Role of Islet Endothelial Cells in Β-Cell Function and Growth
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Ins and Outs of Circadian Timekeeping Steven a Brown* and Ueli Schibler†
gd9507.qxd 11/10/1999 12:14 PM Page 588 588 The ins and outs of circadian timekeeping Steven A Brown* and Ueli Schibler† Recent research in Drosophila and in mammals has generated The mechanism by which light signals entrain the clock is fascinating new models for how circadian clocks in these another topic of intense interest, and will be our other focus. organisms are reset by light and how these clocks, in turn, direct circadian outputs. Though light perception by the central clock is Central clock mechanisms: a brief summary ocular in mammals, it probably proceeds via a mechanism In all cases examined to date, circadian clocks have been separate from traditional visual transduction. In Drosophila, one cell-autonomous: a single cell can generate and maintain mechanism is non-ocular and is in fact present in many different self-sustained circadian oscillations. The molecular basis tissues. In both organisms, the cryptochrome family of for these rhythms may rely on a negative feedback loop in photoreceptor-like molecules plays a role in the circadian clock, which clock proteins negatively regulate their own abun- though their function is incompletely understood. Moreover, dance or activity. This regulation may occur both at the although a master clock resides in the brain, a functional clock transcriptional and at the post-transcriptional level. For appears to reside in most cells of the body. In these tissues, at example, in the bread mold Neurospora crassa, the Fre- least some output genes are controlled at the transcriptional quency protein negatively regulates its own transcription level directly by clock proteins; others appear to be regulated by by interfering with the ability of the White-collar-1 and cascades of circadian transcription factors. -
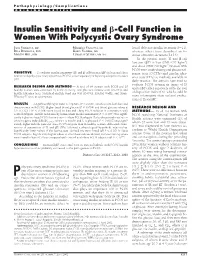
Insulin Sensitivity and ß-Cell Function in Women with Polycystic Ovary
Pathophysiology/Complications ORIGINAL ARTICLE Insulin Sensitivity and -Cell Function in Women With Polycystic Ovary Syndrome JANA VRB´IKOVA´, MD MARKETA´ VANKOVA´, MS found defective insulin secretion (9–11), BELA BENDLOVA´, PHD KAREL VONDRA, MD whereas others have described an in- MARTIN HILL, PHD LUBOSLAV STARKA´ , MD, DSC crease of insulin secretion (12,13). In the present study, IS and -cell function (F) in lean (BMI Ͻ27 kg/m2) and obese (BMI Ն27 kg/m2) women with PCOS were studied using oral glucose tol-   OBJECTIVE — To evaluate insulin sensitivity (IS) and -cell function ( F) in lean and obese erance tests (OGTTs) and insulin toler- women with polycystic ovary syndrome (PCOS), either separately or by using a disposition index ance tests (ITTs) as methods available in (DI). daily practice. The authors have tried to evaluate PCOS women in terms of IS RESEARCH DESIGN AND METHODS — A total of 64 women with PCOS and 20 and/or F either separately or by the tool healthy women were examined by anthropometry, oral glucose tolerance tests (OGTTs), and insulin tolerance tests. Statistical analysis used one-way ANOVA, Kruskal-Wallis, and Mann- of disposition index (DI), which could be Whitney U tests, as appropriate. more informative than isolated evalua- tions of IS and F. RESULTS — A significantly higher waist-to-hip ratio (P Ͻ 0.0001) was found in both lean and obese women with PCOS. Higher basal blood glucose (P Ͻ 0.004) and blood glucose values at RESEARCH DESIGN AND 3 h of OGTT (P Ͻ 0.008) were found in lean and obese PCOS subjects in comparison with METHODS — In all, 64 women with control subjects. -

Endocrine Cell Type Sorting and Mature Architecture in the Islets Of
www.nature.com/scientificreports OPEN Endocrine cell type sorting and mature architecture in the islets of Langerhans require expression of Received: 16 April 2018 Accepted: 4 July 2018 Roundabout receptors in β cells Published: xx xx xxxx Melissa T. Adams, Jennifer M. Gilbert, Jesus Hinojosa Paiz, Faith M. Bowman & Barak Blum Pancreatic islets of Langerhans display characteristic spatial architecture of their endocrine cell types. This architecture is critical for cell-cell communication and coordinated hormone secretion. Islet architecture is disrupted in type-2 diabetes. Moreover, the generation of architecturally correct islets in vitro remains a challenge in regenerative approaches to type-1 