The Respiratory System Chapter 15 the Respiratory System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The Structure and Function of Breathing
CHAPTERCONTENTS The structure-function continuum 1 Multiple Influences: biomechanical, biochemical and psychological 1 The structure and Homeostasis and heterostasis 2 OBJECTIVE AND METHODS 4 function of breathing NORMAL BREATHING 5 Respiratory benefits 5 Leon Chaitow The upper airway 5 Dinah Bradley Thenose 5 The oropharynx 13 The larynx 13 Pathological states affecting the airways 13 Normal posture and other structural THE STRUCTURE-FUNCTION considerations 14 Further structural considerations 15 CONTINUUM Kapandji's model 16 Nowhere in the body is the axiom of structure Structural features of breathing 16 governing function more apparent than in its Lung volumes and capacities 19 relation to respiration. This is also a region in Fascla and resplrstory function 20 which prolonged modifications of function - Thoracic spine and ribs 21 Discs 22 such as the inappropriate breathing pattern dis- Structural features of the ribs 22 played during hyperventilation - inevitably intercostal musculature 23 induce structural changes, for example involving Structural features of the sternum 23 Posterior thorax 23 accessory breathing muscles as well as the tho- Palpation landmarks 23 racic articulations. Ultimately, the self-perpetuat- NEURAL REGULATION OF BREATHING 24 ing cycle of functional change creating structural Chemical control of breathing 25 modification leading to reinforced dysfunctional Voluntary control of breathing 25 tendencies can become complete, from The autonomic nervous system 26 whichever direction dysfunction arrives, for Sympathetic division 27 Parasympathetic division 27 example: structural adaptations can prevent NANC system 28 normal breathing function, and abnormal breath- THE MUSCLES OF RESPIRATION 30 ing function ensures continued structural adap- Additional soft tissue influences and tational stresses leading to decompensation. -

Infections of the Respiratory Tract
F70954-07.qxd 12/10/02 7:36 AM Page 71 Infections of the respiratory 7 tract the nasal hairs and by inertial impaction with mucus- 7.1 Pathogenesis 71 covered surfaces in the posterior nasopharynx (Fig. 11). 7.2 Diagnosis 72 The epiglottis, its closure reflex and the cough reflex all reduce the risk of microorganisms reaching the lower 7.3 Management 72 respiratory tract. Particles small enough to reach the tra- 7.4 Diseases and syndromes 73 chea and bronchi stick to the respiratory mucus lining their walls and are propelled towards the oropharynx 7.5 Organisms 79 by the action of cilia (the ‘mucociliary escalator’). Self-assessment: questions 80 Antimicrobial factors present in respiratory secretions further disable inhaled microorganisms. They include Self-assessment: answers 83 lysozyme, lactoferrin and secretory IgA. Particles in the size range 5–10 µm may penetrate further into the lungs and even reach the alveolar air Overview spaces. Here, alveolar macrophages are available to phagocytose potential pathogens, and if these are overwhelmed neutrophils can be recruited via the This chapter deals with infections of structures that constitute inflammatory response. The defences of the respira- the upper and lower respiratory tract. The general population tory tract are a reflection of its vulnerability to micro- commonly experiences upper respiratory tract infections, bial attack. Acquisition of microbial pathogens is which are often seen in general practice. Lower respiratory tract infections are less common but are more likely to cause serious illness and death. Diagnosis and specific chemotherapy of respiratory tract infections present a particular challenge to both the clinician and the laboratory staff. -

