK GARBHAVRUDHI
MA 5.4 NUMA SI GA RBHAVIKA S KRAM Completed Fetus in prsava- vastha rASANUfJ*^SIK GARBHAVRUDHI I N Ayurvedic classics, the embryonit*««,^jie.uaJf6f'ment has been narrated monthwise while the modern Medical literature has considered the development of embryo in months as well as in weeks. "KALALAV/ASTHA (first month) ^ T ^.?1T. 3/14 Susruta and both Vagbhattas us.ed the word 'K a la la ' forthe shape of the embryo in the first month of intrauterine life. I Caraka has described the first month embryo as a mass ofcells like mucoid character in which all body parts though present are not conspicuous. T Incorporated within it all the five basic elements, ' Panchmah'abhuta' i.e. Pruthvi, Ap , Teja, Vayu and Akas . During the first month the organs of Embryo are both manifested and latent. It is from this stage of Embryo that various organs of the fetus develop, thus they are menifested. But these organs are not well menifested for differentiation and recongnisiation hence they are simultenously described as latent as well as manifested. 3T.f.^. 1/37 Astang - hrudayakar has described the embryo of first month as 'Kalala' but in 'avyakta' form. The organs of an embryo is in indistingushed form. Modern embryologist has described this first month development in week divisions. First Week - No fertile ova of the first week has been examined. Our knowledge of the first week of I embryo is of other mammals as amphibian. The egg is fertilised in the upper end of the uterine tube, and segments into about cells, before it I passes in to the uterus, it continues to segment and develop into a blastocyst (Budbuda) with a trophoblastic cells and inner cell mass. -

Cardiovascular System Note: the Cardiovascular System Develops Early (Week 3), Enabling the Embryo to Grow Beyond the Short
Lymphatics: Lymph vessel formation is similar to blood angiogenesis. Lymphatics begin as lymph sacs in three regions: jugular (near brachiocephalic veins); cranial abdominal (future cysterna chyla); and iliac region. Lym- phatic vessels (ducts) form as outgrowths of the sacs. mesenchyme Lymph nodes are produced by localized mesoder- sinusoid lymph duct lumen mal invaginations that partition the vessel lumen into sinu- soids. The mesoderm develops a reticular framework within which mesodermal lymphocytes accumulate. The spleen and hemal nodes (in ruminants) invagination develop similar to the way lymph nodes develop. Lymph Node Formation Prior to birth, fetal circulation is designed for an in utero aqueous environment where the pla- centa oxygenates fetal blood. Suddenly, at birth... Three In-Utero Adjustments ductus Stretching and constriction of arteriosus umbilical arteries shifts fetal blood flow aortic arch from the placenta to the fetus. Reduced pulmonary trunk L atrium venous return through the (left) umbili- foramen ovale R cal vein and ductus venosus allows the atrium latter to gradually close (over a period caudal vena cava of days). Bradykinin released by expand- ductus venosus ing lungs and increased oxygen concen- tration in blood triggers constriction of aorta the ductus arteriosus which, over two liver months, is gradually converted to a fibrous structure, the ligamentum arte- umbilical v. riosum. portal v. The increased blood flow to the lungs and then to the left atrium equalizes pres- sure in the two atria, resulting in closure umbilical aa. of the foramen ovale that eventually grows permanent. 29 The cardiogenic area, the place where the embryonic heart originates, is located . -

Equine Placenta – Marvelous Organ and a Lethal Weapon
Equine placenta – marvelous organ and a lethal weapon Malgorzata Pozor, DVM, PhD, Diplomate ACT Introduction Placenta has been defined as: „an apposition between parent (usually maternal) and fetal tissue in order to establish physiological exchange” (1). Another definition of this important organ was proposed by Steven and Morris: „a device consisting of one or more transport epithelia located between fetal and maternal blood supply” (2). The main function of placenta is to provide an interface between the dam and the the fetus and to allow the metabolic exchange of the the nutrients, oxygen and waste material. The maternal circulation is brought into a close apposition to the fetal circulation, while a separation of these two circulatory systems remain separated (3). A degree and complexity of this „intimate relationship” varies greately between species mostly due to the structural diversity of the extraembryonic membranes of the vertebrates. The early feto-maternal exchange in the equine pregnancy is established as early as on day 22 after fertilization. The fetal and choriovitellin circulations are already present, the capsule ruptures and the allantois is already visible (4). The allantois starts expanding by day 32 and vascularizes approximately 90% of the chorion and fuses with it to form chorioallantois by day 38 of gestation (5). The equine placenta continues increasing its complexity till approximately day 150 of gestation. Equids have epitheliochorial placenta, there are six leyers separating maternal and fetal circulation, and there are no erosion of the luminal, maternal epithelium, like in ruminants (6). Thousands of small chorionic microvilli develop and penetrate into endometrial invaginations. -

