Morbidity and Mortality
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Presented on Selected Characterstics of Minority Persons in Houston and Parts of Harris County
DOCUMENT RESUME ED 094 023 UD 014 334 AUTHOR Lede, Naomi W.; Dixon, Hortense W. TITLE Urban Minority Groups in Houston: Problems, Progress, and Prospects. A Statistical and Analytical Study. INSTITUTION Texas Southern Univ., Houston. Urban Resources Center. SPONS AGENCY Departm.ant of Housing and Urban Development, Washington, D.C. PUB DATE 29 Mar 73 NOTE 468p.; Charts on pages 146-163 of this document will not be clearly legible due to print size in the original EDRS P:ICE MF-$0.75 HC-$22.20 PLUS POSTAGE DESCRIPTORS Age Groups; *City Demography; Economically . Disadvantaged; Employment Statistics; Family Income; High School Graduates; Marital Status; *Minority Groups; Populatico Trends; Racial Distribution; Socioeconomic Status; *Statistical Analysis; *Urban Population IDENTIFIERS *Texas ABSTRACT This document is cne of a series about the conditions of blacks and other minorities f.L. Houston, Texas. Statistics are presented on selected characterstics of minority persons in Houston and parts of Harris County. document is designed to provide data in an organized and systematic *.:ay by bringing together in one convenient source socioeconomic facts about the minority community and by keeping the document constantly up to date through more current reports. Data for the central, city and some suburban rings in close proximity to Houston proper are given when this type of distinction appears to be significant. The major areas treated in this report are: general socioeconomic characteristics, populetip.n and distribution, family and household size, education, employment and income, housing, poverty, politics, health, economic develippment statistics, and other pertinent data on minority problems and accomplishments. The preparation of the volume was guided by three major concerns: the assessment of problems; a review of progress or accomplishments in the light of civil rights legislation; and a general projection of future needs and prospects. -

Halve the Gap by 2030: Youth Disconnection in America's Cities
HALVE THE GAP YOUTH DISCONNECTION BY 2030 IN AMERICA’S CITIES KRISTEN LEWIS and SARAH BURD-SHARPS 2013 GAP: 30.3 2013 GAP: (PERCENTAGE POINTS) (PERCENTAGE 15.7 GAP IN YOUTH DISCONNECTION RATE RATE DISCONNECTION IN YOUTH GAP 2030 2030 TARGET: TARGET: 7.9 15.2 Racial/ethnic groups Neighborhood clusters Patrick Nolan Guyer | CHIEF STATISTICIAN & CARTOGRAPHER Diana Tung | REPORT DESIGN TO DOWNLOAD THIS REPORT, PLEASE VISIT MEASURE OF AMERICA WWW.MEASUREOFAMERICA.ORG/HALVE-THE-GAP-2030 of the Social Science Research Council Contents Overview..........................................................……………………………………………………………….........3 Introduction..................................……........…..….………………………………………………………………………....5 What Do the Numbers Show?.................................................................………........…………………….....11 Factors Associated with Youth Disconnection..........................................................…………………....19 The Way Forward.................................................................……………………………………….…………….....23 Metro Area Close-Ups….....……………………………….………………………....................................................30 1. Boston 14. New York 2. Minneapolis–St. Paul 15. Los Angeles 3. Washington, DC 16. Dallas–Ft. Worth 4. San Diego 17. San Antonio 5. San Francisco 18. Tampa–St. Petersburg 6. Pittsburgh 19. Miami 7. Denver 20. Atlanta 8. Seattle 21. Portland 9. Chicago 22. Phoenix 10. Houston 23. Charlotte 11. St. Louis 24. Detroit 12. Philadelphia 25. Riverside–San Bernardino 13. Baltimore Endnotes…..………………………………………………………......................................................................105 -

Local Identities Global Challenges
THE ROLE OF THE MEXICAN AMERICAN COMMUNITY 63 The Role of the Mexican American Community in the Production of Urban Space in Houston, Texas BARRY ESPINOSA-OROPEZA Universitat Politècnica de Catalunya Houston is the fourth largest metropolitan area in our urban settlements are organized and built, in- the United States. It is also one of the most cultural- forming how different social groups (in terms of ly diverse cities in America. As such, Houston can be race, culture, ethnicity, gender, age, etc.) relate to presented as a paradigm of the twenty-first century space. Yet, among urban researchers there are dif- multicultural city in the United States. Yet Houston ferent views as to how this relation occurs. Some, remains largely understudied1, in particular, with re- for example, view it as a cause and effect situation, lation to the way ethnic and cultural minorities par- where social structure is the cause and spatial con- ticipate in the production of its urban space. This figuration is the effect. Others believe this spatial research is intended to help fill this gap, focusing configuration to be more the aggregate result of in- in one of the largest ethnic groups in Houston, the dividual decisions. Given the brevity of this paper, Mexican-American population. For this purpose, I and the extensive research already existing, I will conduct a socio-semiotic analysis of one of the old- not go into detail on these subjects.3 Yet, I would est Mexican neighborhoods in the city: ‘El Segundo like to comment, if only briefly, on a third viewpoint: Barrio’. -

Fifth Ward and Denver Harbor: Black and Brown Conflict, Solidarity, and Shared Oppression in East Houston
San Jose State University SJSU ScholarWorks NACCS Annual Conference Proceedings 2012: 39th Annual: NACCS@40 - Chicago, IL Mar 15th, 5:00 AM - 7:00 AM Fifth Ward and Denver Harbor: Black and Brown Conflict, Solidarity, and Shared Oppression in East Houston Stephanie Arguera University of Texas at San Antonio Follow this and additional works at: https://scholarworks.sjsu.edu/naccs Part of the Gender and Sexuality Commons, and the Race and Ethnicity Commons Arguera, Stephanie, "Fifth Ward and Denver Harbor: Black and Brown Conflict, Solidarity, and Shared Oppression in East Houston" (2012). NACCS Annual Conference Proceedings. 6. https://scholarworks.sjsu.edu/naccs/2012/Proceedings/6 This Conference Proceeding is brought to you for free and open access by the National Association for Chicana and Chicano Studies Archive at SJSU ScholarWorks. It has been accepted for inclusion in NACCS Annual Conference Proceedings by an authorized administrator of SJSU ScholarWorks. For more information, please contact [email protected]. Fifth Ward and Denver Harbor 1 Fifth Ward and Denver Harbor: Black and Brown Conflict, Solidarity, and Shared Oppression in East Houston Stephanie Arguera University of Texas at San Antonio Fifth Ward and Denver Harbor 2 Connecting the Dots: A self-awareness Like every other morning at 7:45AM, the concrete, slender hallways of my elementary school were crammed with tiny chattering learners from beige brick to beige brick. In my uninspired navy dress and white polo uniform, I inched into a corridor packed with my schoolmates on my way to class, becoming one with the sea of dark, blurry faces in matching low-cost garb. -
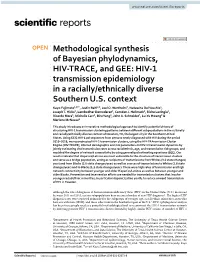
HIV-1 Transmission Epidemiology in a Racially/Ethnically
www.nature.com/scientificreports OPEN Methodological synthesis of Bayesian phylodynamics, HIV‑TRACE, and GEE: HIV‑1 transmission epidemiology in a racially/ethnically diverse Southern U.S. context Kayo Fujimoto1,9*, Justin Bahl2,9, Joel O. Wertheim3, Natascha Del Vecchio4, Joseph T. Hicks2, Lambodhar Damodaran5, Camden J. Hallmark6, Richa Lavingia1, Ricardo Mora6, Michelle Carr6, Biru Yang6, John A. Schneider7, Lu‑Yu Hwang8 & Marlene McNeese6 This study introduces an innovative methodological approach to identify potential drivers of structuring HIV‑1 transmission clustering patterns between diferent subpopulations in the culturally and racially/ethnically diverse context of Houston, TX, the largest city in the Southern United States. Using 6332 HIV‑1 pol sequences from persons newly diagnosed with HIV during the period 2010–2018, we reconstructed HIV‑1 transmission clusters, using the HIV‑TRAnsmission Cluster Engine (HIV‑TRACE); inferred demographic and risk parameters on HIV‑1 transmission dynamics by jointly estimating viral transmission rates across racial/ethnic, age, and transmission risk groups; and modeled the degree of network connectivity by using generalized estimating equations (GEE). Our results indicate that Hispanics/Latinos are most vulnerable to the structure of transmission clusters and serve as a bridge population, acting as recipients of transmissions from Whites (3.0 state changes/ year) and from Blacks (2.6 state changes/year) as well as sources of transmissions to Whites (1.8 state changes/year) and to Blacks (1.2 state changes/year). There were high rates of transmission and high network connectivity between younger and older Hispanics/Latinos as well as between younger and older Blacks. Prevention and intervention eforts are needed for transmission clusters that involve younger racial/ethnic minorities, in particular Hispanic/Latino youth, to reduce onward transmission of HIV in Houston. -

