Respiratory Tract Infections in the Tropics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Infections of the Respiratory Tract
F70954-07.qxd 12/10/02 7:36 AM Page 71 Infections of the respiratory 7 tract the nasal hairs and by inertial impaction with mucus- 7.1 Pathogenesis 71 covered surfaces in the posterior nasopharynx (Fig. 11). 7.2 Diagnosis 72 The epiglottis, its closure reflex and the cough reflex all reduce the risk of microorganisms reaching the lower 7.3 Management 72 respiratory tract. Particles small enough to reach the tra- 7.4 Diseases and syndromes 73 chea and bronchi stick to the respiratory mucus lining their walls and are propelled towards the oropharynx 7.5 Organisms 79 by the action of cilia (the ‘mucociliary escalator’). Self-assessment: questions 80 Antimicrobial factors present in respiratory secretions further disable inhaled microorganisms. They include Self-assessment: answers 83 lysozyme, lactoferrin and secretory IgA. Particles in the size range 5–10 µm may penetrate further into the lungs and even reach the alveolar air Overview spaces. Here, alveolar macrophages are available to phagocytose potential pathogens, and if these are overwhelmed neutrophils can be recruited via the This chapter deals with infections of structures that constitute inflammatory response. The defences of the respira- the upper and lower respiratory tract. The general population tory tract are a reflection of its vulnerability to micro- commonly experiences upper respiratory tract infections, bial attack. Acquisition of microbial pathogens is which are often seen in general practice. Lower respiratory tract infections are less common but are more likely to cause serious illness and death. Diagnosis and specific chemotherapy of respiratory tract infections present a particular challenge to both the clinician and the laboratory staff. -

Unusual Case of Non-Resolving Necrotizing Pneumonia: a Last Resort Measure for Cure
eCommons@AKU Department of Surgery Department of Surgery June 2016 Unusual case of non-resolving necrotizing pneumonia: a last resort measure for cure. Naseem Salahuddin Aga Khan University, [email protected] Naila Baig Ansari Aga Khan University Saulat H. Fatimi Aga Khan University, [email protected] Follow this and additional works at: http://ecommons.aku.edu/pakistan_fhs_mc_surg_surg Part of the Surgery Commons Recommended Citation Salahuddin, N., Ansari, N., Fatimi, S. (2016). Unusual case of non-resolving necrotizing pneumonia: a last resort measure for cure.. JPMA: Journal of the Pakistan Medical Association, 66(6), 754-756. Available at: http://ecommons.aku.edu/pakistan_fhs_mc_surg_surg/566 754 CASE REPORT Unusual case of non-resolving necrotizing pneumonia: A last resort measure for cure Naseem Salahuddin, 1 Naila Baig-Ansari, 2 Saulat Hasnain Fatimi 3 Abstract pathogen of acute CAP, 2,3 and accounts for most cases of To our knowledge, this is an unusual case of a community- slowly resolving pneumonia.The majority of previously acquired pneumonia (CAP) with sepsis secondary to healthy hospitalized patients with severe CAP responded Streptococcus pneumoniae that required lung resection satisfactorily to prompt initiation of appropriate antibiotic for a non-resolving consolidation. A 74 year old previously therapy; however, it is estimated that 10% of hospitalized healthy woman, presented with acute fever, chills and CAP patients have slowly resolving or nonresolving pleuritic chest pain in Emergency Department (ED). A disease. 4 diagnosis of CAP was established with a Pneumonia Severity Index CURB-65 score of 5/5. In the ER, she was Case Report promptly and appropriately managed with antibiotics History: A 74 year old woman who was previously and aggressive supportive therapy. -
Toman's Tuberculosis Case Detection, Treatment, and Monitoring
TOMAN’S TUBERCULOSIS TOMAN’S TUBERCULOSIS CASE DETECTION, TREATMENT, AND MONITORING The second edition of this practical, authoritative reference book provides a rational basis for the diagnosis and management of tuberculosis. Written by a number of experts in the field, it remains faithful to Kurt Toman’s original question-and-answer format, with subject matter grouped under the three headings Case detection, Treatment, and Monitoring. It is a testament to the enduring nature of the first edition that so much CASE DETECTION, TREA material has been retained unchanged. At the same time, the new edition has had not only to address the huge resurgence of tuber- culosis, the emergence of multidrug-resistant bacilli, and the special needs of HIV-infected individuals with tuberculosis, but also to encompass significant scientific advances. These changes in the profile of the disease and in approaches to management have inevitably prompted many new questions and answers and given a different complexion to others. Toman’s Tuberculosis remains essential reading for all who need to AND MONITORING TMENT, QUESTIONS learn more about every aspect of tuberculosis – case-finding, manage- ment, and effective control strategies. It provides invaluable support AND to anyone in the front line of the battle against this disease, from ANSWERS programme managers to policy-makers and from medical personnel to volunteer health workers. SECOND EDITION ISBN 92 4 154603 4 WORLD HEALTH ORGANIZATION WHO GENEVA Toman’s Tuberculosis Case detection, treatment, and monitoring – questions and answers SECOND EDITION Edited by T. Frieden WORLD HEALTH ORGANIZATION GENEVA 2004 WHO Library Cataloguing-in-Publication Data Toman’s tuberculosis case detection, treatment, and monitoring : questions and answers / edited by T. -