Peak Flow Measure: an Index of Respiratory Function?
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Peak Flow Measure: An Index of Respiratory Function? D. Devadiga, Aiswarya Liz Varghese, J. Bhat, P. Baliga, J. Pahwa Department of Audiology and Speech Language Pathology, Kasturba Medical College (A Unit of Manipal University), Mangalore -575001 Corresponding Author: Aiswarya Liz Varghese Received: 06/12/2014 Revised: 26/12/2014 Accepted: 05/01/2015 ABSTRACT Aerodynamic analysis is interpreted as a reflection of the valving activity of the larynx. It involves measuring changes in air volume, flow and pressure which indicate respiratory function. These measures help in determining the important aspects of lung function. Peak expiratory flow rate is a widely used respiratory measure and is an effective measure of effort dependent airflow. Aim: The aim of the current study was to study the peak flow as an aerodynamic measure in healthy normal individuals Method: The study group was divided into two groups with n= 60(30 males and 30 females) in the age range of 18-22 years. The peak flow was measured using Aerophone II (Voice Function Analyser). The anthropometric measurements such as height, weight and Body Mass Index was calculated for all the participants. Results: The peak airflow was higher in females as compared to that of males. It was also observed that the peak air flow rate was correlating well with height and weight in males. Conclusions: Speech language pathologist should consider peak expiratory airflow, a short sharp exhalation rate as a part of routine aerodynamic evaluation which is easier as compared to the otherwise commonly used measure, the vital capacity. -
Spirometry Basics
SPIROMETRY BASICS ROSEMARY STINSON MSN, CRNP THE CHILDREN’S HOSPITAL OF PHILADELPHIA DIVISION OF ALLERGY AND IMMUNOLOGY PORTABLE COMPUTERIZED SPIROMETRY WITH BUILT IN INCENTIVES WHAT IS SPIROMETRY? Use to obtain objective measures of lung function Physiological test that measures how an individual inhales or exhales volume of air Primary signal measured–volume or flow Essentially measures airflow into and out of the lungs Invaluable screening tool for respiratory health compared to BP screening CV health Gold standard for diagnosing and measuring airway obstruction. ATS, 2005 SPIROMETRY AND ASTHMA At initial assessment After treatment initiated and symptoms and PEF have stabilized During periods of progressive or prolonged asthma control At least every 1-2 years: more frequently depending on response to therapy WHY NECESSARY? o To evaluate symptoms, signs or abnormal laboratory tests o To measure the effect of disease on pulmonary function o To screen individuals at risk of having pulmonary disease o To assess pre-operative risk o To assess prognosis o To assess health status before beginning strenuous physical activity programs ATS, 2005 SPIROMETRY VERSUS PEAK FLOW Recommended over peak flow meter measurements in clinician’s office. Variability in predicted PEF reference values. Many different brands PEF meters. Peak Flow is NOT a diagnostic tool. Helpful for monitoring control. EPR 3, 2007 WHY MEASURE? o Some patients are “poor perceivers.” o Perception of obstruction variable and spirometry reveals obstruction more severe. o Family members “underestimate” severity of symptoms. o Objective assessment of degree of airflow obstruction. o Pulmonary function measures don’t always correlate with symptoms. o Comprehensive assessment of asthma. -

The Digestive System
69 chapter four THE DIGESTIVE SYSTEM THE DIGESTIVE SYSTEM The digestive system is structurally divided into two main parts: a long, winding tube that carries food through its length, and a series of supportive organs outside of the tube. The long tube is called the gastrointestinal (GI) tract. The GI tract extends from the mouth to the anus, and consists of the mouth, or oral cavity, the pharynx, the esophagus, the stomach, the small intestine, and the large intes- tine. It is here that the functions of mechanical digestion, chemical digestion, absorption of nutrients and water, and release of solid waste material take place. The supportive organs that lie outside the GI tract are known as accessory organs, and include the teeth, salivary glands, liver, gallbladder, and pancreas. Because most organs of the digestive system lie within body cavities, you will perform a dissection procedure that exposes the cavities before you begin identifying individual organs. You will also observe the cavities and their associated membranes before proceeding with your study of the digestive system. EXPOSING THE BODY CAVITIES should feel like the wall of a stretched balloon. With your skinned cat on its dorsal side, examine the cutting lines shown in Figure 4.1 and plan 2. Extend the cut laterally in both direc- out your dissection. Note that the numbers tions, roughly 4 inches, still working with indicate the sequence of the cutting procedure. your scissors. Cut in a curved pattern as Palpate the long, bony sternum and the softer, shown in Figure 4.1, which follows the cartilaginous xiphoid process to find the ventral contour of the diaphragm. -
The Respiratory System
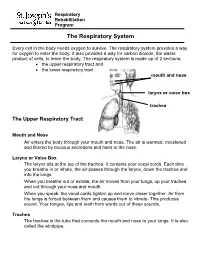
Respiratory Rehabilitation Program The Respiratory System Every cell in the body needs oxygen to survive. The respiratory system provides a way for oxygen to enter the body. It also provides a way for carbon dioxide, the waste product of cells, to leave the body. The respiratory system is made up of 2 sections: the upper respiratory tract and the lower respiratory tract mouth and nose larynx or voice box trachea The Upper Respiratory Tract Mouth and Nose Air enters the body through your mouth and nose. The air is warmed, moistened and filtered by mucous secretions and hairs in the nose. Larynx or Voice Box The larynx sits at the top of the trachea. It contains your vocal cords. Each time you breathe in or inhale, the air passes through the larynx, down the trachea and into the lungs. When you breathe out or exhale, the air moves from your lungs, up your trachea and out through your nose and mouth. When you speak, the vocal cords tighten up and move closer together. Air from the lungs is forced between them and causes them to vibrate. This produces sound. Your tongue, lips and teeth form words out of these sounds. Trachea The trachea is the tube that connects the mouth and nose to your lungs. It is also called the windpipe. The Lower Respiratory Tract Inside Lungs Outside Lungs bronchial tubes alveoli diaphragm (muscle) Bronchial Tubes The trachea splits into 2 bronchial tubes in your lungs. These are called the left bronchus and right bronchus. The bronchus tubes keep branching off into smaller and smaller tubes called bronchi. -

Lab #2: Organs of the Thoracic and Abdominal Cavities. Important: All Dissections of the Thoracic and Abdominal Cavities Will Be Done As a Class
Lab #2: Organs of the thoracic and abdominal cavities. Important: All dissections of the thoracic and abdominal cavities will be done as a class. Do Not get ahead of the class for you may cut into something that we will want to examine later. Goals: Be able to …. Locate and explain the functions of the structures listed below: Neck Region: Abdominal Cavity: thymus gland umbilical chord thyroid gland peritoneum larynx mesenteries trachea liver esophagus stomach thoracic Cavity: spleen right and left pleural cavities small intestine (locate duodenum) right and left lungs pancreas pericardial cavity large intestines heart cecum Thoracic/Abdominal Division: colon diaphragm 13.3 Thoracic and Abdominal Incisions Pp. 164 – 165 Make incisions with class and instructor!!! 13.4 Neck Region, Thoracic Cavity and Abdominal Cavity Pp. 166-170 – Read all introductions, follow the procedures to locate the organs specified and answer all the questions. Pp. 172 – Answer questions #6-8, 11-17, 19 Arrange the organs in order by the way food travels through them: Stomach, esophagus, large intestines, mouth, small intestines, anus, rectum The inhalation of a breath of travels through several organs. Put the following organs in their proper order: Bronchi, nasal passages, bronchioles, larynx, pharynx, alveoli, trachea II. Respiration and Digestion Stations Goals: After this lab you should be able to………….. 1. Describe the appearance of villi and explain how the structure of villi supports their function. 2. Describe the internal structure of the lungs and explain the process of gas exchange. 3. Explain the difference in appearance and function between healthy alveoli and diseased alveoli. -

Human Anatomy and Physiology
LECTURE NOTES For Nursing Students Human Anatomy and Physiology Nega Assefa Alemaya University Yosief Tsige Jimma University In collaboration with the Ethiopia Public Health Training Initiative, The Carter Center, the Ethiopia Ministry of Health, and the Ethiopia Ministry of Education 2003 Funded under USAID Cooperative Agreement No. 663-A-00-00-0358-00. Produced in collaboration with the Ethiopia Public Health Training Initiative, The Carter Center, the Ethiopia Ministry of Health, and the Ethiopia Ministry of Education. Important Guidelines for Printing and Photocopying Limited permission is granted free of charge to print or photocopy all pages of this publication for educational, not-for-profit use by health care workers, students or faculty. All copies must retain all author credits and copyright notices included in the original document. Under no circumstances is it permissible to sell or distribute on a commercial basis, or to claim authorship of, copies of material reproduced from this publication. ©2003 by Nega Assefa and Yosief Tsige All rights reserved. Except as expressly provided above, no part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without written permission of the author or authors. This material is intended for educational use only by practicing health care workers or students and faculty in a health care field. Human Anatomy and Physiology Preface There is a shortage in Ethiopia of teaching / learning material in the area of anatomy and physicalogy for nurses. The Carter Center EPHTI appreciating the problem and promoted the development of this lecture note that could help both the teachers and students. -

RESPIRATORY TRACT INFECTIONS Peter Zajac, DO, FACOFP, Author Amy J
OFP PATIENT EDUCATION HANDOUT RESPIRATORY TRACT INFECTIONS Peter Zajac, DO, FACOFP, Author Amy J. Keenum, DO, PharmD, Editor • Ronald Januchowski, DO, FACOFP, Health Literacy Editor HOME MANAGEMENT INCLUDES: • Drinking plenty of clear fuids and rest. Vitamin-C may help boost your immune system. Over-the-counter pain relievers such as acetaminophen and ibuprofen can be helpful for fevers and to ease any aches. Saline (salt) nose drops, lozenges, and vapor rubs can also help symptoms when used as directed by your physician. • A cool mist humidifer can make breathing easier by thinning mucus. • If you smoke, you should try to stop smoking for good! Avoid second-hand smoking also. • In most cases, antibiotics are not recommended because they are only effective if bacteria caused the infection. • Other treatments, that your Osteopathic Family Physician may prescribe, include Osteopathic Manipulative Therapy (OMT). OMT can help clear mucus, Respiratory tract infections are any relieve congestion, improve breathing and enhance comfort, relaxation, and infection that affect the nose, sinuses, immune function. and throat (i.e. the upper respiratory tract) or airways and lungs (i.e. the • Generally, the symptoms of a respiratory tract infection usually pass within lower respiratory tract). Viruses are one to two weeks. the main cause of the infections, but • To prevent spreading infections, sneeze into the arm of your shirt or in a tissue. bacteria can cause some. You can Also, practice good hygiene such as regularly washing your hands with soap and spread the infection to others through warm water. Wipe down common surfaces, such as door knobs and faucet handles, the air when you sneeze or cough. -

