A Genome-Wide Approach Accounting for Body
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chromosomal Aberrations in Head and Neck Squamous Cell Carcinomas in Norwegian and Sudanese Populations by Array Comparative Genomic Hybridization
825-843 12/9/08 15:31 Page 825 ONCOLOGY REPORTS 20: 825-843, 2008 825 Chromosomal aberrations in head and neck squamous cell carcinomas in Norwegian and Sudanese populations by array comparative genomic hybridization ERIC ROMAN1,2, LEONARDO A. MEZA-ZEPEDA3, STINE H. KRESSE3, OLA MYKLEBOST3,4, ENDRE N. VASSTRAND2 and SALAH O. IBRAHIM1,2 1Department of Biomedicine, Faculty of Medicine and Dentistry, University of Bergen, Jonas Lies vei 91; 2Department of Oral Sciences - Periodontology, Faculty of Medicine and Dentistry, University of Bergen, Årstadveien 17, 5009 Bergen; 3Department of Tumor Biology, Institute for Cancer Research, Rikshospitalet-Radiumhospitalet Medical Center, Montebello, 0310 Oslo; 4Department of Molecular Biosciences, University of Oslo, Blindernveien 31, 0371 Oslo, Norway Received January 30, 2008; Accepted April 29, 2008 DOI: 10.3892/or_00000080 Abstract. We used microarray-based comparative genomic logical parameters showed little correlation, suggesting an hybridization to explore genome-wide profiles of chromosomal occurrence of gains/losses regardless of ethnic differences and aberrations in 26 samples of head and neck cancers compared clinicopathological status between the patients from the two to their pair-wise normal controls. The samples were obtained countries. Our findings indicate the existence of common from Sudanese (n=11) and Norwegian (n=15) patients. The gene-specific amplifications/deletions in these tumors, findings were correlated with clinicopathological variables. regardless of the source of the samples or attributed We identified the amplification of 41 common chromosomal carcinogenic risk factors. regions (harboring 149 candidate genes) and the deletion of 22 (28 candidate genes). Predominant chromosomal alterations Introduction that were observed included high-level amplification at 1q21 (harboring the S100A gene family) and 11q22 (including Head and neck squamous cell carcinoma (HNSCC), including several MMP family members). -

Whole Exome Sequencing in Families at High Risk for Hodgkin Lymphoma: Identification of a Predisposing Mutation in the KDR Gene
Hodgkin Lymphoma SUPPLEMENTARY APPENDIX Whole exome sequencing in families at high risk for Hodgkin lymphoma: identification of a predisposing mutation in the KDR gene Melissa Rotunno, 1 Mary L. McMaster, 1 Joseph Boland, 2 Sara Bass, 2 Xijun Zhang, 2 Laurie Burdett, 2 Belynda Hicks, 2 Sarangan Ravichandran, 3 Brian T. Luke, 3 Meredith Yeager, 2 Laura Fontaine, 4 Paula L. Hyland, 1 Alisa M. Goldstein, 1 NCI DCEG Cancer Sequencing Working Group, NCI DCEG Cancer Genomics Research Laboratory, Stephen J. Chanock, 5 Neil E. Caporaso, 1 Margaret A. Tucker, 6 and Lynn R. Goldin 1 1Genetic Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 2Cancer Genomics Research Laboratory, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 3Ad - vanced Biomedical Computing Center, Leidos Biomedical Research Inc.; Frederick National Laboratory for Cancer Research, Frederick, MD; 4Westat, Inc., Rockville MD; 5Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; and 6Human Genetics Program, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD, USA ©2016 Ferrata Storti Foundation. This is an open-access paper. doi:10.3324/haematol.2015.135475 Received: August 19, 2015. Accepted: January 7, 2016. Pre-published: June 13, 2016. Correspondence: [email protected] Supplemental Author Information: NCI DCEG Cancer Sequencing Working Group: Mark H. Greene, Allan Hildesheim, Nan Hu, Maria Theresa Landi, Jennifer Loud, Phuong Mai, Lisa Mirabello, Lindsay Morton, Dilys Parry, Anand Pathak, Douglas R. Stewart, Philip R. Taylor, Geoffrey S. Tobias, Xiaohong R. Yang, Guoqin Yu NCI DCEG Cancer Genomics Research Laboratory: Salma Chowdhury, Michael Cullen, Casey Dagnall, Herbert Higson, Amy A. -
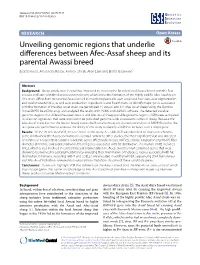
Unveiling Genomic Regions That Underlie Differences Between Afec-Assaf Sheep and Its Parental Awassi Breed
Seroussi et al. Genet Sel Evol (2017) 49:19 DOI 10.1186/s12711-017-0296-3 Genetics Selection Evolution RESEARCH Open Access Unveiling genomic regions that underlie differences between Afec‑Assaf sheep and its parental Awassi breed Eyal Seroussi, Alexander Rosov, Andrey Shirak, Alon Lam and Elisha Gootwine* Abstract Background: Sheep production in Israel has improved by crossing the fat-tailed local Awassi breed with the East Friesian and later, with the Booroola Merino breed, which led to the formation of the highly prolific Afec-Assaf strain. This strain differs from its parental Awassi breed in morphological traits such as tail and horn size, coat pigmentation and wool characteristics, as well as in production, reproductive and health traits. To identify major genes associated with the formation of the Afec-Assaf strain, we genotyped 41 Awassi and 141 Afec-Assaf sheep using the Illumina Ovine SNP50 BeadChip array, and analyzed the results with PLINK and EMMAX software. The detected variable genomic regions that differed between Awassi and Afec-Assaf sheep (variable genomic regions; VGR) were compared to selection signatures that were reported in 48 published genome-wide association studies in sheep. Because the Afec-Assaf strain, but not the Awassi breed, carries the Booroola mutation, association analysis of BMPR1B used as the test gene was performed to evaluate the ability of this study to identify a VGR that includes such a major gene. Results: Of the 20 detected VGR, 12 were novel to this study. A ~7-Mb VGR was identified on Ovies aries chromo- some OAR6 where the Booroola mutation is located. -

