Country Programme Evaluation: Cameroon 2008-2011
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
De 40 MINMAP Région Du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES
MINMAP Région du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de N° Désignation des MO/MOD Montant des Marchés N° Page Marchés 1 Communauté Urbaine de Garoua 11 847 894 350 3 2 Services déconcentrés régionaux 20 528 977 000 4 Département de la Bénoué 3 Services déconcentrés départementaux 10 283 500 000 6 4 Commune de Barndaké 13 376 238 000 7 5 Commune de Bascheo 16 305 482 770 8 6 Commune de Garoua 1 11 201 187 000 9 7 Commune de Garoua 2 26 498 592 344 10 8 Commune de Garoua 3 22 735 201 727 12 9 Commune de Gashiga 21 353 419 404 14 10 Commune de Lagdo 21 2 026 560 930 16 11 Commune de Pitoa 18 360 777 700 18 12 Commune de Bibémi 18 371 277 700 20 13 Commune de Dembo 11 300 277 700 21 14 Commune de Ngong 12 235 778 000 22 15 Commune de Touroua 15 187 777 700 23 TOTAL 214 6 236 070 975 Département du Faro 16 Services déconcentrés 5 96 500 000 25 17 Commune de Beka 15 230 778 000 25 18 Commune de Poli 22 481 554 000 26 TOTAL 42 808 832 000 Département du Mayo-Louti 19 Services déconcentrés 6 196 000 000 28 20 Commune de Figuil 16 328 512 000 28 21 Commune de Guider 28 534 529 000 30 22 Commune de Mayo Oulo 24 331 278 000 32 TOTAL 74 1 390 319 000 MINMAP / DIVISION DE LA PROGRAMMATION ET DU SUIVI DES MARCHES PUBLICS Page 1 de 40 MINMAP Région du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de N° Désignation des MO/MOD Montant des Marchés N° Page Marchés Département du Mayo-Rey 23 Services déconcentrés 7 152 900 000 35 24 Commune de Madingring 14 163 778 000 35 24 Commune de Rey Bouba -

Cameroon : Adamawa, East and North Rgeions
CAMEROON : ADAMAWA, EAST AND NORTH RGEIONS 11° E 12° E 13° E 14° E N 1125° E 16° E Hossere Gaval Mayo Kewe Palpal Dew atan Hossere Mayo Kelvoun Hossere HDossere OuIro M aArday MARE Go mbe Trabahohoy Mayo Bokwa Melendem Vinjegel Kelvoun Pandoual Ourlang Mayo Palia Dam assay Birdif Hossere Hosere Hossere Madama CHARI-BAGUIRMI Mbirdif Zaga Taldam Mubi Hosere Ndoudjem Hossere Mordoy Madama Matalao Hosere Gordom BORNO Matalao Goboum Mou Mayo Mou Baday Korehel Hossere Tongom Ndujem Hossere Seleguere Paha Goboum Hossere Mokoy Diam Ibbi Moukoy Melem lem Doubouvoum Mayo Alouki Mayo Palia Loum as Marma MAYO KANI Mayo Nelma Mayo Zevene Njefi Nelma Dja-Lingo Birdi Harma Mayo Djifi Hosere Galao Hossere Birdi Beli Bili Mandama Galao Bokong Babarkin Deba Madama DabaGalaou Hossere Goudak Hosere Geling Dirtehe Biri Massabey Geling Hosere Hossere Banam Mokorvong Gueleng Goudak Far-North Makirve Dirtcha Hwoli Ts adaksok Gueling Boko Bourwoy Tawan Tawan N 1 Talak Matafal Kouodja Mouga Goudjougoudjou MasabayMassabay Boko Irguilang Bedeve Gimoulounga Bili Douroum Irngileng Mayo Kapta Hakirvia Mougoulounga Hosere Talak Komboum Sobre Bourhoy Mayo Malwey Matafat Hossere Hwoli Hossere Woli Barkao Gande Watchama Guimoulounga Vinde Yola Bourwoy Mokorvong Kapta Hosere Mouga Mouena Mayo Oulo Hossere Bangay Dirbass Dirbas Kousm adouma Malwei Boulou Gandarma Boutouza Mouna Goungourga Mayo Douroum Ouro Saday Djouvoure MAYO DANAY Dum o Bougouma Bangai Houloum Mayo Gottokoun Galbanki Houmbal Moda Goude Tarnbaga Madara Mayo Bozki Bokzi Bangei Holoum Pri TiraHosere Tira -

Proceedingsnord of the GENERAL CONFERENCE of LOCAL COUNCILS