Translational Deep Phenotyping of Deaths Related to the COVID-19 Pandemic: Protocol for a Prospective Observational Autopsy Study
Open access Protocol BMJ Open: first published as 10.1136/bmjopen-2021-049083 on 27 August 2021. Downloaded from Translational deep phenotyping of deaths related to the COVID-19 pandemic: protocol for a prospective observational autopsy study Mikkel Jon Henningsen ,1 Apameh Khatam- Lashgari,1 Kristine Boisen Olsen,1 Christina Jacobsen,1 Christian Beltoft Brøchner ,2 Jytte Banner1 To cite: Henningsen MJ, ABSTRACT Strengths and limitations of this study Khatam- Lashgari A, Olsen KB, Introduction The COVID-19 pandemic is an international et al. Translational deep emergency with an extreme socioeconomic impact and a ► A standardised, prospective autopsy study on COVID- phenotyping of deaths high mortality and disease burden. The COVID-19 outbreak related to the COVID-19 19- related deaths with systematic data collection. is neither fully understood nor fully pictured. Autopsy studies pandemic: protocol for a ► A multidisciplinary, translational approach elucidat- can help understand the pathogenesis of COVID-19 and has prospective observational ing changes from protein level to whole human. already resulted in better treatment of patients. Structured autopsy study. BMJ Open ► A comprehensive biobank and extensive registry and systematic autopsy of COVID-19- related deaths will 2021;11:e049083. doi:10.1136/ data as an umbrella for planned and future research. bmjopen-2021-049083 enhance the mapping of pathophysiological pathways, not ► The internal control group partly compensates for possible in the living. Furthermore, it provides an opportunity Prepublication history and the observational design. ► to envision factors translationally for the purpose of disease additional supplemental material ► Limited by a selected sample of COVID-19 diseased prevention in this and future pandemics. -

Treatment and Outcomes of Community-Acquired Pneumonia at Canadian Hospitals Research Brian G
Treatment and outcomes of community-acquired pneumonia at Canadian hospitals Research Brian G. Feagan,* Thomas J. Marrie,† Catherine Y. Lau,‡ Recherche Susan L. Wheeler,‡ Cindy J. Wong,* Margaret K. Vandervoort* From *the London Clinical Abstract Trials Research Group, London, Ont.; †the Background: Community-acquired pneumonia is a common disease with a large Department of Medicine, economic burden. We assessed clinical practices and outcomes among patients University of Alberta, with community-acquired pneumonia admitted to Canadian hospitals. Edmonton, Alta.; Methods: A total of 20 hospitals (11 teaching and 9 community) participated. Data and ‡Janssen–Ortho from the charts of adults admitted during November 1996, January 1997 and Incorporated, Toronto, Ont. March 1997 were reviewed to determine length of stay (LOS), admission to an intensive care unit and 30-day in-hospital mortality. Multivariate analyses exam- This article has been peer reviewed. ined sources of variability in LOS. The type and duration of antibiotic therapy and the proportion of patients who were treated according to clinical practice CMAJ 2000;162(10):1415-20 guidelines were determined. Results: A total of 858 eligible patients were identified; their mean age was 69.4 (standard deviation 17.7) years. The overall median LOS was 7.0 days (in- terquartile range [IQR] 4.0–11.0 days); the median LOS ranged from 5.0 to 9.0 days across hospitals (IQR 6.0–7.8 days). Only 22% of the variability in LOS could be explained by known factors (disease severity 12%; presence of chronic obstructive lung disease or bacterial cause for the pneumonia 2%; hospital site 7%). -
The Respiratory System
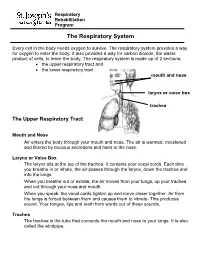
Respiratory Rehabilitation Program The Respiratory System Every cell in the body needs oxygen to survive. The respiratory system provides a way for oxygen to enter the body. It also provides a way for carbon dioxide, the waste product of cells, to leave the body. The respiratory system is made up of 2 sections: the upper respiratory tract and the lower respiratory tract mouth and nose larynx or voice box trachea The Upper Respiratory Tract Mouth and Nose Air enters the body through your mouth and nose. The air is warmed, moistened and filtered by mucous secretions and hairs in the nose. Larynx or Voice Box The larynx sits at the top of the trachea. It contains your vocal cords. Each time you breathe in or inhale, the air passes through the larynx, down the trachea and into the lungs. When you breathe out or exhale, the air moves from your lungs, up your trachea and out through your nose and mouth. When you speak, the vocal cords tighten up and move closer together. Air from the lungs is forced between them and causes them to vibrate. This produces sound. Your tongue, lips and teeth form words out of these sounds. Trachea The trachea is the tube that connects the mouth and nose to your lungs. It is also called the windpipe. The Lower Respiratory Tract Inside Lungs Outside Lungs bronchial tubes alveoli diaphragm (muscle) Bronchial Tubes The trachea splits into 2 bronchial tubes in your lungs. These are called the left bronchus and right bronchus. The bronchus tubes keep branching off into smaller and smaller tubes called bronchi. -