Houston Facts 2019 Are Current As of June ’19 Unless Otherwise Noted
HOUSTON 2019 GREATERFACTS HOUSTON PARTNERSHIP Discover the Houston Region The facts speak for themselves. Austin | Brazoria | Chambers | Fort Bend | Galveston | Harris | Liberty | Montgomery | San Jacinto | Walker | Waller HOUSTONFACTS About the Greater Houston Partnership The mission of the Greater Houston Partnership is to make Houston one of the world’s best places to live, work and build a business. The Partnership works to make Houston greater by promoting economic development, foreign trade and investment, and by advocating for efficient and effective government that supports, rather than impedes, business growth. The Partnership also convenes key stakeholders to solve the region’s most pressing issues. The Partnership was formed in 1989 in a merger of the Greater Houston Chamber of Commerce, the Houston Economic Development Council and the Houston World Trade Association. Today, the Partnership serves the 11-county greater Houston region and represents a member roster of more than 1,000 businesses and institutions. Members of the Partnership account for one-fifth of all jobs in Houston. They engage in various initiatives, committees and task forces to work toward our goal of making Houston greater. GREATER HOUSTON PARTNERSHIP | 701 AVENIDA DE LAS AMERICAS, SUITE 900 | HOUSTON, TX 77010 713-844-3600 | HOUSTON.ORG © 2019 Greater Houston Partnership Data in Houston Facts 2019 are current as of June ’19 unless otherwise noted. Houston Facts is a registered trademark of the Greater Houston Partnership. Houston Facts 2019 was compiled by the research team of the Greater Houston Partnership, including Elizabeth Balderrama, Patrick Jankowski, Roel Gabe Martinez, Josh Pherigo, Nadia Valliani and Melissa Verhoef. This publication was designed by Marc Keosayian and Suzanne Morgan. -
2008 the City of Houston Health Disparities Data Report
The City of Houston Health Disparities Data Report March 2008 The City of Houston Health Disparities Data Report 2008 Cover photos are courtesy of the U.S. Census Bureau. © 2008 by the City of Houston. All rights reserved. In recognition of contemporary needs of researchers/information providers and users in a globally connected information of cybersystem, we require that the following conditions be met when reusing this material: Include this standard copyright line: © 2008 by the City of Houston. If placed on a Web site, include this hyperlink/hot link to: www.houston.tx.gov/health. If reprinted or used in any format, there must be no charge for viewing any part of the document. Distributed by the City of Houston Department of Health and Human Services Dear Fellow Houstonians: The Houston Department of Health and Human Services (HDHHS) is committed towards eliminating health disparities for vulnerable populations as defined by race/ethnicity, socio- economic status, geography, gender, age, disability status, and risk status related to sex and gender. Health disparities are defined as differences in health conditions which exist between specific population groups, resulting in one group having a disproportionate burden of disease, disability, or premature death. The purpose of the HDHHS is to protect and promote the health and well-being of all Houston residents through advocacy, education, and community-based health services. Houston is both the largest city in Texas and fourth largest city in the United States; a growing, diverse city with a vibrant economy in industries of energy, production, processing, science, medicine, and technology. The Texas Medical Center is one of the largest concentrations of hospitals and medical teaching facilities in the nation, and is renowned as a leader in research, education, and medical treatment. -