The Genes Pme-1 and Pme-2 Encode Two Poly(ADP-Ribose) Polymerases in Caenorhabditis Elegans Steve N
Biochem. J. (2002) 368, 263–271 (Printed in Great Britain) 263 The genes pme-1 and pme-2 encode two poly(ADP-ribose) polymerases in Caenorhabditis elegans Steve N. GAGNON*, Michael O. HENGARTNER† and Serge DESNOYERS*1 *Department of Pediatrics, Laval University Medical Research Centre and Faculty of Medicine, Laval University, Quebec, Canada, and †Institute of Molecular Biology, University of Zu$ rich, Winterthurerstrasse 190, 8057 Zu$ rich, Switzerland Poly(ADP-ribose) polymerases (PARPs) are an expanding, well- domain of PARPs in general and shares 24% identity with conserved family of enzymes found in many metazoan species, huPARP-2. Recombinant PME-1 and PME-2 display PARP including plants. The enzyme catalyses poly(ADP-ribosyl)ation, activity, which may partially account for the similar activity a post-translational modification that is important in DNA found in the worm. A partial duplication of the pme-1 gene with repair and programmed cell death. In the present study, we pseudogene-like features was found in the nematode genome. report the finding of an endogenous source of poly(ADP- Messenger RNA for pme-1 are 5h-tagged with splice leader 1, ribosyl)ation in total extracts of the nematode Caenorhabditis whereas those for pme-2 are tagged with splice leader 2, suggesting elegans. Two cDNAs encoding highly similar proteins to human an operon-like expression for pme-2. The expression pattern of PARP-1 (huPARP-1) and huPARP-2 are described, and we pme-1 and pme-2 is also developmentally regulated. Together, propose to name the corresponding enzymes poly(ADP-ribose) these results show that PARP-1 and -2 are conserved in evolution metabolism enzyme 1 (PME-1) and PME-2 respectively. -