RESPIRATORY TRACT INFECTIONS Peter Zajac, DO, FACOFP, Author Amy J
OFP PATIENT EDUCATION HANDOUT RESPIRATORY TRACT INFECTIONS Peter Zajac, DO, FACOFP, Author Amy J. Keenum, DO, PharmD, Editor • Ronald Januchowski, DO, FACOFP, Health Literacy Editor HOME MANAGEMENT INCLUDES: • Drinking plenty of clear fuids and rest. Vitamin-C may help boost your immune system. Over-the-counter pain relievers such as acetaminophen and ibuprofen can be helpful for fevers and to ease any aches. Saline (salt) nose drops, lozenges, and vapor rubs can also help symptoms when used as directed by your physician. • A cool mist humidifer can make breathing easier by thinning mucus. • If you smoke, you should try to stop smoking for good! Avoid second-hand smoking also. • In most cases, antibiotics are not recommended because they are only effective if bacteria caused the infection. • Other treatments, that your Osteopathic Family Physician may prescribe, include Osteopathic Manipulative Therapy (OMT). OMT can help clear mucus, Respiratory tract infections are any relieve congestion, improve breathing and enhance comfort, relaxation, and infection that affect the nose, sinuses, immune function. and throat (i.e. the upper respiratory tract) or airways and lungs (i.e. the • Generally, the symptoms of a respiratory tract infection usually pass within lower respiratory tract). Viruses are one to two weeks. the main cause of the infections, but • To prevent spreading infections, sneeze into the arm of your shirt or in a tissue. bacteria can cause some. You can Also, practice good hygiene such as regularly washing your hands with soap and spread the infection to others through warm water. Wipe down common surfaces, such as door knobs and faucet handles, the air when you sneeze or cough. -

Control of Breathing in Mechanically Ventilated Patients
Eur Respir J, 1996, 9, 2151–2160 Copyright ERS Journals Ltd 1996 DOI: 10.1183/09031936.96.09102151 European Respiratory Journal Printed in UK - all rights reserved ISSN 0903 - 1936 SERIES "CLINICAL PHYSIOLOGY IN RESPIRATORY INTENSIVE CARE" Edited by A. Rossi and C. Roussos Control of breathing in mechanically ventilated patients D. Georgopoulos, C. Roussos Control of breathing in mechanically ventilated patients. D. Georgopoulos, C. Roussos. Pulmonary and Critical Care Dept, General ©ERS Journals Ltd 1996. Hospital "G. Papanicolaou", University of ABSTRACT: During mechanical ventilation, the respiratory system is under the Thessaloniki, Thessaloniki, Greece and influence of two pumps, the ventilator pump and the patient's own respiratory Critical Care Dept, "Evangelismos" Hospital, muscles. Depending on the mode of mechanical ventilatory support, ventilation University of Athens, Athens, Greece. may be totally controlled by the ventilator or may be determined by the interac- Correspondence: D. Georgopoulos tion between patient respiratory effort and ventilator function. In either case, com- General Hospital "G. Papanicolaou" pared to spontaneous breathing, the breathing pattern is altered and this may Pulmonary Dept influence: 1) force-length and force-velocity relationships of respiratory muscles Respiratory Failure Unit (mechanical feedback); 2) chemical stimuli (chemical feedback); 3) the activity of Exochi 57010 various receptors located in the respiratory tract, lung and chest wall (reflex feed- Thessaloniki back); and 4) behavioural response (behavioural feedback). Changes in these feed- Greece back systems may modify the function of the ventilator, in a way that is dependent Keywords: Behavioural feedback on the mode of mechanical ventilatory support, ventilator settings, mechanics of chemical feedback the respiratory system and the sleep/awake stage. -