diabetes. Although the characteristic islet architecture is well documented, the mechanisms controlling its formation remain obscure. Here, we report that correct endocrine cell type sorting and the formation of mature islet architecture require the expression of Roundabout (Robo) receptors in β cells. Mice with whole-body deletion of Robo1 and conditional deletion of Robo2 either in all endocrine cells or selectively in β cells show complete loss of endocrine cell type sorting, highlighting the importance of β cells as the primary organizer of islet architecture. Conditional deletion of Robo in mature β cells subsequent to islet formation results in a similar phenotype. Finally, we provide evidence to suggest that the loss of islet architecture in Robo KO mice is not due to β cell transdiferentiation, cell death or loss of β cell diferentiation or maturation. Te islets of Langerhans display typical, species-specifc architecture, with distinct spatial organization of their various endocrine cell types1–5. In the mouse, the core of the islet is composed mostly of insulin-secreting β cells, while glucagon-secreting α cells, somatostatin-secreting δ cells and pancreatic polypeptide-secreting PP cells are located at the islet periphery3. -

The Role of Thyroid Hormone
Central Journal of Endocrinology, Diabetes & Obesity Mini Review Special Issue on Role of Thyroid Hormone Pancreatic and Islet Develop- in Metabolic Homeostasis ment and Function: The Role of *Corresponding authors Teresa L Mastracci, Department of Pediatrics, Indiana University School of Medicine, Herman B Wells Center for Thyroid Hormone Pediatric Research, 635 Barnhill Dr, MS2031, Indianapolis, IN, USA 46202, Tel: 317-278-8940; Fax: 317-274-4107; Teresa L Mastracci1,5* and Carmella Evans-Molina2,3,4,5* Email: 1Department of Pediatrics, Indiana University School of Medicine, USA Carmella Evans-Molina, Department of Medicine, 2Department of Medicine, Indiana University School of Medicine, USA Cellular and Integrative Physiology, Biochemistry and 3Department of Cellular and Integrative Physiology, Indiana University School of Molecular Biology, Herman B Wells Center for Pediatric Medicine, USA Research, Indiana University School of Medicine, 4Department of Biochemistry and Molecular Biology, Indiana University School of Indiana University School of Medicine, 635 Barnhill Dr., Medicine, USA MS2031, Indianapolis, IN, USA 46202, Tel: 317-278-3177; 5Herman B Wells Center for Pediatric Research, Indiana University School of Medicine, Fax: 317-274-4107; Email: USA Submitted: 12 June 2014 Accepted: 17 July 2014 Published: 19 July 2014 Abstract ISSN: 2333-6692 A gradually expanding body of literature suggests that Thyroid Hormone (TH) Copyright and Thyroid Hormone Receptors (TRs) play a contributing role in pancreatic and islet © 2014 Mastracci et al. cell development, maturation, and function. Studies using a variety of model systems capable of exploiting species-specific developmental paradigms have revealed the OPEN ACCESS contribution of TH to cellular differentiation, lineage decisions, and endocrine cell specification. -
![First Responder Cells Drive the First-Phase [Ca2+] Response](https://docslib.b-cdn.net/cover/3508/first-responder-cells-drive-the-first-phase-ca2-response-733508.webp)
First Responder Cells Drive the First-Phase [Ca2+] Response
bioRxiv preprint doi: https://doi.org/10.1101/2020.12.22.424082; this version posted December 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Functional architecture of the pancreatic islets: First responder cells drive the first-phase [Ca2+] response Vira Kravetsa,b, JaeAnn M. Dwuleta, Wolfgang E. Schleicherb, David J. Hodsonc, Anna M. Davis,a Robert A. Piscopiob, Maura Sticco-Ivins,b Richard K.P. Benningera,b,1. a Department of Bioengineering, University of Colorado, Anschutz Medical campus, Aurora, CO. USA b Barbara Davis center for childhood diabetes, University of Colorado, Anschutz Medical campus, Aurora, CO. USA c Institute of Metabolism and Systems Research, University of Birmingham, Birmingham. UK, and Centre for Endocrinology, Diabetes and Metabolism, Birmingham Health Partners, Birmingham, UK 1 To whom correspondence should be addressed: [email protected] Tel: (303) 724-6388. Fax: (303) 724-5800. 1775 Aurora court, M20-4306D, mailstop B140, University of Colorado Anschutz Medical campus, Aurora, CO. 80045. Short title: First responder cells control islet function Keywords: Laser ablation; Multicellular Dynamics; Biological Networks; Optical Microscopy; Diabetes; Gap junctions. Manuscript word count (main text, excluding methods): 5311. Abstract word count: 294 bioRxiv preprint doi: https://doi.org/10.1101/2020.12.22.424082; this version posted December 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Abstract Insulin-secreting b-cells are functionally heterogeneous. Subpopulations of b-cells can control islet function and the regulation of hormone release, such as driving the second (oscillatory) phase of free-calcium ([Ca2+]) following glucose elevation. -