REPUBLIC OF CAMEROON REPUBLIQUE DU CAMEROUN Peace - Work - Fatherland Paix - Travail - Patrie ------------------------- ------------------------- MINISTRY OF DECENTRALIZATION MINISTERE DE LA DECENTRALISATION AND LOCAL DEVELOPMENT ET DU DEVELOPPEMENT LOCAL Extrême PROCEEDINGSNord OF THE GENERAL CONFERENCE OF LOCAL COUNCILS Nord Theme: Deepening Decentralization: A New Face for Local Councils in Cameroon Adamaoua Nord-Ouest Yaounde Conference Centre, 6 and 7 February 2019 Sud- Ouest Ouest Centre Littoral Est Sud Published in July 2019 For any information on the General Conference on Local Councils - 2019 edition - or to obtain copies of this publication, please contact: Ministry of Decentralization and Local Development (MINDDEVEL) Website: www.minddevel.gov.cm Facebook: Ministère-de-la-Décentralisation-et-du-Développement-Local Twitter: @minddevelcamer.1 Reviewed by: MINDDEVEL/PRADEC-GIZ These proceedings have been published with the assistance of the German Federal Ministry for Economic Cooperation and Development (BMZ) through the Deutsche Gesellschaft für internationale Zusammenarbeit (GIZ) GmbH in the framework of the Support programme for municipal development (PROMUD). GIZ does not necessarily share the opinions expressed in this publication. The Ministry of Decentralisation and Local Development (MINDDEVEL) is fully responsible for this content. Contents Contents Foreword ..............................................................................................................................................................................5 -

Monthly Humanitarian Situation Report CAMEROON Date: 27Th May 2013
Monthly Humanitarian Situation Report CAMEROON Date: 27th May 2013 Highlights The Health and Nutrition week (SASNIM) was organized in the 10 regions from 26 to 30 April; 1,152,045 children aged 6-59 months received vitamin A and 1,349,937 children aged 12-59 months were dewormed in the Far North and North region. 1,727,391 (101%) children under 5 received Polio drops (OPV), and 38,790 pregnant women received Intermittent Preventive treatment (IPT). A mass screening of acute malnutrition in the North and Far North region was carried out during [the Mother and Child Health and Nutrition Action Week (SASNIM), reaching 90% of children. Out of 1,420,145 children 6-59 months estimated to be covered, 1,288,475 children were enrolled in the mass screening with MUAC, 425,892 in the North region and 862,583 in the Far North. 50,583 MAM cases and 9,269 SAM cases were found and referred to outpatient centres. 10 health districts out of 43 require urgent action. A 10 member delegation led by the UN Foundation team consisting of US Congressional aides and Rotary International visited Garoua - North Region to look at Child Survival and HIV initiatives from April 27 – May 2nd 2013. Following the declaration of state of emergency on May 14 in Nigeria, the actions carried out by Nigerian Government towards the Boko Haram rebels in Maiduguru State (neighbor of Cameroon) may lead to displacement of population from Nigeria to Cameroun. Some Cameroonians living near Nigeria Borno State are moving into Far North region of Cameroon. -

N.Pmruixior Uurrrm DIRECTION DES RESSOURCES RESOURCES HUMAINES