A High Throughput, Functional Screen of Human Body Mass Index GWAS Loci Using Tissue-Specific Rnai Drosophila Melanogaster Crosses Thomas J
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2018 A high throughput, functional screen of human Body Mass Index GWAS loci using tissue-specific RNAi Drosophila melanogaster crosses Thomas J. Baranski Washington University School of Medicine in St. Louis Aldi T. Kraja Washington University School of Medicine in St. Louis Jill L. Fink Washington University School of Medicine in St. Louis Mary Feitosa Washington University School of Medicine in St. Louis Petra A. Lenzini Washington University School of Medicine in St. Louis See next page for additional authors Follow this and additional works at: https://digitalcommons.wustl.edu/open_access_pubs Recommended Citation Baranski, Thomas J.; Kraja, Aldi T.; Fink, Jill L.; Feitosa, Mary; Lenzini, Petra A.; Borecki, Ingrid B.; Liu, Ching-Ti; Cupples, L. Adrienne; North, Kari E.; and Province, Michael A., ,"A high throughput, functional screen of human Body Mass Index GWAS loci using tissue-specific RNAi Drosophila melanogaster crosses." PLoS Genetics.14,4. e1007222. (2018). https://digitalcommons.wustl.edu/open_access_pubs/6820 This Open Access Publication is brought to you for free and open access by Digital Commons@Becker. It has been accepted for inclusion in Open Access Publications by an authorized administrator of Digital Commons@Becker. For more information, please contact [email protected]. Authors Thomas J. Baranski, Aldi T. Kraja, Jill L. Fink, Mary Feitosa, Petra A. Lenzini, Ingrid B. Borecki, Ching-Ti Liu, L. Adrienne Cupples, Kari E. North, and Michael A. Province This open access publication is available at Digital Commons@Becker: https://digitalcommons.wustl.edu/open_access_pubs/6820 RESEARCH ARTICLE A high throughput, functional screen of human Body Mass Index GWAS loci using tissue-specific RNAi Drosophila melanogaster crosses Thomas J. -

Massively Parallel Discovery of Human-Specific Substitutions That Alter Neurodevelopmental Enhancer Activity
bioRxiv preprint doi: https://doi.org/10.1101/865519; this version posted December 5, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. Massively parallel discovery of human-specific substitutions that alter neurodevelopmental enhancer activity Authors: Severin Uebbing1*, Jake Gockley1*§, Steven K. Reilly1†, Acadia A. Kocher1, Evan Geller1, Neeru Gandotra1, Curt Scharfe1, Justin Cotney1‡, James P. Noonan1,2,3,4+ Affiliations: 1 Department of Genetics, Yale School of Medicine, New Haven, CT 06510, USA. 2 Department of Ecology and Evolutionary Biology, Yale University, New Haven, CT 06520, USA. 3 Department of Neuroscience, Yale School of Medicine, New Haven, CT 06510, USA. 4 Kavli Institute for Neuroscience, Yale School of Medicine, New Haven, CT 06510, USA. *These authors contributed equally to the work. §Present address: Sage Bionetworks, Seattle, WA 98121, USA. †Present address: Broad Institute, Cambridge, MA 02142, USA. ‡Present address: Department of Genetics and Genome Science, University of Connecticut Health, Farmington, CT 06030, USA. +Corresponding author: [email protected]. bioRxiv preprint doi: https://doi.org/10.1101/865519; this version posted December 5, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. Abstract Genetic changes that altered the function of gene regulatory elements have been implicated in the evolution of the human brain. -

Structure and Dynamics of the Insulin Receptor: Implications for Receptor Activation and Drug Discovery
REVIEWS Drug Discovery Today Volume 22, Number 7 July 2017 Reviews Structure and dynamics of the insulin POST SCREEN receptor: implications for receptor activation and drug discovery 1 1 2 2 Libin Ye , Suvrajit Maji , Narinder Sanghera , Piraveen Gopalasingam , 3 3 4 Evgeniy Gorbunov , Sergey Tarasov , Oleg Epstein and Judith Klein- Seetharaman1,2 1 Department of Structural Biology, University of Pittsburgh, Pittsburgh, PA 15260, USA 2 Division of Metabolic and Vascular Health & Systems, Medical School, University of Warwick, Coventry CV4 7AL, UK 3 OOO ‘NPF ‘MATERIA MEDICA HOLDING’, 47-1, Trifonovskaya St, Moscow 129272, Russian Federation 4 The Institute of General Pathology and Pathophysiology, 8, Baltiyskaya St, 125315 Moscow, Russian Federation Recently, major progress has been made in uncovering the mechanisms of how insulin engages its receptor and modulates downstream signal transduction. Here, we present in detail the current structural knowledge surrounding the individual components of the complex, binding sites, and dynamics during the activation process. A novel kinase triggering mechanism, the ‘bow-arrow model’, is proposed based on current knowledge and computational simulations of this system, in which insulin, after its initial interaction with binding site 1, engages with site 2 between the fibronectin type III (FnIII)- 1 and -2 domains, which changes the conformation of FnIII-3 and eventually translates into structural changes across the membrane. This model provides a new perspective on the process of insulin binding to its receptor and, thus, could lead to future novel drug discovery efforts. Introduction upon insulin binding [8]. The first crystal structure of the basal The insulin receptor (IR) has a pivotal role in the regulation of (inactive) TK was reported in 1994 [9]. -

Vast Human-Specific Delay in Cortical Ontogenesis Associated With
Supplementary information Extension of cortical synaptic development distinguishes humans from chimpanzees and macaques Supplementary Methods Sample collection We used prefrontal cortex (PFC) and cerebellar cortex (CBC) samples from postmortem brains of 33 human (aged 0-98 years), 14 chimpanzee (aged 0-44 years) and 44 rhesus macaque individuals (aged 0-28 years) (Table S1). Human samples were obtained from the NICHD Brain and Tissue Bank for Developmental Disorders at the University of Maryland, USA, the Netherlands Brain Bank, Amsterdam, Netherlands and the Chinese Brain Bank Center, Wuhan, China. Informed consent for use of human tissues for research was obtained in writing from all donors or their next of kin. All subjects were defined as normal by forensic pathologists at the corresponding brain bank. All subjects suffered sudden death with no prolonged agonal state. Chimpanzee samples were obtained from the Yerkes Primate Center, GA, USA, the Anthropological Institute & Museum of the University of Zürich-Irchel, Switzerland and the Biomedical Primate Research Centre, Netherlands (eight Western chimpanzees, one Central/Eastern and five of unknown origin). Rhesus macaque samples were obtained from the Suzhou Experimental Animal Center, China. All non-human primates used in this study suffered sudden deaths for reasons other than their participation in this study and without any relation to the tissue used. CBC dissections were made from the cerebellar cortex. PFC dissections were made from the frontal part of the superior frontal gyrus. All samples contained an approximately 2:1 grey matter to white matter volume ratio. RNA microarray hybridization RNA isolation, hybridization to microarrays, and data preprocessing were performed as described previously (Khaitovich et al. -

Deepsvp: Integration of Genotype and Phenotype for Structural Variant Prioritization Using Deep Learning
bioRxiv preprint doi: https://doi.org/10.1101/2021.01.28.428557; this version posted April 9, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY 4.0 International license. i i “output” — 2021/4/9 — 6:14 — page 1 — #1 i i Bioinformatics doi.10.1093/bioinformatics/xxxxxx Applications Note Genome analysis DeepSVP: Integration of genotype and phenotype for structural variant prioritization using deep learning Azza Althagafi 1,2, Lamia Alsubaie 3, Nagarajan Kathiresan 4, Katsuhiko Mineta 1, Taghrid Aloraini 3, Fuad Almutairi 5,6, Majid Alfadhel 5,6,7, Takashi Gojobori 8, Ahmad Alfares 3,7,9, and Robert Hoehndorf1,∗ 1 Computational Bioscience Research Center (CBRC), Computer, Electrical and Mathematical Sciences & Engineering Division (CEMSE), King Abdullah University of Science and Technology (KAUST), Thuwal 23955-6900, Saudi Arabia (SA); 2 Computer Science Department, College of Computers and Information Technology, Taif University, Taif, SA; 3 Department of Pathology and Laboratory Medicine, King Abdulaziz Medical City (KAMC), Riyadh, SA; 4 Supercomputing Core Lab, KAUST, Thuwal, SA; 5 Division of Genetics, Department of Pediatrics, KAMC, Riyadh, SA; 6 King Saud bin Abdulaziz University for Health Sciences, KAMC, Riyadh, SA; 7 King Abdullah International Medical Research Center, Riyadh, SA; 8 Biological and Environmental Science and Engineering Division, CBRC, KAUST, Thuwal, SA; 9 Department of Pediatrics, College of Medicine, Qassim University, Qassim, SA. ∗To whom correspondence should be addressed. Associate Editor: XXXXXXX Received on XXXXX; revised on XXXXX; accepted on XXXXX Abstract Motivation: Structural genomic variants account for much of human variability and are involved in several diseases. -

Downloaded from the European Nucleotide Archive (ENA; 126
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 5 September 2018 doi:10.20944/preprints201809.0082.v1 1 Article 2 Transcriptomics as precision medicine to classify in 3 vivo models of dietary-induced atherosclerosis at 4 cellular and molecular levels 5 Alexei Evsikov 1,2, Caralina Marín de Evsikova 1,2* 6 1 Epigenetics & Functional Genomics Laboratory, Department of Molecular Medicine, Morsani College of 7 Medicine, University of South Florida, Tampa, Florida, 33612, USA; 8 2 Department of Research and Development, Bay Pines Veteran Administration Healthcare System, Bay 9 Pines, FL 33744, USA 10 11 * Correspondence: [email protected]; Tel.: +1-813-974-2248 12 13 Abstract: The central promise of personalized medicine is individualized treatments that target 14 molecular mechanisms underlying the physiological changes and symptoms arising from disease. 15 We demonstrate a bioinformatics analysis pipeline as a proof-of-principle to test the feasibility and 16 practicality of comparative transcriptomics to classify two of the most popular in vivo diet-induced 17 models of coronary atherosclerosis, apolipoprotein E null mice and New Zealand White rabbits. 18 Transcriptomics analyses indicate the two models extensively share dysregulated genes albeit with 19 some unique pathways. For instance, while both models have alterations in the mitochondrion, the 20 biochemical pathway analysis revealed, Complex IV in the electron transfer chain is higher in mice, 21 whereas the rest of the electron transfer chain components are higher in the rabbits. Several fatty 22 acids anabolic pathways are expressed higher in mice, whereas fatty acids and lipids degradation 23 pathways are higher in rabbits. -
University of Cincinnati
UNIVERSITY OF CINCINNATI Date:___________________ I, _________________________________________________________, hereby submit this work as part of the requirements for the degree of: in: It is entitled: This work and its defense approved by: Chair: _______________________________ _______________________________ _______________________________ _______________________________ _______________________________ CHARACTERIZATION OF TANKYRASE STRUCTURE & FUNCTION; EVIDENCE FOR A ROLE AS A MASTER SCAFFOLDING PROTEIN A dissertation submitted to the Division of Research and Advanced Studies of the University of Cincinnati in partial fulfillment of the requirements for the degree of DOCTORATE OF PHILOSOPHY (Ph.D.) in the Department of Molecular Genetics, Biochemistry and Microbiology College of Medicine 2004 by Manu De Rycker B.S., University of Antwerp, 1995 M.S., University of Gent, 1998 Committee Chair: Carolyn Price, Ph.D. ABSTRACT Tankyrases are novel poly(ADP-ribose) polymerases that have SAM and ankyrin protein- interaction domains. They are found at telomeres, centrosomes, nuclear pores and the Golgi- apparatus, and participate in telomere length regulation and resolution of sister chromatid association. Their other function(s) are unknown and it has been difficult to envision a common role at such diverse cellular locations. We isolated the chicken tankyrase homologs and examined their interaction partners, subcellular location and domain functions to learn more about their mode of action. Cross-species sequence comparison indicated that tankyrase domain structure is highly conserved and supports division of the ankyrin domain into five subdomains, each separated by a highly conserved LLEAAR/K motif. GST-pull down experiments demonstrated that the ankyrin domains of both proteins interact with chicken TRF1. Analysis of total cellular and nuclear proteins showed that cells contain approximately twice as much tankyrase 1 as tankyrase 2. -

Download Coordinates the Pymol Scripts for Visualizing All Available Interfaces
bioRxiv preprint doi: https://doi.org/10.1101/579862; this version posted March 18, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. RESOURCE ProtCID: A tool for hypothesis generation of the structures of protein interactions Qifang Xu, Roland L. Dunbrack, Jr.* Fox Chase Cancer Center 333 Cottman Avenue Philadelphia PA 19111 * [email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/579862; this version posted March 18, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. Abstract Interaction of proteins with other molecules is central to their ability to carry out biological functions. These interactions include those in homo- and heterooligomeric protein complexes as well as those with nucleic acids, lipids, ions, and small molecules. Structural information on the interactions of proteins with other molecules is very plentiful, and for some proteins and protein domain families, there may be 100s or even 1000s of available structures. While it is possible for any biological scientist to search the Protein Data Bank and investigate individual structures, it is virtually impossible for a scientist who is not trained in structural bioinformatics to access this information across all of the structures that are available of any one extensively studied protein or protein family.