The Islet Ghrelin Cell 52:1 R35–R49 Review
N WIERUP and others The islet ghrelin cell 52:1 R35–R49 Review The islet ghrelin cell Nils Wierup, Frank Sundler and R Scott Heller1 Correspondence should be addressed Unit of Neuroendocrine Cell Biology, Department of Clinical Sciences in Malmo¨ , Lund University Diabetes Centre, to N Wierup Clinical Research Centre, Scania University Hospital, Jan Waldenstro¨ ms gata 35, SE 205 02 Malmo¨ , Sweden Email 1Imaging Team, Novo Nordisk A/S, Novo Nordisk Park, DK2760 Ma˚ løv, Denmark [email protected] Abstract The islets of Langerhans are key regulators of glucose homeostasis and have been known Key Words as a structure for almost one and a half centuries. During the twentieth century several " ghrelin different cell types were described in the islets of different species and at different " islet developmental stages. Six cell types with identified hormonal product have been described " ghrelin cell so far by the use of histochemical staining methods, transmission electron microscopy, " pancreas and immunohistochemistry. Thus, glucagon-producing a-cells, insulin-producing b-cells, " human somatostatin-producing d-cells, pancreatic polypeptide-producing PP-cells, serotonin- " rat producing enterochromaffin-cells, and gastrin-producing G-cells have all been found in the " mouse mammalian pancreas at least at some developmental stage. Species differences are at hand " diabetes and age-related differences are also to be considered. Eleven years ago a novel cell type, " development the ghrelin cell, was discovered in the human islets. Subsequent studies have shown the presence of islet ghrelin cells in several animals, including mouse, rat, gerbils, and fish. The developmental regulation of ghrelin cells in the islets of mice has gained a lot of interest and several studies have added important pieces to the puzzle of molecular mechanisms and the genetic regulation that lead to differentiation into mature ghrelin cells. -

GLIS3 Is Indispensable for TSH/TSHR-Dependent Thyroid Hormone Biosynthesis and Follicular Cell Proliferation
GLIS3 is indispensable for TSH/TSHR-dependent thyroid hormone biosynthesis and follicular cell proliferation Hong Soon Kang, … , Raja Jothi, Anton M. Jetten J Clin Invest. 2017;127(12):4326-4337. https://doi.org/10.1172/JCI94417. Research Article Endocrinology Deficiency in Krüppel-like zinc finger transcription factor GLI-similar 3 (GLIS3) in humans is associated with the development of congenital hypothyroidism. However, the functions of GLIS3 in the thyroid gland and the mechanism by which GLIS3 dysfunction causes hypothyroidism are unknown. In the current study, we demonstrate that GLIS3 acts downstream of thyroid-stimulating hormone (TSH) and TSH receptor (TSHR) and is indispensable for TSH/TSHR- mediated proliferation of thyroid follicular cells and biosynthesis of thyroid hormone. Using ChIP-Seq and promoter analysis, we demonstrate that GLIS3 is critical for the transcriptional activation of several genes required for thyroid hormone biosynthesis, including the iodide transporters Nis and Pds, both of which showed enhanced GLIS3 binding at their promoters. The repression of cell proliferation of GLIS3-deficient thyroid follicular cells was due to the inhibition of TSH-mediated activation of the mTOR complex 1/ribosomal protein S6 (mTORC1/RPS6) pathway as well as the reduced expression of several cell division–related genes regulated directly by GLIS3. Consequently, GLIS3 deficiency in a murine model prevented the development of goiter as well as the induction of inflammatory and fibrotic genes during chronic elevation of circulating TSH. Our study identifies GLIS3 as a key regulator of TSH/TSHR-mediated thyroid hormone biosynthesis and proliferation of thyroid follicular cells and uncovers a mechanism by which GLIS3 deficiency causes neonatal hypothyroidism and prevents goiter development. -

Beta Cell Physiological Dynamics and Dysfunctional Transitions in Response to Islet Inflammation in Obesity and Diabetes
H OH metabolites OH Review Beta Cell Physiological Dynamics and Dysfunctional Transitions in Response to Islet Inflammation in Obesity and Diabetes Marlon E. Cerf 1,2,3 1 Grants, Innovation and Product Development, South African Medical Research Council, Tygerberg 7505, South Africa; [email protected] 2 Biomedical Research and Innovation Platform, South African Medical Research Council, Tygerberg 7505, South Africa 3 Division of Medical Physiology, Department of Biomedical Sciences, Faculty of Medicine and Health Sciences, University of Stellenbosch, Tygerberg 7505, South Africa Received: 14 August 2020; Accepted: 10 October 2020; Published: 10 November 2020 Abstract: Beta cells adapt their function to respond to fluctuating glucose concentrations and variable insulin demand. The highly specialized beta cells have well-established endoplasmic reticulum to handle their high metabolic load for insulin biosynthesis and secretion. Beta cell endoplasmic reticulum therefore recognize and remove misfolded proteins thereby limiting their accumulation. Beta cells function optimally when they sense glucose and, in response, biosynthesize and secrete sufficient insulin. Overnutrition drives the pathogenesis of obesity and diabetes, with adverse effects on beta cells. The interleukin signaling system maintains beta cell physiology and plays a role in beta cell inflammation. In pre-diabetes and compromised metabolic states such as obesity, insulin resistance, and glucose intolerance, beta cells biosynthesize and secrete more insulin, i.e., hyperfunction. Obesity is entwined with inflammation, characterized by compensatory hyperinsulinemia, for a defined period, to normalize glycemia. However, with chronic hyperglycemia and diabetes, there is a perpetual high demand for insulin, and beta cells become exhausted resulting in insufficient insulin biosynthesis and secretion, i.e., they hypofunction in response to elevated glycemia. -

Wnt3a Upregulates Brain-Derived Insulin by Increasing Neurod1 Via
Lee et al. Molecular Brain (2016) 9:24 DOI 10.1186/s13041-016-0207-5 RESEARCH Open Access Wnt3a upregulates brain-derived insulin by increasing NeuroD1 via Wnt/β-catenin signaling in the hypothalamus Jaemeun Lee1, Kyungchan Kim1, Seong-Woon Yu1 and Eun-Kyoung Kim1,2* Abstract Background: Insulin plays diverse roles in the brain. Although insulin produced by pancreatic β-cells that crosses the blood–brain barrier is a major source of brain insulin, recent studies suggest that insulin is also produced locally within the brain. However, the mechanisms underlying the production of brain-derived insulin (BDI) are not yet known. Results: Here, we examined the effect of Wnt3a on BDI production in a hypothalamic cell line and hypothalamic tissue. In N39 hypothalamic cells, Wnt3a treatment significantly increased the expression of the Ins2 gene, which encodes the insulin isoform predominant in the mouse brain, by activating Wnt/β-catenin signaling. The concentration of insulin was higher in culture medium of Wnt3a-treated cells than in that of untreated cells. Interestingly, neurogenic differentiation 1 (NeuroD1), a target of Wnt/β-catenin signaling and one of transcription factors for insulin, was also induced by Wnt3a treatment in a time- and dose-dependent manner. In addition, the treatment of BIO, a GSK3 inhibitor, also increased the expression of Ins2 and NeuroD1. Knockdown of NeuroD1 by lentiviral shRNAs reduced the basal expression of Ins2 and suppressed Wnt3a-induced Ins2 expression. To confirm the Wnt3a-induced increase in Ins2 expression in vivo, Wnt3a was injected into the hypothalamus of mice. Wnt3a increased the expression of NeuroD1 and Ins2 in the hypothalamus in a manner similar to that observed in vitro. -

Regulating Distinct Cell Lineages in the Pancreatic Islet Joshua a Levine
Regulating Distinct Cell Lineages in the Pancreatic Islet Joshua A Levine Submitted in partial fulfillment of the Requirements for the degree of Doctor of Philosophy in the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2013 © 2012 Joshua A Levine All Rights Reserved ABSTRACT Regulating Distinct Cell Lineages in the Pancreatic Islet Joshua A Levine Type I and type II diabetes mellitus are associated with a loss of functioning insulin- producing β cells in the pancreas. Understanding the mechanism of normal islet and β cell development will be an important step in developing possible treatments for the disease. Nkx2.2 is essential for proper β cell differentiation. Nkx2.2-/- mice show a complete absence of insulin-producing β cells, a 90% reduction of glucagon-producing α cells, and an increase in ghrelin-producing cells. Nkx2.2 contains three conserved domains: the tinman domain (TN), homeodomain (HD), and NK2-specific domain (SD). The SD domain is highly conserved among Nk2 family members and across species. However, its function remains largely unknown. In order to further understand the molecular interactions involving Nkx2.2 in the developing mouse pancreas, we have generated a mouse line containing mutations in the NK2-SD domain. We show that SD mutant mice have a decrease in β cell numbers as well as a decrease in the β cell markers, NeuroD, Nkx6.1, Ins1 and Ins2. However, there is no change in α cell numbers or the α cell markers, Glucagon and Irx2. Unlike the persistent upregulation of ghrelin in the Nkx2.2-/- mice, Nkx2.2SD/SD mice display a transient increase in ghrelin expression, which normalizes by birth. -

Embryonic Endocrine Pancreas and Mature Β Cells Acquire Α and PP Cell Phenotypes Upon Arx Misexpression
Embryonic endocrine pancreas and mature β cells acquire α and PP cell phenotypes upon Arx misexpression Patrick Collombat, … , Palle Serup, Ahmed Mansouri J Clin Invest. 2007;117(4):961-970. https://doi.org/10.1172/JCI29115. Research Article Aristaless-related homeobox (Arx) was recently demonstrated to be involved in pancreatic α cell fate specification while simultaneously repressing the β and δ cell lineages. To establish whether Arx is not only necessary, but also sufficient to instruct the α cell fate in endocrine progenitors, we used a gain-of-function approach to generate mice conditionally misexpressing this factor. Mice with forced Arx expression in the embryonic pancreas or in developing islet cells developed a dramatic hyperglycemia and eventually died. Further analysis demonstrated a drastic loss of β and δ cells. Concurrently, a remarkable increase in the number of cells displaying α cell or, strikingly, pancreatic polypeptide (PP) cell features was observed. Notably, the ectopic expression of Arx induced in embryonic or adult β cells led to a loss of the β cell phenotype and a concomitant increase in a number of cells with α or PP cell characteristics. Combining quantitative real-time PCR and lineage-tracing experiments, we demonstrate that, in adult mice, the misexpression of Arx, rather than its overexpression, promotes a conversion of β cells into glucagon- or PP-producing cells in vivo. These results provide important insights into the complex mechanisms underlying proper pancreatic endocrine cell allocation and cell identity acquisition. Find the latest version: https://jci.me/29115/pdf Related Commentary, page 859 Research article Embryonic endocrine pancreas and mature β cells acquire α and PP cell phenotypes upon Arx misexpression Patrick Collombat,1 Jacob Hecksher-Sørensen,2 Jens Krull,1 Joachim Berger,3 Dietmar Riedel,4 Pedro L. -
Endocrine System
Chapter 17 *Lecture PowerPoint The Endocrine System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • In humans, two systems—the nervous and endocrine—communicate with neurotransmitters and hormones • This chapter is about the endocrine system – Chemical identity – How they are made and transported – How they produce effects on their target cells • The endocrine system is involved in adaptation to stress • There are many pathologies that result from endocrine dysfunctions 17-2 Overview of the Endocrine System • Expected Learning Outcomes – Define hormone and endocrine system. – Name several organs of the endocrine system. – Contrast endocrine with exocrine glands. – Recognize the standard abbreviations for many hormones. – Compare and contrast the nervous and endocrine systems. 17-3 Overview of the Endocrine System • The body has four principal mechanisms of communication between cells – Gap junctions • Pores in cell membrane allow signaling molecules, nutrients, and electrolytes to move from cell to cell – Neurotransmitters • Released from neurons to travel across synaptic cleft to second cell – Paracrine (local) hormones • Secreted into tissue fluids to affect nearby cells – Hormones • Chemical messengers that travel in the bloodstream to other tissues and organs 17-4 Overview of the Endocrine System • Endocrine system—glands, tissues, and cells that secrete hormones