Download Document the 2019 Kinder Houston Area Survey Through 38
Building Better Cities Building Better Lives The 2019 Kinder Houston Area Survey Tracking Responses to the Economic and Demographic Transformations through 38 Years of Houston Surveys STEPHEN L. KLINEBERG, FOUNDING DIRECTOR, KINDER INSTITUTE FOR URBAN RESEARCH MAY 2019 We define our success through yours We can only be successful if our employees, customers and the communities we serve have the opportunity to achieve their own vision of success. Bank of America is helping to build a better tomorrow by using our capital, expertise and innovation to foster a diverse workforce to address societal issues like climate change, gender equality and economic mobility. Shared success means creating responsible, sustainable growth for our company and our world. Learn more at bankofamerica.com/about. Connect with us: @BofA_News ©2019 Bank of America Corporation | AR64WX5V | ESG-236-AD CONTENTS 1 Contents 2 Introduction; Survey Methodology 4 Highlights from the Thirty-Eighth Year 7 The Houston Economy across the 38 Years 11 The Education Crisis and the Growing Inequalities 15 Feeling More at Home with Houston’s Burgeoning Diversity 20 After Harvey 23 Continuity and Change in Political Orientations 27 Concluding Note Tracking Responses to the Economic and Demographic Transformations Through 38 Years of Houston Surveys xiquinhosilva/flickr xiquinhosilva/flickr Introduction or 38 years, Rice University’s Kinder Houston Area Survey has been tracking systematically the continuities and changes in the perceptions and experiences of successive representative Fsamples of Harris County adults. Through intensive interviews with a total of more than 46,000 Houston area residents, the surveys have been measuring the trends among Harris County residents in their life experiences, attitudes, and beliefs during almost four decades of remarkable economic, demographic, and technological change. -

YOON-THESIS.Pdf (426.3Kb)
ASIAN RESIDENTIAL SEGREGATION IN HOUSTON, TEXAS A Thesis by BO HEE YOON Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE August 2007 Major Subject: Sociology ASIAN RESIDENTIAL SEGREGATION IN HOUSTON, TEXAS A Thesis by BO HEE YOON Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE Approved by: Chair of Committee, Mark Fossett Committee Members, Dudley L. Poston, Jr. Rogelio Saenz Daniel Z. Sui Head of Department, Mark Fossett August 2007 Major Subject: Sociology iii ABSTRACT Asian Residential Segregation in Houston, Texas. (August 2007) Bo Hee Yoon, B.A., Sogang University Chair of Advisory Committee: Dr. Mark Fossett This thesis investigates the residential segregation of the Asian population in Houston considering segregation among Asian groups as well as segregation of Asians from broader non-Asian groups, namely whites, blacks, and Hispanics. Methods applied in this thesis draw on previous works on residential segregation and measure segregation using indices of exposure and isolation and indices of uneven distribution. The demographic and historical backgrounds of Asian populations are reviewed to identify potential reasons for Asian residential segregation. New major findings from my analysis are that Asians have socioeconomic status similar to whites and, thus, have higher socioeconomic status than blacks and Hispanics who have low socioeconomic status. Other major findings are that Asians have moderate segregation from whites, high segregation from Hispanics and even higher segregation from blacks. Detailed Asian groups are mostly moderately segregated from whites and are more highly segregated from Hispanics and blacks. -

The Role of Helicobacter Pylori Virulence and Host Genetic Factors in Gastroduodenal Disease
The role of Helicobacter pylori virulence and host genetic factors in gastroduodenal disease Heather-Marie Ann Schmidt A thesis submitted as fulfilment of the requirement for the degree of Doctor of Philosophy (PhD) School of Biotechnology and Biomolecular Sciences University of New South Wales 2010 Abstract Helicobacter pylori, a gastric bacterial pathogen, colonises >50% of the world’s population. Colonisation invariably leads to chronic gastritis, with a small but significant proportion progressing to peptic ulcer disease and gastric cancer (GC). The reason why some individuals progress to severe disease is unknown, but is likely the result of an as yet unidentified combination of bacterial, host and environmental factors. This thesis aimed to elucidate the contribution of host genetics and H. pylori virulence to severe disease, particularly GC, in patients from different ethnicities. Papers I, II and III investigated a comprehensive set of H. pylori virulence factors for their association with pro-inflammatory signalling in gastric epithelial cells in vitro and disease development. The major H. pylori virulence factors, including the cag PAI, vacA, babA and oipA were highly prevalent in all three ethnic groups resident in Malaysia and Singapore irrespective of the disease state of the host, suggesting all strains from this region are highly virulent. There was significant ethnic variation in the CagA EPIYA-motifs, HP0521 alleles and dupA, confirming that distinct H. pylori strains circulate within particular populations. Paper IV assessed strains isolated from patients with different levels of inflammation for their ability to cause dendritic cell maturation and activation, and induce pro- inflammatory signalling in gastric epithelial cells in vitro. -

From the Archives of South Texas 180
THE JOURNAL OF SOUTH TEXAS A journal devoted to the history and heritage of South Texas VOLUME 33 NUMBER 2 | FALL 2019 MANAGING EDITOR Alberto Rodriguez PhD ASSISTANT MANAGING EDITORS Veronica Duran MA William C. Yancey PhD EDITORS Larry Knight PhD, Roger Tuller PhD Je Glick PhD, and Manuel Flores EdD BOOK REVIEW EDITOR Jesse Esparza PhD WEBSITE EDITOR Mamadee M. Koromah PUBLISHER Texas A&M University-Kingsville Produced by e College of Arts and Sciences at Texas A&M University-Kingsville for e South Texas Historical Association Copyright © 2019 THE SOUTH TEXAS HISTORICAL ASSOCIATION Founded in 1954 “to encourage and to aid in the development of local historical societies and to discover, collect, preserve, and publish historical records and data relating to South Texas, and with special emphasis on the Tamaulipan background and the colony of Nuevo Santander.” OFFICERS President -Carroll Scogin-Brinceeld Vice President - Lynn M. Burlbaw Treasurer - Mike Carlisle Secretary - George Gellett Parliamentarian - Laurie Jasinski BOARD OF DIRECTORS Gary Hickinbotham - New Braunfels Arnulfo Mar - Brownsville Lisa Neely - Kingsville Dr. Manuel Flores – Kingsville e Journal of South Texas (ISSN: 1099-9310) is a biannual publication and is sent to all members of the South Texas Historical Association. Individual STHA membership is $25 annually. Joint membership per couple is $30 annually. Membership dues should be sent to Michael Carlisle, 3749 Piedra Creek, Corpus Christi, Texas 78410 Or for P.O. Box purposes: Mike Carlisle, MCC Writing, P.O. Box 260299, Corpus Christi, Texas 78426 Responsibility for statements of fact or opinion appearing in the Journal belongs to the individual authors and not to the South Texas Historical Association or Texas A&M University - Kingsville. -

Economic Development Page 45 of 153
RICE UNIVERSITY Shell Center for Sustainability SUSTAINABLE DEVELOPMENT OF . HOUSTON DISTRICTSDISTRICTS:: ECONOMIC The Health of the City DEVELOPMENT LESTER KING, PhD. Economic Development Page 45 of 153 Economic Development Page 46 of 153 Sustainable Development of Houston Districts: The Health of the City by Lester King, PhD, AICP, LEED Economic Development Pillar of Sustainability Economic Development Pillar of Sustainability ...................................................................................... 47 Theme - Economic Development ............................................................................................................ 49 Sub Theme - Employment ................................................................................................................... 49 Sub Theme - Macroeconomic Performance ....................................................................................... 53 Sub Theme - Earnings ......................................................................................................................... 57 Sub Theme – Business Location .......................................................................................................... 59 Theme - Consumption and Production ................................................................................................... 65 Sub Theme – Capital Improvements ................................................................................................... 65 Theme - Transportation .........................................................................................................................