2017 Pulmonary Coding and Payment Quick Reference
2017 Coding & Payment Quick Reference Select Pulmonary Procedures Payer policies will vary and should be verified prior to treatment for limitations on diagnosis, coding or site of service requirements. The coding options listed within this guide are commonly used codes and are not intended to be an all-inclusive list. We recommend consulting your relevant manuals for appropriate coding options. Medicare Physician, Hospital Outpatient, and ASC Payments The bronchoscopy procedures listed below (except CPT® Codes 31622, 31660, and 31661) all include a diagnostic bronchoscopy when performed by the same physician. 2017 Medicare National Average Payment RVUs Physician‡,2 Facility3 CPT® Total Total Hospital Code Description Work In-Office In-Facility ASC Code1 Office Facility Outpatient Biopsy 31625 Bronchoscopy, rigid or flexible, including fluoroscopic guidance, 3.11 9.43 4.53 $338 $163 $1,270† $569 when performed; with bronchial or endobronchial biopsy(s), single or multiple sites 31628 Bronchoscopy, rigid or flexible, including fluoroscopic guidance, 3.55 10.00 5.09 $359 $183 $2,431† $1,117 when performed; with transbronchial lung biopsy(s), single lobe 31632 Bronchoscopy, rigid or flexible, including fluoroscopic guidance, 1.03 1.84 1.42 $66 $51 $0 $0 when performed; with transbronchial lung biopsy(s), each additional lobe (List separately in addition to code for primary procedure)* Cytology and Brush 31622 Bronchoscopy, rigid or flexible, including fluoroscopic guidance, 2.53 6.86 3.81 $246 $137 $1,270† $569 when performed; diagnostic, -

Community Acquired Pneumonia
Community Acquired Pneumonia MELISSA PALMER AGACNP Objectives Know the target population for the 2019 American Thoracic Society and Infectious Diseases Society of America (ATS/IDSA) Community-acquired Pneumonia (CAP) guidelines 2019 Know when to perform testing for CAP: sputum cultures, blood cultures, Legionella and pneumococcal urinary antigen testing, influenza testing, and procalcitonin Be able to discuss the utilization of steroids in patients with CAP Know the selection of initial empiric antibiotic therapy for community-acquired pneumonia and duration of treatment for inpatients Criteria for hospitalization versus the need for ICU admission in adults diagnosed with CAP based on Pneumonia severity index (PSI) compared to CURB-65 Discuss the differences between the 2019 and 2007 ATS/IDSA Community-acquired Pneumonia Guidelines. COVID-19 Identify and Isolate. Pneumonia and CAP definition Pneumonia Infection of the alveoli, distal airways and the interstitium of the lung. Clinical: a new or changing radiographic density (infiltrate). Usually accompanied by constitutional symptoms of lung inflammation. Community Acquired Pneumonia acquired outside the hospital Signs and symptoms of pneumonia with radiographic confirmation *Patient must not have been hospitalized nor resided in a long-term-care facility for, at minimum, 14 days prior to the onset of symptoms Impact of Pneumonia leading infectious cause of hospitalization and death among U.S. adults more than 1.5 million adults hospitalized annually medical costs exceeding -

IDSA/ATS Consensus Guidelines on The
SUPPLEMENT ARTICLE Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults Lionel A. Mandell,1,a Richard G. Wunderink,2,a Antonio Anzueto,3,4 John G. Bartlett,7 G. Douglas Campbell,8 Nathan C. Dean,9,10 Scott F. Dowell,11 Thomas M. File, Jr.12,13 Daniel M. Musher,5,6 Michael S. Niederman,14,15 Antonio Torres,16 and Cynthia G. Whitney11 1McMaster University Medical School, Hamilton, