1 Integrated Pancreatic Blood Flow: Bi-Directional
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Effects of Streptozotocin-Induced Diabetes on the Pineal Gland in the Domestic Pig
International Journal of Molecular Sciences Article Effects of Streptozotocin-Induced Diabetes on the Pineal Gland in the Domestic Pig Bogdan Lewczuk 1,* , Magdalena Prusik 1 , Natalia Ziółkowska 1, Michał D ˛abrowski 2, Kamila Martniuk 1, Maria Hanuszewska 1 and Łukasz Zielonka 2 1 Department of Histology and Embryology, Faculty of Veterinary Medicine, University of Warmia and Mazury in Olsztyn, Oczapowskiego 13, 10-719 Olsztyn, Poland; [email protected] (M.P.); [email protected] (N.Z.); [email protected] (K.M.); [email protected] (M.H.) 2 Department of Veterinary Prevention and Feed Hygiene, Faculty of Veterinary Medicine, University of Warmia and Mazury in Olsztyn, Oczapowskiego 13, 10-719 Olsztyn, Poland; [email protected] (M.D.); [email protected] (Ł.Z.) * Correspondence: [email protected]; Tel.: +48-89-523-39-49; Fax: +48-89-523-34-40 Received: 15 July 2018; Accepted: 5 October 2018; Published: 9 October 2018 Abstract: Several observations from experiments in rodents and human patients suggest that diabetes affects pineal gland function, including melatonin secretion; however, the accumulated data are not consistent. The aim of the present study was to determine the effects of streptozotocin-induced diabetes on the pineal gland in the domestic pig, a species widely used as a model in various biomedical studies. The study was performed on 10 juvenile pigs, which were divided into two groups: control and diabetic. Diabetes was evoked by administration of streptozotocin (150 mg/kg of body weight). After six weeks, the animals were euthanized between 12.00 and 14.00, and the pineal glands were removed and divided into two equal parts, which were used for biochemical analyses and for preparation of explants for the superfusion culture. -
Insulin Sensitivity and ß-Cell Function in Women with Polycystic Ovary
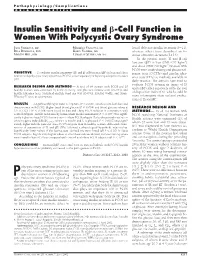
Pathophysiology/Complications ORIGINAL ARTICLE Insulin Sensitivity and -Cell Function in Women With Polycystic Ovary Syndrome JANA VRB´IKOVA´, MD MARKETA´ VANKOVA´, MS found defective insulin secretion (9–11), BELA BENDLOVA´, PHD KAREL VONDRA, MD whereas others have described an in- MARTIN HILL, PHD LUBOSLAV STARKA´ , MD, DSC crease of insulin secretion (12,13). In the present study, IS and -cell function (F) in lean (BMI Ͻ27 kg/m2) and obese (BMI Ն27 kg/m2) women with PCOS were studied using oral glucose tol-   OBJECTIVE — To evaluate insulin sensitivity (IS) and -cell function ( F) in lean and obese erance tests (OGTTs) and insulin toler- women with polycystic ovary syndrome (PCOS), either separately or by using a disposition index ance tests (ITTs) as methods available in (DI). daily practice. The authors have tried to evaluate PCOS women in terms of IS RESEARCH DESIGN AND METHODS — A total of 64 women with PCOS and 20 and/or F either separately or by the tool healthy women were examined by anthropometry, oral glucose tolerance tests (OGTTs), and insulin tolerance tests. Statistical analysis used one-way ANOVA, Kruskal-Wallis, and Mann- of disposition index (DI), which could be Whitney U tests, as appropriate. more informative than isolated evalua- tions of IS and F. RESULTS — A significantly higher waist-to-hip ratio (P Ͻ 0.0001) was found in both lean and obese women with PCOS. Higher basal blood glucose (P Ͻ 0.004) and blood glucose values at RESEARCH DESIGN AND 3 h of OGTT (P Ͻ 0.008) were found in lean and obese PCOS subjects in comparison with METHODS — In all, 64 women with control subjects. -

Endocrine Cell Type Sorting and Mature Architecture in the Islets Of