REPUBLIQUE DU CAMEROUN Rf,PUBLTC OF CAMEROON Paix-Travail-Patrie Peace.Work-Fatherlând MINISTERE DE L'EDUCATION DE MINISTRY OF BASIC EDUCATION BASE GENERAL SECRETARIAT SECRETARIAT Gf,NERAL n.pmruixior uurrrm DIRECTION DES RESSOURCES RESOURCES HUMAINES TROISIEME PROGRAMME DE CONTRACTUALISATION DES INSTITUTEURS AU MINISTERE DE L'EDUCATION DE BASE DEUXIEME OPERATION AU TITRE DE L'EXERCICE 2O2O usrE DEs EcoLEs NECESSTTEUSES (JOB POSTING ) REGION DU NORD N" REGION DEPARTEMENT ARRONDISSEMENT NOM DE L'ECOLE 1 NORD BENOUE BASCHEO ECOLE PUBLIQUE DE BASCHEO 2 NORD BEN OU E BASCHEO EP BANTAYE-BASCH EO 3 NORD BE NOU E BASCHEO EP BARGOUMA 4 NORD BENOUE BASCHEO EP BOMBOL 5 NORD BENOU E BASCHEO EP DARAM 6 NORD BE NOU E BASCHEO EP DARPATA 7 NORD BE NOU E BASCHEO EP DJALINGO.BELEL 8 NORD BEN OU E BASCHEO EP DJAOURO-MOUSSA 9 NORD BEN OU E BASCHEO EP DJARENGOL 10 NORD BEN OU E BASCHEO EP DORBA 11 NORD B ENOU E BASCHEO EP FOULBERE 72 NORD BENOUE BASCHEO EP GASSIRE -15 NORD B ENOU E BASCHEO EP HAMAKOUSSOU 14 NORD B ENOU E BASCHEO EP HAMAYEL 15 NORD BENO U E BASCHEO EP HARKOU NORD BENOUE BASCHEO EP KATAKO 17 NORD 8 ENOU E BASCHEO EP KATCHATCHIA 18 NORD BENOUE BASCHEO EP KERZING 19 NORD BENOUE EASCHEO EP KOBOSSI 20 NORD B ENOU E BASCHEO EP LARIA 2t NORD BENOUE BASCHEO EP MALKOUROU NORD BENOU E BASCHEO EP MAPOUTKI 23 NORD BENOUE BASCHEO EP MAYO-OULO-FALI 24 NORD BENOUE BASCHEO EP MBABI 25 NORD BENOUE BASCHEO EP MBOULMI 26 NORD BENOUE BASCHEO EP NARO-KOUBADJE 27 NORD 8 ENOU E BASCHEO EP NASSARAO 28 NORD BENOUE BASCHEO EP NGOUROU-DABA 29 NORD BENOUE BASCHEO EP -
Expanded PDF Profile
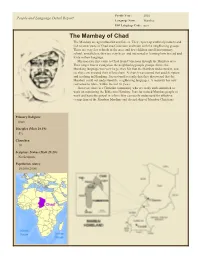
Profile Year: 2001 People and Language Detail Report Language Name: Mambai ISO Language Code: mcs The Mambay of Chad The Mambay are agriculturalist and fishers. They export agricultural products and fish to other parts of Chad and Cameroon and trade with the neighboring groups. There are very few schools in the area, and few children enroll into primary school, nonetheless, they are very keen and interested in learning how to read and write in their language. Missionaries first came to Chad from Cameroon through the Mambay area. Their target was to evangelize the neighboring people groups. Since, the Mundang language was very large, they felt that the Mambay understand it, and so, they concentrated their efforts there. A church was started that used Scripture and teaching in Mundang. It is not until recently that they discovered that the Mambay could not understand the neighboring languages. A majority has now converted to Islam, within the last 30 years. However, there is a Christian community who are ready and committed to work on translating the Bible into Mambay. Pray for trained Mambay people to work and have the gospel in a form they can easily understand for effective evangelism of the Mambay Muslims and discipleship of Mambay Christians. Primary Religion: Islam Disciples (Matt 28.19): 5% Churches: 10 Scripture Status (Matt 28.20): No Scripture Population (date): 10,000 (2000) The Mambay of Chad Item Name Item Note Have They Heard The Gospel? Profile Summary Call Themselves Christian (%) 25 Believe In Jesus As God & Only Savior (%) 5% Prophet/Good Man, But Not God's Son (%) 75 Have Not Heard Who Jesus is (%) ? Believe Jesus Is A Myth (%) 0 Number Of Pastors 10 Comment (Pastors) 10 pastors based on pastor ratio of 1:1,000 and population of 10,000 Number Of Communities 26 villages Number Of Churches 10 Is The Word Of God Translated? No Any Hinderance To Scripture Distribution? Illiteracy rate is quite high. -

Floods and Cholera Epidemic