Respiratory Tract Infections in the Tropics
9.1 CHAPTER 9 Respiratory Tract Infections in the Tropics Tim J.J. Inglis 9.1 INTRODUCTION Acute respiratory infections are the single most common infective cause of death worldwide. This is also the case in the tropics, where they are a major cause of death in children under five. Bacterial pneumonia is particularly common in children in the tropics, and is more often lethal. Pulmonary tuberculosis is the single most common fatal infection and is more prevalent in many parts of the tropics due to a combination of endemic HIV infection and widespread poverty. A lack of diagnostic tests, limited access to effective treatment and some traditional healing practices exacerbate the impact of respiratory infection in tropical communities. The rapid urbanisation of populations in the tropics has increased the risk of transmitting respiratory pathogens. A combination of poverty and overcrowding in the peri- urban zones of rapidly expanding tropical cities promotes the epidemic spread of acute respiratory infection. PART A. INFECTIONS OF THE LOWER RESPIRATORY TRACT 9.2 PNEUMONIA 9.2.1 Frequency Over four million people die from acute respiratory infection per annum, mostly in developing countries. There is considerable overlap between these respiratory deaths and deaths due to tuberculosis, the single commonest fatal infection. The frequency of acute respiratory infection differs with location due to host, pathogen and environmental factors. Detailed figures are difficult to find and often need to be interpreted carefully, even for tuberculosis where data collection is more consistent. But in urban settings the enormity of respiratory infection is clearly evident. Up to half the patients attending hospital outpatient departments in developing countries have an acute respiratory infection. -

NIOSH), Centers for Disease Control and Prevention (CDC)
Technical Report Filtering Facepiece Respirators with an Exhalation Valve: Measurements of Filtration Efficiency to Evaluate Their Potential for Source Control Centers for Disease Control and Prevention National Institute for Occupational Safety and Health Technical Report Filtering Facepiece Respirators with an Exhalation Valve: Measurements of Filtration Efficiency to Evaluate Their Potential for Source Control DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Institute for Occupational Safety and Health National Personal Protective Technology Laboratory This document is in the public domain and may be freely copied or reprinted. Disclaimer Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention (CDC). In addition, citations to websites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these websites. All web addresses referenced in this document were accessible as of the publication date. Get More Information Find NIOSH products and get answers to workplace safety and health questions: 1-800-CDC-INFO (1-800-232-4636) | TTY: 1-888-232-6348 CDC/NIOSH INFO: cdc.gov/info | cdc.gov/niosh Monthly NIOSH eNews: cdc.gov/niosh/eNews Suggested Citation NIOSH [2020]. Filtering facepiece respirators with an exhalation valve: measurements of filtration efficiency to evaluate their potential for source control. By Portnoff L, Schall J, Brannen J, Suhon N, Strickland K, Meyers J. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. -

Physical and Geometric Constraints Shape the Labyrinth-Like Nasal Cavity
Physical and geometric constraints shape the labyrinth-like nasal cavity David Zwickera,b,1, Rodolfo Ostilla-Monico´ a,b, Daniel E. Liebermanc, and Michael P. Brennera,b aJohn A. Paulson School of Engineering and Applied Sciences, Harvard University, Cambridge, MA 02138; bKavli Institute for Bionano Science and Technology, Harvard University, Cambridge, MA 02138; and cDepartment of Human Evolutionary Biology, Harvard University, Cambridge, MA 02138 Edited by Leslie Greengard, New York University, New York, NY, and approved January 26, 2018 (received for review August 29, 2017) The nasal cavity is a vital component of the respiratory system take into account geometric constraints imposed by the shape that heats and humidifies inhaled air in all vertebrates. Despite of the head that determine the length of the nasal cavity, its this common function, the shapes of nasal cavities vary widely cross-sectional area, and, generally, the shape of the space that it across animals. To understand this variability, we here connect occupies. To tackle this complex problem, we first show that, nasal geometry to its function by theoretically studying the air- without geometric constraints, optimal shapes have slender flow and the associated scalar exchange that describes heating cross-sections. We then demonstrate that these shapes can be and humidification. We find that optimal geometries, which have compacted into the typical labyrinth-like shapes without much minimal resistance for a given exchange efficiency, have a con- loss in performance. stant gap width between their side walls, while their overall shape can adhere to the geometric constraints imposed by the Results head. Our theory explains the geometric variations of natural The Flow in the Nasal Cavity Is Laminar.