Circle ONLY the Most Appropriate Answer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
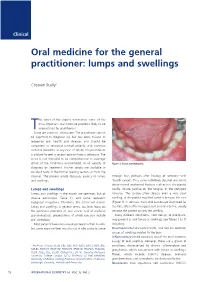
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

Applications of Cytokeratin Expression in the Diagnosis of Oral Diseases
Jemds.com Review Article Applications of Cytokeratin Expression in the Diagnosis of Oral Diseases Archana Sonone1, Alka Hande2, Madhuri Gawande3,Swati Patil4 1, 2, 3, 4 Department of Oral Pathology and Microbiology, Sharad Pawar Dental College, Datta Meghe Institute of Medical Sciences (Deemed to Be University) Sawangi (Meghe), Wardha, Maharashtra, India. ABSTRACT All mammalian cells have a complex intracytoplasmic cytoskeleton made up of three Corresponding Author: main structural units and related proteins, tubulin containing microtubules, actin Dr. Archana Sonone. Department of Oral Pathology and containing microfilaments, and Intermediate Filaments (IF). There are six types of Microbiology, Sharad Pawar Dental IFs; cytokeratin fibres consisting of type I and type II IFs. Cytokeratins (CK), College, Datta Meghe Institute of Medical . comprising of collections of IFs that are explicitly communicated by epithelial tissues Sciences (Deemed to Be University) There are 20 unique polypeptides of CK expressed by epithelium that have been Sawangi (Meghe), Wardha, Maharashtra, indexed based on their molecular weight (range 40-70 kDa). India. CK and associated filaments give a framework to epithelial cells and tissues to E-mail: [email protected] maintain their structural integrity. Thus, ensure mechanical resilience, sustain stress, establish cell polarity, and to protect against variations in hydrostatic pressure. DOI: 10.14260/jemds/2021/50 Genetic encoding of cytokeratins shows homogeneous “nucleotide sequence”. 54 How to Cite This Article: genes are responsible for encoding of cytokeratin in humans which are congregated Sonone A, Hande A, Gawande M, et al. on chromosome no. 2. Genetic mutation of cytokeratins is important for Applications of cytokeratin expression in pathophysiology of various mucocutaneous disorders, which is mostly autosomal the diagnosis of oral diseases. -

Benign Cementoblastoma Associated with an Impacted Mandibular Third Molar – Report of an Unusual Case
Case Report Benign Cementoblastoma Associated with an Impacted Mandibular Third Molar – Report of an Unusual Case Chethana Dinakar1, Vikram Shetty2, Urvashi A. Shetty3, Pushparaja Shetty4, Madhvika Patidar5,* 1,3Senior Lecturer, 4Professor & HOD, Department of Oral Pathology and Microbiology, AB Shetty Memorial Institute of Dental Science, Mangaloge, 2Director & HOD, Nittee Meenakshi Institute of Craniofacial Surgery, Mangalore, 5Senior Lecturer, Department of Oral Pathology and Microbiology, Babu Banarasi Das College of Dental Sciences, Lucknow *Corresponding Author: Email: [email protected] ABSTRACT Cementoblastoma is characterized by the formation of cementum-like tissue in direct connection with the root of a tooth. It is a rare lesion constituting less than 1% of all odontogenic tumors. We report a unique case of a large cementoblastoma attached to the lateral root surface of an impacted permanent mandibular third molar in a 33 year old male patient. The association of cementoblastomas with impacted teeth is a rare finding. Key Words: Odontogenic tumor, Cementoblastoma, Impacted teeth, Third molar, Cementum Access this article online opening limited to approximately 10mm. The swelling Quick Response was firm to hard in consistency and tender on palpation. Code: Website: Lymph nodes were not palpable. www.innovativepublication.com On radiographical examination, it showed a large, well circumscribed radiopaque mass attached to the lateral root surface of impacted permanent right mandibular DOI: 10.5958/2395-6194.2015.00005.3 third molar. The mass displayed a radiolucent area at the other end and was seen occupying almost the entire length of the ramus of mandible. The entire lesion was INTRODUCTION surrounded by a thin, uniform radiolucent line (Fig. -

Management of Anterior Spacing with Peg Lateral by Interdisciplinary Approach : a Case Report
Case Report Management of Anterior Spacing with Peg Lateral by Interdisciplinary Approach : A Case Report Dr Sanjay Prasad Gupta Assistant Professor & Consultant Orthodontist, Department of Orthodontics, Tribhuvan University Teaching Hospital, Institute of Medicine, Kathmandu Correspondence: Dr Sanjay Prasad Gupta; Email: [email protected] ABSTRACT Anterior spacing is a common esthetic problem of patient during dental consultation. The most common etiology include tooth size and arch length discrepancy. Maxillary lateral incisors vary in form more than any other tooth in the mouth except the third molars. Microdontia is a condition where the teeth are smaller than the normal size. Microdontia of maxillary lateral incisor is called as “peg lateral”, that exhibit converging mesial and distal surfaces of crown forming a cone like shape. A carefully documented diagnosis and treatment plan are essential if the clinician is to apply the most effective approach to address the patient’s needs. A patient sometimes requires a multidisciplinary approach to correct the esthetics and to improve the occlusion. This case report describes the management of an adult female patient with a proclined upper anterior teeth, upper anterior spacing, deep bite and peg shaped upper right lateral incisor tooth through orthodontic and restorative treatment approach. Key words: Anterior spacing, Peg lateral, Esthetic, Interdisciplinary approach INTRODUCTION Peg shaped lateral incisors occur in approximately 2% to 5% of the general population, and women show a Maxillary lateral incisors vary in form more than any slightly higher frequency than men. Usually they are found other tooth in the mouth except the third molars. If the equally on the right and left, uni or bilaterally, however variation is too great, it is considered a developmental some studies have shown their bilateral occurrence anomaly.1 Developmental alterations which are most slightly higher than the unilateral occurrence. -

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Permanent Mandibular Incisor with Multiple Anomalies - Report of a Rare Clinical Case
Braz346 Dent J (2011) 22(4): 346-350 N. B. Nagaveni et al. ISSN 0103-6440 Permanent Mandibular Incisor with Multiple Anomalies - Report of a Rare Clinical Case Nayaka Basavanthappa NAGAVENI1 Kagathur Veerbadrapa UMASHANKARA2 B.G. VIDYULLATHA3 SREEDEVI3 Nayaka Basavanthappa RADHIKA4 1Department of Pedodontics and Preventive Dentistry, Hitkarini Dental College and Hospital, Jabalpur, Madhya Pradesh, India 2Department of Oral and Maxillofacial Surgery, Hitkarini Dental College and Hospital, Jabalpur, Madhya Pradesh, India 3Department of Oral Medicine and Radiology, Hitkarini Dental College and Hospital, Jabalpur, Madhya Pradesh, India 4Department of Orthodontics and Dentofacial Orthopedics, School of Dentistry, Krishna Institute of Medical Sciences, Satara district, Karad, Maharashtra, India Permanent mandibular central incisor is rarely affected by tooth shape anomalies of crown and root. Co-occurrence of multiple anomalies in a permanent mandibular central incisor is extremely rare. This paper reports an unusual concurrent combination of multiple dental anomalies affecting both the crown and root of a permanent mandibular left central incisor - talon cusp, dens invaginatus, short root anomaly and macrodontia -, which has not previously been reported together. Case management is described and implications are discussed. The dentist should be aware of these rare entities in order to provide an accurate diagnosis and management for which detailed examination of the tooth both clinically and radiographically is very important. Key Words: anomalies, dens invaginatus, mandibular incisor, short root anomaly, talon cusp. INTRODUCTION differentiation stage of tooth development (2). Dens invaginatus is also a rare developmental Morphological variations of dental structure anomaly defined as a deep surface invagination of the involving either crown or root are common in the crown or root, which is lined by enamel and resulting literature. -

Analysis of the Association of Foramen Cecum and Dens in Dente in Maxillary Lateral Incisor
Published online: 2020-10-05 THIEME 242 OriginalAssociation Article of Foramen Cecum and Dens in Dente Genaro et al. Analysis of the Association of Foramen Cecum and Dens in Dente in Maxillary Lateral Incisor Luis Eduardo Genaro1 Marcelo Brito Conte1 Giovana Anovazzi1 Andréa Gonçalves2 1 1 Marcela de Almeida Gonçalves Ticiana Sidorenko de Oliveira Capote 1Department of Morphology, Genetics, Orthodontic and Pediatric Address for correspondence Luis Eduardo Genaro, DDS, Dentistry, School of Dentistry, São Paulo State University, Department of Morphology, Genetics, Orthodontic and Pediatric Araraquara, São Paulo, Brazil Dentistry, School of Dentistry, São Paulo State University (UNESP), 2Department of Diagnosis and Surgery, School of Dentistry, São Rua Humaitá, 1680, 14801-903 Araraquara, SP, Brazil Paulo State University, Araraquara, São Paulo, Brazil (e-mail: [email protected]). Eur J Dent 2021;15:242–246 Abstract Objectives The aim of this study was to evaluate the frequency of foramen cecum and dens in dente, and to verify the association of these structures in the maxillary lateral incisor (MLI). Materials and Methods The presence of foramen cecum in the lingual surface of 110 MLI was verified, and the teeth were radiographed to observe the presence of dens in dente, being classified according to the literature. An association study between the presence of foramen cecum and dens in dente was performed using the Cramer’s V and chi-square statistical tests. Results The association was statistically significant between the foramen cecum and the dens in dente. Concomitant presence was observed in 17.27%, being a high rate when compared with the presence of foramen cecum alone (9.09%) or dens in dente alone (8.18%). -