www.nature.com/scientificreports OPEN Endocrine cell type sorting and mature architecture in the islets of Langerhans require expression of Received: 16 April 2018 Accepted: 4 July 2018 Roundabout receptors in β cells Published: xx xx xxxx Melissa T. Adams, Jennifer M. Gilbert, Jesus Hinojosa Paiz, Faith M. Bowman & Barak Blum Pancreatic islets of Langerhans display characteristic spatial architecture of their endocrine cell types. This architecture is critical for cell-cell communication and coordinated hormone secretion. Islet architecture is disrupted in type-2 diabetes. Moreover, the generation of architecturally correct islets in vitro remains a challenge in regenerative approaches to type-1 diabetes. Although the characteristic islet architecture is well documented, the mechanisms controlling its formation remain obscure. Here, we report that correct endocrine cell type sorting and the formation of mature islet architecture require the expression of Roundabout (Robo) receptors in β cells. Mice with whole-body deletion of Robo1 and conditional deletion of Robo2 either in all endocrine cells or selectively in β cells show complete loss of endocrine cell type sorting, highlighting the importance of β cells as the primary organizer of islet architecture. Conditional deletion of Robo in mature β cells subsequent to islet formation results in a similar phenotype. Finally, we provide evidence to suggest that the loss of islet architecture in Robo KO mice is not due to β cell transdiferentiation, cell death or loss of β cell diferentiation or maturation. Te islets of Langerhans display typical, species-specifc architecture, with distinct spatial organization of their various endocrine cell types1–5. In the mouse, the core of the islet is composed mostly of insulin-secreting β cells, while glucagon-secreting α cells, somatostatin-secreting δ cells and pancreatic polypeptide-secreting PP cells are located at the islet periphery3. -

The Role of Thyroid Hormone
Central Journal of Endocrinology, Diabetes & Obesity Mini Review Special Issue on Role of Thyroid Hormone Pancreatic and Islet Develop- in Metabolic Homeostasis ment and Function: The Role of *Corresponding authors Teresa L Mastracci, Department of Pediatrics, Indiana University School of Medicine, Herman B Wells Center for Thyroid Hormone Pediatric Research, 635 Barnhill Dr, MS2031, Indianapolis, IN, USA 46202, Tel: 317-278-8940; Fax: 317-274-4107; Teresa L Mastracci1,5* and Carmella Evans-Molina2,3,4,5* Email: 1Department of Pediatrics, Indiana University School of Medicine, USA Carmella Evans-Molina, Department of Medicine, 2Department of Medicine, Indiana University School of Medicine, USA Cellular and Integrative Physiology, Biochemistry and 3Department of Cellular and Integrative Physiology, Indiana University School of Molecular Biology, Herman B Wells Center for Pediatric Medicine, USA Research, Indiana University School of Medicine, 4Department of Biochemistry and Molecular Biology, Indiana University School of Indiana University School of Medicine, 635 Barnhill Dr., Medicine, USA MS2031, Indianapolis, IN, USA 46202, Tel: 317-278-3177; 5Herman B Wells Center for Pediatric Research, Indiana University School of Medicine, Fax: 317-274-4107; Email: USA Submitted: 12 June 2014 Accepted: 17 July 2014 Published: 19 July 2014 Abstract ISSN: 2333-6692 A gradually expanding body of literature suggests that Thyroid Hormone (TH) Copyright and Thyroid Hormone Receptors (TRs) play a contributing role in pancreatic and islet © 2014 Mastracci et al. cell development, maturation, and function. Studies using a variety of model systems capable of exploiting species-specific developmental paradigms have revealed the OPEN ACCESS contribution of TH to cellular differentiation, lineage decisions, and endocrine cell specification. -
![First Responder Cells Drive the First-Phase [Ca2+] Response](https://docslib.b-cdn.net/cover/3508/first-responder-cells-drive-the-first-phase-ca2-response-733508.webp)
First Responder Cells Drive the First-Phase [Ca2+] Response
bioRxiv preprint doi: https://doi.org/10.1101/2020.12.22.424082; this version posted December 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Functional architecture of the pancreatic islets: First responder cells drive the first-phase [Ca2+] response Vira Kravetsa,b, JaeAnn M. Dwuleta, Wolfgang E. Schleicherb, David J. Hodsonc, Anna M. Davis,a Robert A. Piscopiob, Maura Sticco-Ivins,b Richard K.P. Benningera,b,1. a Department of Bioengineering, University of Colorado, Anschutz Medical campus, Aurora, CO. USA b Barbara Davis center for childhood diabetes, University of Colorado, Anschutz Medical campus, Aurora, CO. USA c Institute of Metabolism and Systems Research, University of Birmingham, Birmingham. UK, and Centre for Endocrinology, Diabetes and Metabolism, Birmingham Health Partners, Birmingham, UK 1 To whom correspondence should be addressed: [email protected] Tel: (303) 724-6388. Fax: (303) 724-5800. 1775 Aurora court, M20-4306D, mailstop B140, University of Colorado Anschutz Medical campus, Aurora, CO. 80045. Short title: First responder cells control islet function Keywords: Laser ablation; Multicellular Dynamics; Biological Networks; Optical Microscopy; Diabetes; Gap junctions. Manuscript word count (main text, excluding methods): 5311. Abstract word count: 294 bioRxiv preprint doi: https://doi.org/10.1101/2020.12.22.424082; this version posted December 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Abstract Insulin-secreting b-cells are functionally heterogeneous. Subpopulations of b-cells can control islet function and the regulation of hormone release, such as driving the second (oscillatory) phase of free-calcium ([Ca2+]) following glucose elevation. -

GLIS3 Is Indispensable for TSH/TSHR-Dependent Thyroid Hormone Biosynthesis and Follicular Cell Proliferation
GLIS3 is indispensable for TSH/TSHR-dependent thyroid hormone biosynthesis and follicular cell proliferation Hong Soon Kang, … , Raja Jothi, Anton M. Jetten J Clin Invest. 2017;127(12):4326-4337. https://doi.org/10.1172/JCI94417. Research Article Endocrinology Deficiency in Krüppel-like zinc finger transcription factor GLI-similar 3 (GLIS3) in humans is associated with the development of congenital hypothyroidism. However, the functions of GLIS3 in the thyroid gland and the mechanism by which GLIS3 dysfunction causes hypothyroidism are unknown. In the current study, we demonstrate that GLIS3 acts downstream of thyroid-stimulating hormone (TSH) and TSH receptor (TSHR) and is indispensable for TSH/TSHR- mediated proliferation of thyroid follicular cells and biosynthesis of thyroid hormone. Using ChIP-Seq and promoter analysis, we demonstrate that GLIS3 is critical for the transcriptional activation of several genes required for thyroid hormone biosynthesis, including the iodide transporters Nis and Pds, both of which showed enhanced GLIS3 binding at their promoters. The repression of cell proliferation of GLIS3-deficient thyroid follicular cells was due to the inhibition of TSH-mediated activation of the mTOR complex 1/ribosomal protein S6 (mTORC1/RPS6) pathway as well as the reduced expression of several cell division–related genes regulated directly by GLIS3. Consequently, GLIS3 deficiency in a murine model prevented the development of goiter as well as the induction of inflammatory and fibrotic genes during chronic elevation of circulating TSH. Our study identifies GLIS3 as a key regulator of TSH/TSHR-mediated thyroid hormone biosynthesis and proliferation of thyroid follicular cells and uncovers a mechanism by which GLIS3 deficiency causes neonatal hypothyroidism and prevents goiter development. -

GLP-1 Effects on Islets: Hormonal, Neuronal, Or Paracrine?
DIABETES PATHOPHYSIOLOGY GLP-1 Effects on Islets: Hormonal, Neuronal, or Paracrine? 1 MARC Y. DONATH, MD control of glycemia through the activation 2 RÉMY BURCELIN, PHD of the gut brain axis. Furthermore, the di- rect administration of the DPP-4 inhibitor into the rat portal vein significantly in- creased portal (but not peripheral) GLP-1 ccording to the classical incretin con- (5) within minutes from the absorption and insulin levels and decreased glucose Acept, glucagon-like peptide (GLP)-1 of glucose and lipids. The final aim of concentrations (14). However, despite the is viewed as a hormone produced this axis is to anticipate the breakthrough large amount of experimental evidence de- in the intestinal L cells and acting via of the nutrients into the blood and their scribed above showing the important role the circulation on satiety in the brain, better handling. Indeed, GLP-1 secreted of GLP-1 on the gut-to-brain axis, a recent gut motility, and insulin and glucagon from L cells can influence brain neuronal observation in mice suggests that the circu- secretion in the pancreatic islet. How- activities via an alternative neural path- lating GLP-1 could also directly access the ever, in contrast to typical hormones, way initiated by sensors in the hepatic brain and the b-cells and induce insulin plasma levels of GLP-1 are relatively low portal region (6–8). Thereby, the vagus secretion (15). Transgenic mice that ex- with a very short half-life. Furthermore, nerve transmits the metabolic infor- pressed the human GLP-1 receptor in islets GLP-1 is rapidly inactivated by dipep- mation to the nucleus tractus solitarii and in pancreatic ductal cells within the tidyl peptidase-4 (DPP-4) in the vicinity in the brain stem, which relays the glu- background of the GLP-1 receptor knock- of L cells within ,1 min from the secre- cose signal to hypothalamic nuclei (9). -

Beta Cell Physiological Dynamics and Dysfunctional Transitions in Response to Islet Inflammation in Obesity and Diabetes
H OH metabolites OH Review Beta Cell Physiological Dynamics and Dysfunctional Transitions in Response to Islet Inflammation in Obesity and Diabetes Marlon E. Cerf 1,2,3 1 Grants, Innovation and Product Development, South African Medical Research Council, Tygerberg 7505, South Africa; [email protected] 2 Biomedical Research and Innovation Platform, South African Medical Research Council, Tygerberg 7505, South Africa 3 Division of Medical Physiology, Department of Biomedical Sciences, Faculty of Medicine and Health Sciences, University of Stellenbosch, Tygerberg 7505, South Africa Received: 14 August 2020; Accepted: 10 October 2020; Published: 10 November 2020 Abstract: Beta cells adapt their function to respond to fluctuating glucose concentrations and variable insulin demand. The highly specialized beta cells have well-established endoplasmic reticulum to handle their high metabolic load for insulin biosynthesis and secretion. Beta cell endoplasmic reticulum therefore recognize and remove misfolded proteins thereby limiting their accumulation. Beta cells function optimally when they sense glucose and, in response, biosynthesize and secrete sufficient insulin. Overnutrition drives the pathogenesis of obesity and diabetes, with adverse effects on beta cells. The interleukin signaling system maintains beta cell physiology and plays a role in beta cell inflammation. In pre-diabetes and compromised metabolic states such as obesity, insulin resistance, and glucose intolerance, beta cells biosynthesize and secrete more insulin, i.e., hyperfunction. Obesity is entwined with inflammation, characterized by compensatory hyperinsulinemia, for a defined period, to normalize glycemia. However, with chronic hyperglycemia and diabetes, there is a perpetual high demand for insulin, and beta cells become exhausted resulting in insufficient insulin biosynthesis and secretion, i.e., they hypofunction in response to elevated glycemia. -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria. -

Why Pancreatic Islets Should Be Regarded and Regulated Like Organs
CellR4 2021; 9: e3083 Why pancreatic islets should be regarded and regulated like organs G. C. Weir, S. Bonner-Weir Section on Islet Cell and Regenerative Biology, Joslin Diabetes Center, Harvard Medical School, Boston, MA, USA Corresponding Author: Gordon C. Weir, MD; e-mail: [email protected] Keywords: Autologous transplantation, Islet transplanta- islets transplants, processed exactly in the same way, tion, Pancreatic alpha cells, Pancreatic beta cells, Pancreatic are exempted from these drugs regulations in the islets. US. Alloislets are exempt from drug regulation, and safely and effectively offered as a standard-of-care ABSTRACT treatment option in a number of developed nations, There are strong reasons to say that pancreatic with the notable exception of the US. islets are organs before they are isolated and Some of the basis for distinguishing between that they should be considered to be organs once allogenic islets and other organ/vascularized com- transplanted. Thus, taking into account how posite tissues lies in taking the position that alloge- much we have learned about the structure and neic islets are not to be vascularized organs, which function of islet micro-organs, it seems highly led to the plan to regulate them as drugs, which is illogical to on one hand consider autologous how cellular transplants are regulated. islets be regulated as organ transplants and al- Although there are many complexities, there loislets to be regulated with the very restrictive is the simple question of whether islets are organs. rules used for cell transplantation. It is partic- The answer for many is clearly yes, and that would ularly problematic that this policy has led to pertain to both autologous islets and alloislets. -

Wnt3a Upregulates Brain-Derived Insulin by Increasing Neurod1 Via
Lee et al. Molecular Brain (2016) 9:24 DOI 10.1186/s13041-016-0207-5 RESEARCH Open Access Wnt3a upregulates brain-derived insulin by increasing NeuroD1 via Wnt/β-catenin signaling in the hypothalamus Jaemeun Lee1, Kyungchan Kim1, Seong-Woon Yu1 and Eun-Kyoung Kim1,2* Abstract Background: Insulin plays diverse roles in the brain. Although insulin produced by pancreatic β-cells that crosses the blood–brain barrier is a major source of brain insulin, recent studies suggest that insulin is also produced locally within the brain. However, the mechanisms underlying the production of brain-derived insulin (BDI) are not yet known. Results: Here, we examined the effect of Wnt3a on BDI production in a hypothalamic cell line and hypothalamic tissue. In N39 hypothalamic cells, Wnt3a treatment significantly increased the expression of the Ins2 gene, which encodes the insulin isoform predominant in the mouse brain, by activating Wnt/β-catenin signaling. The concentration of insulin was higher in culture medium of Wnt3a-treated cells than in that of untreated cells. Interestingly, neurogenic differentiation 1 (NeuroD1), a target of Wnt/β-catenin signaling and one of transcription factors for insulin, was also induced by Wnt3a treatment in a time- and dose-dependent manner. In addition, the treatment of BIO, a GSK3 inhibitor, also increased the expression of Ins2 and NeuroD1. Knockdown of NeuroD1 by lentiviral shRNAs reduced the basal expression of Ins2 and suppressed Wnt3a-induced Ins2 expression. To confirm the Wnt3a-induced increase in Ins2 expression in vivo, Wnt3a was injected into the hypothalamus of mice. Wnt3a increased the expression of NeuroD1 and Ins2 in the hypothalamus in a manner similar to that observed in vitro. -
Endocrine System
Chapter 17 *Lecture PowerPoint The Endocrine System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • In humans, two systems—the nervous and endocrine—communicate with neurotransmitters and hormones • This chapter is about the endocrine system – Chemical identity – How they are made and transported – How they produce effects on their target cells • The endocrine system is involved in adaptation to stress • There are many pathologies that result from endocrine dysfunctions 17-2 Overview of the Endocrine System • Expected Learning Outcomes – Define hormone and endocrine system. – Name several organs of the endocrine system. – Contrast endocrine with exocrine glands. – Recognize the standard abbreviations for many hormones. – Compare and contrast the nervous and endocrine systems. 17-3 Overview of the Endocrine System • The body has four principal mechanisms of communication between cells – Gap junctions • Pores in cell membrane allow signaling molecules, nutrients, and electrolytes to move from cell to cell – Neurotransmitters • Released from neurons to travel across synaptic cleft to second cell – Paracrine (local) hormones • Secreted into tissue fluids to affect nearby cells – Hormones • Chemical messengers that travel in the bloodstream to other tissues and organs 17-4 Overview of the Endocrine System • Endocrine system—glands, tissues, and cells that secrete hormones