September 2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cov-2 Wastewater Surveillance System (Vatar COVID-19) from December 2020 to March
medRxiv preprint doi: https://doi.org/10.1101/2021.05.27.21257918; this version posted May 30, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. All rights reserved. No reuse allowed without permission. Monitoring emergence of SARS-CoV-2 B.1.1.7 Variant through the Spanish National SARS- CoV-2 Wastewater Surveillance System (VATar COVID-19) from December 2020 to March 2021 Albert Carcereny1, Adán Martínez-Velázquez1, Albert Bosch1, Ana Allende2, Pilar Truchado2, Jenifer Cascales2, Jesús L Romalde3, Marta Lois3, David Polo3, Gloria Sánchez4, Alba Pérez- Cataluña4, Azahara Díaz-Reolid4, Andrés Antón5, Josep Gregori6,7, Damir Garcia-Cehic6,7, Josep Quer6,7, Margarita Palau8, Cristina González Ruano9, Rosa M Pintó1#* and Susana Guix1#* 1 Enteric Virus laboratory, Department of Genetics, Microbiology and Statistics, Section of Microbiology, Virology and Biotechnology, School of Biology, and Institute of Nutrition and Food Safety (INSA), University of Barcelona, Barcelona, Spain. 2 Research Group on Microbiology and Quality of Fruit and Vegetables, CEBAS-CSIC, Campus Universitario de Espinardo, 25, 30100, Murcia, Spain. 3 Department of Microbiology and Parasitology, CIBUS-Faculty of Biology & Institute CRETUS, Universidade de Santiago de Compostela, Santiago de Compostela, 15782, Spain. 4 Department of Preservation and Food Safety Technologies, Institute of Agrochemistry and Food Technology, IATA-CSIC, Av. Agustín Escardino 7, Paterna, 46980, Valencia, Spain. 5 Microbiology Department, Vall d'Hebron Institut de Recerca (VHIR), Vall d'Hebron Barcelona Hospital Campus, Passeig Vall d'Hebron 119-129, 08035 Barcelona, Spain. -

Cooperating for a More Competitive, Innovative, Inclusive and Sustainable Mediterranean
COOPERATING FOR A MORE COMPETITIVE, INNOVATIVE, INCLUSIVE AND SUSTAINABLE MEDITERRANEAN Catalogue of the standard projects funded by the ENI CBC ’Mediterranean Sea Basin’ Programme 1 Publisher Managing Authority Regione Autonoma della Sardegna Cagliari, Italy Concept and editing ENI CBC Med Programme Artwork and graphics Begoña Machancoses, Laura Ojeda Printed November 2019 Disclaimer This publication has been produced with the financial assistance of the European Un- ion. Its contents are the sole responsibility of the Managing Authority of the ENI CBC Med Programme and can under no circumstanc- es be regarded as reflecting the position of the European Union. Although every effort is made to ensure the accuracy of the information in this publica- tion, the ENI CBC Med Programme cannot be held responsible for any information from external sources, technical inaccuracies, ty- pographical errors or other errors herein. Information and links may have changed without notice. Reproduction is authorized provided the source is acknowledged. COOPERATING FOR A MORE COMPETITIVE, INNOVATIVE, INCLUSIVE AND SUSTAINABLE MEDITERRANEAN Catalogue of the standard projects funded by the ENI CBC ’Mediterranean Sea Basin’ Programme 3 3. SOCIAL INCLUSION AND FIGHT AGAINST POVERTY 48 3.1 Employability of young people (NEETS) and women 50-55 • HELIOS - enHancing thE sociaL Inclusion Of neetS ....................................................................................................................................... 50 ABOUT THE ENI CBC MED PROGRAMME -

PKF Jordan and Iraq PKF Progroup PKF Khattab & Co
PKF Jordan and Iraq PKF ProGroup PKF Khattab & Co. PKF Planning Tax Advisory PKF Human Resource Consulting Market Overview | Aqaba - Jordan September 2015 PKF Jordan and PKF Iraq are member firms of the PKF International Limited network of legally independent firms and do not accept any responsibility or liability for the actions or inactions on the part of any other individual member firm or firms. Country Overview The Hashemite Kingdom of Jordan has a very strategic location in the heart of the Middle East. It is bounded by Syria from the north, Iraq from the east, Saudi Arabia from the south and southern east and West Bank from the west. Jordan overlooks the Dead Sea from the west and Gulf of Aqaba from south which gives the country a 27 km coastline with the Red Sea. Jordan is a small country with a total area of 89,556 square kilometers. According to the Jordanian Department of Statistics, Jordan’s population reached 6,675,000 in 2014. Jordan had a rising population growth rate of more than 2.2% in 2014. The capital Amman is the biggest city in the country with an estimated population of 2,584,600 in the metropolitan area, therefore forming 38.7% of the country’s population in 2014. Jordan has a vibrant young population, 37.1 percent of the population are less than 14 years old (males form 1,279,370/females form 1,212,090), 59.4 percent are between ages 15 and 64 years (males form 2,052,560/females form 1,915,510) and 3.2 percent are above 65 years (males form 109,070/females form 106,400). -
Standards to Support an Enduring Capability in Wastewater Surveillance for Public Health
DHS/NIST Workshop: Standards to Support an Enduring Capability in Wastewater Surveillance for Public Health Poster Abstracts June 14-18th 2021 Virtual Poster Session https://swwsworkshop.virtualpostersession.org/ CEDAR-MC: Clinical and Environmental Dynamics of Antibiotic Resistance within Microbial Communities George Hanna1,2, Bashir Hamidi1, Scott Curry1, Cheryl Carmack2, Alexander V. Alekseyenko1 1Medical University of South Carolina; 2Charleston Waterkeeper Introduction: Escape into the environment and the persistence of antibiotic resistance is an imminent threat to the healthcare advances attained in the 20th century. Microbial communities that co-exist with resistant bacteria may help uncover novel strategies for global antimicrobial control and curb emergence and maintenance of resistance. However, availability of clinically relevant specimens with complementary samples from the built and natural environment is a major obstacle to effective studies of the dynamics of resistance in the affected human populations and in their surroundings. Methods: We bring together environmental and clinical measurements of the microbial communities with evidence for emerging resistance by linking existing local clinical and environmental surveillance programs. The clinical specimens are sourced from the Medical University of South Carolina (MUSC) infection surveillance culture program that routinely samples the MUSC patient population for clinically relevant pathogens. The environmental specimens are the result of partnership with a local non-profit, -
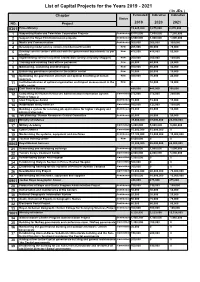
List of Capital Projects for the Years 2019 - 2021 ( in Jds ) Chapter Estimated Indicative Indicative Status NO
List of Capital Projects for the Years 2019 - 2021 ( In JDs ) Chapter Estimated Indicative Indicative Status NO. Project 2019 2020 2021 0301 Prime Ministry 13,625,000 9,875,000 8,870,000 1 Supporting Radio and Television Corporation Projects Continuous 8,515,000 7,650,000 7,250,000 2 Support the Royal Film Commission projects Continuous 3,500,000 1,000,000 1,000,000 3 Media and Communication Continuous 300,000 300,000 300,000 4 Developing model service centers (middle/nourth/south) New 205,000 90,000 70,000 5 Develop service centers affiliated with the government departments as per New 475,000 415,000 50,000 priorities 6 Implementing service recipients satisfaction surveys (mystery shopper) New 200,000 200,000 100,000 7 Training and enabling front offices personnel New 20,000 40,000 20,000 8 Maintaining, sustaining and developing New 100,000 80,000 40,000 9 Enhancing governance practice in the publuc sector New 10,000 20,000 10,000 10 Optimizing the government structure and optimal benefiting of human New 300,000 70,000 20,000 resources 11 Institutionalization of optimal organization and impact measurement in the New 0 10,000 10,000 public sector 0601 Civil Service Bureau 485,000 445,000 395,000 12 Completing the Human Resources Administration Information System Committed 275,000 275,000 250,000 Project/ Stage 2 13 Ideal Employee Award Continuous 15,000 15,000 15,000 14 Automation and E-services Committed 160,000 125,000 100,000 15 Building a system for receiving job applications for higher category and Continuous 15,000 10,000 10,000 administrative jobs. -

Wastewater Based Epidemiology Perspective As a Faster Protocol for Detecting Coronavirus RNA in Human Populations: a Review with Specific Reference to SARS-Cov-2 Virus
pathogens Review Wastewater Based Epidemiology Perspective as a Faster Protocol for Detecting Coronavirus RNA in Human Populations: A Review with Specific Reference to SARS-CoV-2 Virus Milad Mousazadeh 1,2,†,‡ , Razieh Ashoori 3, Biswaranjan Paital 4 , I¸sıkKabda¸slı 5,‡ , Zacharias Frontistis 6 , Marjan Hashemi 7 , Miguel A. Sandoval 8,9,‡ , Samendra Sherchan 10, Kabita Das 11 and Mohammad Mahdi Emamjomeh 12,* 1 Student Research Committee, Qazvin University of Medical Sciences, Qazvin, Iran; [email protected] 2 Department of Environmental Health Engineering, School of Health, Qazvin University of Medical Sciences, Qazvin, Iran 3 Department of Environmental Health Engineering, School of Health, Shiraz University of Medical Sciences, Shiraz, Iran; [email protected] 4 Redox Regulation Laboratory, College of Basic Science and Humanities, Odisha University of Agriculture and Technology, Bhubaneswar 751003, India; [email protected] 5 Environmental Engineering Department, Civil Engineering Faculty, Ayaza˘gaCampus, Istanbul˙ Technical University, Istanbul˙ 34469, Turkey; [email protected] 6 Department of Chemical Engineering, University of Western Macedonia, 50132 Kozani, Greece; Citation: Mousazadeh, M.; Ashoori, [email protected] 7 Environmental and Occupational Hazards Control Research Center, Shahid Beheshti University of Medical R.; Paital, B.; Kabda¸slı,I.; Frontistis, Sciences, Tehran, Iran; [email protected] Z.; Hashemi, M.; Sandoval, M.A.; 8 Laboratorio de Electroquímica Medio Ambiental LEQMA, Departamento -

Wastewater Surveillance Collaborative MOU FINAL
Colorado SARS-CoV-2 Wastewater Surveillance Collaborative Memorandum of Understanding July 2020 Section 1 Background The Colorado Department of Public Health and Environment (Department) is partnering with Colorado State University, Metropolitan State University of Denver (MSU), and 17 Wastewater Utilities to develop a statewide wastewater surveillance system of SARS-CoV-2 RNA, the etiological agent of COVID19. The purpose of the surveillance system is to provide early warning (days to a week) for state and local health authorities of significant changes in fecal shedding of SARS-CoV-2 that could be used in combination with other surveillance efforts and drive action in responding to future COVID19 outbreaks. This testing could also confirm downward trends in COVID-19 outbreaks. With more data and analysis, it may also be useful for predicting community prevalence or to identify potential virus hot spots. Section 2 Purpose This agreement is being entered into by the Memorandum of Understanding (MOU) parties so that roles and responsibilities of each member of the collaborative are understood. The Department has secured $520,000 in funding for this project and this MOU is focused on how those dollars will be leveraged. The effort is scalable and may be expanded through future agreements. The financial obligations under this MOU are contingent upon appropriation, budgeting, and availability of specific funds to discharge those obligations. Nothing in this MOU constitutes a debt, a direct or indirect multiple fiscal year financial obligation or a pledge of a Wastewater Utilities’ credit. Section 3 MOU Parties The following entities are parties to this MOU, individually referred to as Wastewater Utilities, Universities, and Regulatory Agencies. -

Jordan Middle East DISCUSSION PAPER and North Africa Transition Fund September 2017 Middle East and North Africa Transition Fund
Towards a new partnership between government and youth in Jordan Middle East DISCUSSION PAPER and North Africa Transition Fund September 2017 Middle East and North Africa Transition Fund ABOUT THE OECD MENA TRANSITION FUND OF THE DEAUVILLE PARTNERSHIP The Organisation for Economic Co-operation and Development (OECD) is an international body that promotes In May 2011, the Deauville Partnership was launched as a policies to improve the economic and social well-being long-term global initiative that provides Arab countries in of people around the world. It is made up of 35 member transition with a framework based on technical support countries, a secretariat in Paris, and a committee, drawn to strengthen governance for transparent, accountable from experts from government and other fields, for each governments and to provide an economic framework for work area covered by the organisation. The OECD provides sustainable and inclusive growth. a forum in which governments can work together to share experiences and seek solutions to common problems. We The Deauville Partnership has committed to support collaborate with governments to understand what drives Egypt, Jordan, Libya, Morocco, Tunisia and Yemen and the economic, social and environmental change. We measure Transition Fund is one of the levers to implement this productivity and global flows of trade and investment. commitment. The Transition Fund demonstrates a joint commitment by G7 members, Gulf and regional partners, For more information, please visit www.oecd.org. and international and regional financial institutions to support the efforts of the people and governments of the Partnership countries as they overhaul their economic systems to promote more accountable governance, broad- based, sustainable growth, and greater employment opportunities for youth and women. -