4 Extraembryonic Membranes
Implantation, Extraembryonic Membranes, Placental Structure and Classification A t t a c h m e n t and Implantation Implantation is the first stage in development of the placenta. In most cases, implantation is preceded by a close interaction of embryonic trophoblast and endometrial epithelial cells that is known as adhesion or attachment. Implantation also is known as the stage where the blastocyst embeds itself in the endometrium, the inner membrane of the uterus. This usually occurs near the top of the uterus and on the posterior wall. Among other things, attachment involves a tight intertwining of microvilli on the maternal and embryonic cells. Following attachment, the blastocyst is no longer easily flushed from the lumen of the uterus. In species that carry multiple offspring, attachment is preceeded by a remarkably even spacing of embryos through the uterus. This process appears to result from uterine contractions and in some cases involves migration of embryos from one uterine horn to another (transuterine migration). The effect of implantation in all cases is to obtain very close apposition between embryonic and maternal tissues. There are, however, substantial differences among species in the process of implantation, particularly with regard to "invasiveness," or how much the embryo erodes into maternal tissue. In species like horses and pigs, attachment and implantation are essentially equivalent. In contrast, implantation in humans involves the embryo eroding deeply into the substance of the uterus. •Centric: the embryo expands to a large size before implantation, then remains in the center of the uterus. Examples include carnivores, ruminants, horses, and pigs. •Eccentric: The blastocyst is small and implants within the endometrium on the side of the uterus, usually opposite to the mesometrium. -

From Trophoblast to Human Placenta
From Trophoblast to Human Placenta (from The Encyclopedia of Reproduction) Harvey J. Kliman, M.D., Ph.D. Yale University School of Medicine I. Introduction II. Formation of the placenta III. Structure and function of the placenta IV. Complications of pregnancy related to trophoblasts and the placenta Glossary amnion the inner layer of the external membranes in direct contact with the amnionic fluid. chorion the outer layer of the external membranes composed of trophoblasts and extracellular matrix in direct contact with the uterus. chorionic plate the connective tissue that separates the amnionic fluid from the maternal blood on the fetal surface of the placenta. chorionic villous the final ramification of the fetal circulation within the placenta. cytotrophoblast a mononuclear cell which is the precursor cell of all other trophoblasts. decidua the transformed endometrium of pregnancy intervillous space the space in between the chorionic villi where the maternal blood circulates within the placenta invasive trophoblast the population of trophoblasts that leave the placenta, infiltrates the endo– and myometrium and penetrates the maternal spiral arteries, transforming them into low capacitance blood channels. Sunday, October 29, 2006 Page 1 of 19 From Trophoblasts to Human Placenta Harvey Kliman junctional trophoblast the specialized trophoblast that keep the placenta and external membranes attached to the uterus. spiral arteries the maternal arteries that travel through the myo– and endometrium which deliver blood to the placenta. syncytiotrophoblast the multinucleated trophoblast that forms the outer layer of the chorionic villi responsible for nutrient exchange and hormone production. I. Introduction The precursor cells of the human placenta—the trophoblasts—first appear four days after fertilization as the outer layer of cells of the blastocyst. -

Abundant Expression of Parathyroid Hormone-Related Protein in Human Amnion and Its Association with Labor (Pregnancy/Myometrium/Decidua/Placenta/Amniotic Fluid) J
Proc. Nati. Acad. Sci. USA Vol. 89, pp. 8384-8388, September 1992 Physiology Abundant expression of parathyroid hormone-related protein in human amnion and its association with labor (pregnancy/myometrium/decidua/placenta/amniotic fluid) J. E. FERGUSON II*, JANET V. GORMAN*, DAVID E. BRUNS*, ELEANOR C. WEIRt, WILLIAM J. BURTISt, T. J. MARTINt, AND M. ELIZABETH BRUNS*§ *Departments of Obstetrics & Gynecology and Pathology, University of Virginia Medical School, Charlottesville, VA 22908; tDepartments of Medicine and Comparative Medicine, Yale University Medical School, New Haven, CT 06510; and tDepartment of Medicine, University of Melbourne, Melbourne 3065 Australia Communicated by Robert H. Wasserman, June 1, 1992 (receivedfor review December 12, 1991) ABSTRACT In animal models, parathyroid hormone- and reaches a peak 48 hr prior to parturition (4). A peak in related protein (PTHrP) increases placental calcium transport peptide content has also been demonstrated by biological and and inhibits contraction ofuterine smooth muscle. The present immunological assays. As PTHrP and PTH have been shown studies were undertaken to characterize the expression of to be vasodilators and to relax smooth muscles, including PTHrP in human uteroplacental tissues. PTHrP mRNA was uterine smooth muscle (7-9), PTHrP may play a role in (i) identified by Northern analysis as a single species (:1.8 vasodilation in the uteroplacental unit, (ii) expansion of the kilobases) in human amnion, chorion, placenta, decidua, and uterus to accommodate fetal growth, (iii) maintenance ofthe myometrium. The most abundant signal was seen in amnion, pregnant uterus in a quiescent, relaxed state prior to the onset where it was 10-400 times that in the other uteroplacental of labor, and/or (iv) relaxation of the uterine cervix to allow tissues.