Misdiagnosis of Osteosarcoma As Cementoblastoma from an Atypical Mandibular Swelling: a Case Report
ONCOLOGY LETTERS 11: 3761-3765, 2016 Misdiagnosis of osteosarcoma as cementoblastoma from an atypical mandibular swelling: A case report ZAO FANG1*, SHUFANG JIN1*, CHENPING ZHANG1, LIZHEN WANG2 and YUE HE1 1Department of Oral Maxillofacial Head and Neck Oncology, Faculty of Oral and Maxillofacial Surgery; 2Department of Oral Pathology, Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai Key Laboratory of Stomatology, Shanghai 200011, P.R. China Received December 1, 2014; Accepted January 12, 2016 DOI: 10.3892/ol.2016.4433 Abstract. Cementoblastoma is a form of benign odontogenic of the lesion with extraction of the associated tooth (2); tumor, with the preferred treatment consisting of tooth extrac- however, certain patients may decide against surgery, under- tion and follow-up examinations, while in certain cases, going follow-up alone. Osteosarcoma is a non-hematopoietic, follow-up examinations without surgery are performed. malignant tumor of the bone, with the neoplastic cells of the Osteosarcoma of the jaw is a rare, malignant, mesenchymal lesion producing osteoid (3). This form of tumor is character- tumor, associated with a high mortality rate and low incidence ized by high malignancy, metastasis and mortality rates (4). of metastasis. Cementoblastoma and osteosarcoma of the jaw The tumors are most prevalently located in the metaphyseal are dissimilar in terms of their histological type and prognosis; region of long bones, particularly in the knee and pelvis (5). however, there are a number of covert associations between Osteosarcoma of the jaw is rare, accounting for 5-13% of all them. The present study describes the case of a 20-year-old osteosarcoma cases (6), the majority of which are located in female with an unusual swelling in the left mandible that the mandible. -

WHAT HAPPENED? CDR, a 24-Year-Old Chinese Male
CHILDHOOD DEVELOPMENTAL SCREENING 2020 https://doi.org/10.33591/sfp.46.5.up1 FINDING A MASS WITHIN THE ORAL CAVITY: WHAT ARE THE COMMON CAUSES AND 4-7 GAINING INSIGHT: WHAT ARE THE ISSUES? In Figure 2 below, a list of masses that could arise from each site Figure 3. Most common oral masses What are the common salivary gland pathologies Salivary gland tumours (Figure 7) commonly present as channel referrals to appropriate specialists who are better HOW SHOULD A GP MANAGE THEM? of the oral cavity is given and elaborated briey. Among the that a GP should be aware of? painless growing masses which are usually benign. ey can equipped in centres to accurately diagnose and treat these Mr Tan Tai Joum, Dr Marie Stella P Cruz CDR had a slow-growing mass in the oral cavity over one year more common oral masses are: torus palatinus, torus occur in both major and minor salivary glands but are most patients, which usually involves surgical excision. but sought treatment only when he experienced a sudden acute mandibularis, pyogenic granuloma, mucocele, broma, ere are three pairs of major salivary glands (parotid, commonly found occurring in the parotid glands. e most 3) Salivary gland pathology may be primary or secondary to submandibular and sublingual) as well as hundreds of minor ABSTRACT onset of severe pain and numbness. He was fortunate to have leukoplakia and squamous cell carcinoma – photographs of common type of salivary gland tumour is the pleomorphic systemic causes. ese dierent diseases may present with not sought treatment as it had not caused any pain. -
Mandibular Tori
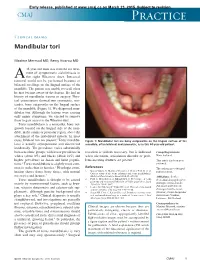
Early release, published at www.cmaj.ca on March 23, 2015. Subject to revision. CMAJ Practice Clinical images Mandibular tori Maxime Mermod MD, Remy Hoarau MD 44-year-old man was referred for treat- ment of symptomatic sialolithiasis in A the right Wharton duct. Intraoral removal could not be performed because of bilateral swellings on the lingual surface of the mandible. The patient was unable to recall when he first became aware of the lesions. He had no history of mandibular trauma or surgery. Phys- ical examination showed two symmetric, non- tender, bony outgrowths on the lingual surface of the mandible (Figure 1). We diagnosed man- dibular tori. Although the lesions were causing only minor symptoms, we elected to remove them to gain access to the Wharton duct. Torus mandibularis is a nontender, bony out- growth located on the lingual side of the man- dible, in the canine or premolar region, above the attachment of the mylohyoid muscle. In most 1 cases, bilateral tori are present. Torus mandibu- Figure 1: Mandibular tori are bony outgrowths on the lingual surface of the laris is usually asymptomatic and discovered mandible, often bilateral and symmetric, as in this 44-year-old patient. incidentally. The prevalence varies substantially between ethnic groups, with lower prevalence in resection is seldom necessary, but is indicated Competing interests: whites (about 8%) and blacks (about 16%) and when ulceration, articulation disorder or prob- None declared. higher prevalence in Asian and Inuit popula- lems inserting dentures are present.3 This article has been peer tions.2 Torus mandibularis is slightly more com- reviewed. -

Abscesses Apicectomy
BChD, Dip Odont. (Mondchir.) MBChB, MChD (Chir. Max.-Fac.-Med.) Univ. of Pretoria Co Reg: 2012/043819/21 Practice.no: 062 000 012 3323 ABSCESSES WHAT IS A TOOTH ABSCESS? A dental/tooth abscess is a localised acute infection at the base of a tooth, which requires immediate attention from your dentist. They are usually associated with acute pain, swelling and sometimes an unpleasant smell or taste in the mouth. More severe infections cause facial swelling as the bacteria spread to the nearby tissues of the face. This is a very serious condition. Once the swelling begins, it can spread rapidly. The pain is often made worse by drinking hot or cold fluids or biting on hard foods and may spread from the tooth to the ear or jaw on the same side. WHAT CAUSES AN ABSCESS? Damage to the tooth, an untreated cavity, or a gum disease can cause an abscessed tooth. If the cavity isn’t treated, the inside of the tooth can become infected. The bacteria can spread from the tooth to the tissue around and beneath it, creating an abscess. Gum disease causes the gums to pull away from the teeth, leaving pockets. If food builds up in one of these pockets, bacteria can grow, and an abscess may form. An abscess can cause the bone around the tooth to dissolve. WHY CAN'T ANTIBIOTIC TREATMENT ALONE BE USED? Antibiotics will usually help the pain and swelling associated with acute dental infections. However, they are not very good at reaching into abscesses and killing all the bacteria that are present. -

Dental Anomalies: Foundational Articles and Consensus Recommendations, 2021
Dental Anomalies: Foundational Articles and Consensus Recommendations, 2021 Adekoya-Sofowora CA. Natal and neonatal teeth: a review. Niger Postgrad Med J 2008;15:38-41 Al-Ani AH, Antoun JS, Thomson WM, Merriman TR, Farella M. Hypodontia: An Update on Its Etiology, Classification, and Clinical Management. Biomed Res Int. 2017:9378325. doi.org/10.1155/2017/9378325. Anthonappa RP, King NM, Rabie AB. Aetiology of supernumerary teeth: A literature review. Eur Arch Paediatr Dent. 2013;14:279-88. Dashash, M. Yeung CA, Jamous I, Blinkhorn A. Interventions for the restorative care of amelogenesis imperfecta in children and adolescents. Cochrane Database Syst Rev 2013;6:CD007157. Gallacher A, Ali R, Bhakta S. Dens invaginatus: diagnosis and management strategies. Br Dent J 2016;221:383-7. Gill DS, Barker CS. The multidisciplinary management of hypodontia: a team approach. Br Dent J 2015;218:143-9. Khalaf K, Miskelly J, Voge E, Macfarlane TV. Prevalence of hypodontia and associated factors: a systematic review and meta-analysis. J Orthod. 2014; 41:299-316. Lammi L. Arte S, Somer M, Javinen H, et al. Mutations in AXIN2 cause familial tooth agenesis and predispose to colorectal cancer. Am. J. Hum. Genet. 2004, 74:1043–1050. Marvin ML, Mazzoni S, Herron CM, Edwards S, et al. AXIN2-associated autosomal dominant ectodermal dysplasia and neoplastic syndrome. Am J Med Genet A. 2011,155 898–902. Seow WK. Developmental defects of enamel and dentine: Challenges for basic science research and clinical management. Aust Dent J 2014;59:143-54. Shields ED, Bixler D, El-Kafrawy AM. A proposed classification for heritable human dentine defects with a description of a new entity.