Amman, Jordan
MINISTRY OF WATER AND IRRIGATION WATER YEAR BOOK “Our Water situation forms a strategic challenge that cannot be ignored.” His Majesty Abdullah II bin Al-Hussein “I assure you that the young people of my generation do not lack the will to take action. On the contrary, they are the most aware of the challenges facing their homelands.” His Royal Highness Hussein bin Abdullah Imprint Water Yearbook Hydrological year 2016-2017 Amman, June 2018 Publisher Ministry of Water and Irrigation Water Authority of Jordan P.O. Box 2412-5012 Laboratories & Quality Affairs Amman 1118 Jordan P.O. Box 2412 T: +962 6 5652265 / +962 6 5652267 Amman 11183 Jordan F: +962 6 5652287 T: +962 6 5864361/2 I: www.mwi.gov.jo F: +962 6 5825275 I: www.waj.gov.jo Photos © Water Authority of Jordan – Labs & Quality Affairs © Federal Institute for Geosciences and Natural Resources Authors Thair Almomani, Safa’a Al Shraydeh, Hilda Shakhatreh, Razan Alroud, Ali Brezat, Adel Obayat, Ala’a Atyeh, Mohammad Almasri, Amani Alta’ani, Hiyam Sa’aydeh, Rania Shaaban, Refaat Bani Khalaf, Lama Saleh, Feda Massadeh, Samah Al-Salhi, Rebecca Bahls, Mohammed Alhyari, Mathias Toll, Klaus Holzner The Water Yearbook is available online through the web portal of the Ministry of Water and Irrigation. http://www.mwi.gov.jo Imprint This publication was developed within the German – Jordanian technical cooperation project “Groundwater Resources Management” funded by the German Federal Ministry for Economic Cooperation and Development (BMZ) Implemented by: Foreword It is highly evident and well known that water resources in Jordan are very scarce. -

History of the Discovery of Hepatitis a Virus
Downloaded from http://perspectivesinmedicine.cshlp.org/ on October 1, 2021 - Published by Cold Spring Harbor Laboratory Press History of the Discovery of Hepatitis A Virus Stephen M. Feinstone Department of Biochemistry and Molecular Medicine, George Washington University School of Medicine, Washington, D.C. 20037 Correspondence: [email protected] Disease outbreaks resembling hepatitis A have been known since antiquity. However, it was not until World War II when two forms of viral hepatitis were clearly differentiated. After the discovery of Australia antigen and its association with hepatitis B, similar method- ologies were used to find the hepatitis A virus. The virus was ultimately identified when investigators changed the focus of their search from serum to feces and applied appropriate technology. iseases resembling hepatitis A, both in DIFFERENTIATION OF TWO FORMS OF Dindividuals and in outbreaks involving VIRAL HEPATITIS groups, were reported in China as early as 5000 years ago. Hippocrates noted a disease Viral hepatitis was a major problem for both the he called benign epidemic jaundice in “De Allies and the Axis during World War II. Early Morbis Internis” that certainly resembled hep- in the war, an outbreak of hepatitis related to atitis A. More accurate descriptions of hepatitis yellow fever vaccine, stabilized with human se- A began appearing in the 17th century often rum involving 49,233 clinically apparent cases associated with military campaigns. The first (Seeff et al. 1987), prompted a major hepatitis outbreak recorded in the United States was research effort. As the records on the vaccinees in 1812 in Norfolk, VA, and the disease was were very good, the incubation period was de- common among the Union troops during fined accurately as between 60 and 154 days. -