EPoA Operations Update Cameroon: Floods and Cholera Epidemic DREF Operation no. MDRCM020 GLIDE n° EP-2014-000121-CMR Operations update n° 1 Period covered by this update: 8 September to 5 November, 2014 Operation start date:8 September, 2014 Timeframe: 5 months (End date: 5 February 2015) Operation budget:CHF 308,136 (Initial allocation:CHF 179,304;additional allocation:CHF 128,832) N° of people being assisted: 52,380 (initial number targeted to be assisted was 26,380) Host National Society presence: 25,000 volunteers, more than 50 staff, 58 departmental branches and 250 local branches. Red Cross Red Crescent Movement partners actively involved in the operation: IFRC Other partner organizations actively involved in the operation: Ministry of Public Health, Local Administration Authorities Summary: This operations update extends the operation timeframe by an additional 2 months with an additional budget allocation of CHF 128,832 to; Reinforce public outreach / awareness-raising activities in the six localities, which were included in the EPoA (Bibemi, Figuil, Guider, Mayo-Oulo, Pitoa, and Touboro), in an effort to improve the populations’ sanitation and hygiene practices and thus combat the cholera epidemic in 12 districts (six additional districts) of the North Region of Cameroon Extend these activities into the six localities where new cases have been reported (Garoua I, Garoua II, Gashiga, Golombé, Rey Bouba and Tcholiré). The DREF budget revision will cover the training (on Epidemic Control for Volunteers (ECV) manual); and deployment of an Cameroon RC volunteers offloading NFIs in Bibemi. Photo: IFRC additional 50 volunteers and five supervisors (additional 10 volunteers and one supervisor per locality) in five existing localities (Figuil, Guider, Mayo-Oulo, Pitoa, and Touboro); as well as an additional 130 volunteers and 13 supervisors in the six localities where new cases have been reported (Garoua I, Garoua II, Gashiga, Golombe, Rey Bouba and Tcholiré. -

The World Bank for OFFICIAL USE ONLY
Document of The World Bank FOR OFFICIAL USE ONLY Report No: 74701-CM Public Disclosure Authorized PROJECT APPRAISAL DOCUMENT ON A PROPOSED CREDIT IN THE AMOUNT OF SDR 32.5 MILLION Public Disclosure Authorized (US$50 MILLION EQUIVALENT) TO THE REPUBLIC OF CAMEROON FOR A SOCIAL SAFETY NET PROJECT March 4, 2013 Public Disclosure Authorized Human Development Country Department AFCC1 Africa Region This document has a restricted distribution and may be used by recipients only in the Public Disclosure Authorized performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective January 31, 2013) Currency Unit = XAF XAF484 = US$1 US$1.54 = SDR 1 FISCAL YEAR January 1 - December 31 ABBREVIATIONS AND ACRONYMS ASPEN Africa Safeguard Policies Enhancement BAD Banque Africaine de Diveloppement BP Bank Policy BUCREP Bureau Centraldes Recensements des Etudes de Population CA Credit Agreement CAS Country Assistance Strategy CCT Conditional Cash Transfer CSMP Commission Spiciale de Passationdes Marchis Publics CT Cash Transfer CTS Comit Technique de Suivi des ProgrammesEconomiques DSCE Document de Stratigie Pour la Croissance et L'Emploi DL Disbursement Letter ECAM Enqu6te CambrounaiseAupris de Manages EOI Expression of Interest ESIA Environmental Social Impact Assessments ESW Economic and Sector Work ESMF Environmental and Social Management Framework ESMP Environmental and Social Management Plans EU European Union FCFA Central African Franc/Francde la Coopbration -

Cameroun : Situation De L'épidémie De Choléra Dans Les Régions Du Nord Et De L'extrême-Nord
Cameroun : Situation de l’épidémie de Choléra dans les régions du Nord et de l’Extrême-Nord (10/10/2019) FAITS SAILLANTS o Âge médian : 28 ans (1 an - 90 ans) ; o Taux de létalité : 5,8%. - Présence opérationnelle faibles des partenaires du secteur santé dans les districts de santé enregistrant encore une transmission active de la 100 Cas Décès maladie ; 90 80 - Transmission active du choléra dans les districts de santé Bibémi, Garoua 70 I, Garoua II (Région du Nord) et Kar Hay (région de l’Extrême-Nord) ; 60 50 Nombre de cas 40 - Pour l’ensemble des deux régions depuis la date de déclaration de 30 20 l’épidémie jusqu’au 10/10/2019 : 10 o 1 581 cas enregistrés avec 89 décès ; 0 o Taux de létalité : 5,6%. 2018-SE20 2018-SE23 2018-SE26 2018-SE29 2018-SE32 2018-SE35 2018-SE38 2018-SE41 2018-SE44 2018-SE47 2018-SE50 2019-SE01 2019-SE04 2019-SE07 2019-SE10 2019-SE13 2019-SE16 2019-SE19 2019-SE22 2019-SE25 2019-SE28 2019-SE31 2019-SE34 2019-SE37 2019-SE40 SITUATION ÉPIDÉMIOLOGIQUE Semaine épidémiologique DANS LA RÉGION DU NORD EN 2019 Figure 2 : Courbe épidémique des cas de choléra, région du Nord (2018 et 2019) - 9/15 districts de santé ont enregistré des cas de choléra (Bibémi, Figuil, 31% 56% 13% 54% Garoua I, Garoua II, Gashiga, Golombe, Ngong, Pitoa, Tcholliré) ; < 18 ans 18-59 ans 60 ans et + Femmes - 35 cas enregistrés entre la 38ème et la 41ème semaine épidémiologique (22 cas soit 63% issus du district de santé Bibémi) ; - À ce jour o 402 cas enregistrés avec 20 décès (12 hospitaliers et 08 en communauté) ; o Taux de létalité : 5,0% ; o 88/118 échantillons confirmés ; o Âge médian : 30 ans (1 an – 86 ans). -
Plan Communal De Developpement De Figuil
REPUBLIQUE DU CAMEROUN REPUBLIC OF CAMEROON ------------ --------- Paix – Travail – Patrie Peace – Work – Fatherland ----------- ---------- MINISTERE DE L’ADMINISTRATION MINISTRY OF TERRITORIAL TERRITORIALE ET DE LA ADMINISTRATION AND DECENTRALISATION DECENTRALISATION ----------- ------------ REGION DU NORD NORTH REGION ------------- ---------- DEPARTEMENT DU MATO-LOUTI MAYO-LOUTI DIVISION ------------ ---------- COMMUNE DE FIGUIL FIGUIL COUNCIL PLAN COMMUNAL DE DEVELOPPEMENT DE FIGUIL Hôtel de ville de Figuil SEPTEMBRE 2015 PLAN COMMUNAL DE DEVELOPPEMENT DE FIGUIL 2015 Validation du PCD FIGUIL le …………….......... GUIDER le ……………........... Le Maire DE FIGUIL Le DD MINEPAT DU MAYO-LOUTI GUIDER le ……………........... Le PREFET DU MAYO-LOUTI Commune de Figuil BP : E-mail : Tél (+237) Page 1 PLAN COMMUNAL DE DEVELOPPEMENT DE FIGUIL 2015 Sommaire Sommaire ....................................................................................................................................................................................................... 2 Résumé .......................................................................................................................................................................................................... 5 Liste des abréviations ..................................................................................................................................................................................... 6 Liste des tableaux ......................................................................................................................................................................................... -

CAMEROON GENDER and ENVIRONMENT WATCH (CAMGEW) Republic of Cameroon
CAMEROON GENDER AND ENVIRONMENT WATCH (CAMGEW) Republic of Cameroon Equator Initiative Case Studies Local sustainable development solutions for people, nature, and resilient communities UNDP EQUATOR INITIATIVE CASE STUDY SERIES Local and Indigenous communities across the world are solutions (NBS) for climate change and local sustainable advancing innovative sustainable development solutions development. Selected from 847 nominations from across that work for people and for nature. Few publications 127 countries, the winners were celebrated at a gala event or case studies tell the full story of how such initiatives in New York, coinciding with UN Climate Week and the evolve, the breadth of their impacts, or how they change 74th Session of the UN General Assembly. The winners are over time. Fewer still have undertaken to tell these stories sustainably protecting, restoring, and managing forests, with community practitioners themselves guiding the farms, wetlands, and marine ecosystems to mitigate narrative. The Equator Initiative aims to fill that gap. greenhouse gas emissions, help communities adapt to The Equator Initiative, supported by generous funding climate change, and create a green new economy. Since from the German Federal Ministry for Economic 2002, the Equator Prize has been awarded to 245 initiatives. Cooperation and Development (BMZ) and the Norwegian Agency for Development Cooperation (NORAD), awarded The following case study is one in a growing series that the Equator Prize 2019 to 22 outstanding local community describes vetted and peer-reviewed best practices and Indigenous peoples initiatives from 16 countries. Each intended to inspire the policy dialogue needed to of the 22 winners represents outstanding community and scale nature-based solutions essential to achieving the Indigenous initiatives that are advancing nature-based Sustainable Development Goals (SDGs). -

Structural Features Derived from a Multiscale Analysis and 2.75D
https://doi.org/10.5194/se-2020-135 Preprint. Discussion started: 2 September 2020 c Author(s) 2020. CC BY 4.0 License. 1 Structural features derived from a Multiscale Analysis and 2.75D Modelling of 2 Aeromagnetic Data over the Pitoa-Figuil Area (Northern Cameroon) 3 4 5 Voltaire Souga Kassiaa; Theophile Ndougsa Mbargaa,b*;Arsène Meyingc; Jean Daniel Ngoha; Steve 6 Ngoa Embeng a 7 8 aPostgraduate School of Science, Technology and Geosciences, University of Yaoundé I, Yaoundé, Cameroon 9 bDepartment of Physics, Advanced Teacher’s Training College, University of Yaoundé I, P.O. Box 47, Yaoundé, Cameroon c 10 School of Geology and Mining Engineering, University of Ngaoundéré, P.O. Box 115, Meiganga, Cameroon 11 12 Correspondence should be addressed to Ndougsa Mbarga Theophile; *[email protected] 13 14 15 ABSTRACT: 16 In the Pitoa-Figuil area (Northern Cameroon), an interpretation of aeromagnetic data was 17 conducted. The aim of this investigation was first to emphasize lineaments hidden under geological 18 formations and secondly to propose two 2.75D models of the subsurface structures. Different 19 magnetic data processing techniques were used, notably horizontal gradient magnitude, analytic 20 signal, and Euler deconvolution. These techniques in combination with the 2.75D modelling to the 21 aeromagnetic anomaly reduced to the equator permit to understand the stratification of the deep 22 and near surface structures, which are sources of the observed anomalies. We managed to put in 23 evidence and characterize 18 faults and some intrusive bodies. According to Euler’s solutions, 24 anomaly sources go up to a depth of 5.3 km.