KLİMUD E-Bülten Aralık 2020
e- BÜLTEN Aralık 2020 Kapak Resmi : TUTUKLULAR ÇEMBERİ Vincent Van Gogh (http://art - vangogh.com/saint -remy_121.html) 1 Acı Kaybımız Duayen hocamız, çok kıymetli bilim insanı, Ülkemizde İmmünoloji, Viral Hepatitler, Kan Bankacılığı ve Transfüzyon Tıbbı alan- larında ilklere imza atan, eski Sağlık Bakanı Prof. Dr. Kaya Kılıçturgay’ın aramızdan ay- rılması hepimizi üzmüştür. Yazdığı kitaplarıyla, kurucusu olduğu derneklerle ve gençle- rin önünü açtığı çalışmalarıyla unutulmaz değerlerimiz ara- sında yerini alan “hocaların hocası” Prof. Dr. Kaya Kılıçtur- gay Türkiye’de bilimin kurumsallaşmasına ve toplumsal ya- şama katılmasına katkılarıyla daima anımsanacaktır. Prof.Dr Kaya Kılıçturgay foroğraflarını bizimle paylaşan Prof. Dr.Ahmet Başustaoğlu’na teşekkür ederiz 2 Bu Sayıda Öne Çıkanlar e - B Ü LT E N Ayın Portresi Aralık 2020 June Almeida Sevgili okurlar Dergi Saati COVID-19 ve Doğru Risk Kontrol Sıradışı bir yılı yaşadık hep birlikte… Yorulduk, sıkıldık, bunaldık, üzüldük hep birlikte... Stratejileri İhtiyacı Bu zor günlerde Klimud e-Bülten’ in hepimize bir soluk alma, bir rahatlama fırsatı sunmuş ol- Edebiyat ve Mikrobiyoloji masını diliyoruz. Shakespeare’in Öksürüğü Geçen sayımızda başlattığımız Ayın Portresi’nde koronavirüsleri ilk kez elektron mikrosko- bu ile görüntüleyen ve isimlendiren June Almedia’nın öyküsünü arkadaşımız Bilge Dikenel- Orwell’in Titremesi li’nin kaleminden sunuyoruz sizlere. İki yıldır kesintisiz paylaştığımız sayfalarımız Edebiyat Fotoğrafhane ve Mikrobiyoloji, Fotoğrafhane, SineMikrop ‘ta ilginizi çekecek içerikler var yine. Platon ve Mağara Allegorisi Bu güne kadar bültenimizde paylaşım yapan tüm meslektaşlarımıza, katkılarını esirgemeyen SineMikrop tüm dostlarımıza en içten teşekkürlerimizi sunarız. Çiçek Hastalığı 2002: Yeni sayılarımızda ekibimizin genişleyerek büyümesi en büyük arzumuz. 2021 yılından bek- lentimiz ise yeni yılın hepimiz için daha umutlu, daha mutlu, daha sağlıklı günlere kapı aç- Sessiz Silah masını diliyoruz. -

Medical Virology of Hepatitis B: How It Began and Where We Are Now Wolfram H Gerlich
Gerlich Virology Journal 2013, 10:239 http://www.virologyj.com/content/10/1/239 REVIEW Open Access Medical Virology of Hepatitis B: how it began and where we are now Wolfram H Gerlich Abstract Infection with hepatitis B virus (HBV) may lead to acute or chronic hepatitis. HBV infections were previously much more frequent but there are still 240 million chronic HBV carriers today and ca. 620,000 die per year from the late sequelae liver cirrhosis or hepatocellular carcinoma. Hepatitis B was recognized as a disease in ancient times, but its etiologic agent was only recently identified. The first clue in unraveling this mystery was the discovery of an enigmatic serum protein named Australia antigen 50 years ago by Baruch Blumberg. Some years later this was recognized to be the HBV surface antigen (HBsAg). Detection of HBsAg allowed for the first time screening of inapparently infected blood donors for a dangerous pathogen. The need to diagnose clinically silent HBV infections was a strong driving force in the development of modern virus diagnostics. HBsAg was the first infection marker to be assayed with a highly sensitive radio immune assay. HBV itself was among the first viruses to be detected by assay of its DNA genome and IgM antibodies against the HBV core antigen were the first to be selectively detected by the anti-μ capture assay. The cloning and sequencing of the HBV genome in 1978 paved the way to understand the viral life cycle, and allowed development of efficient vaccines and drugs. Today’s hepatitis B vaccine was the first vaccine produced by gene technology.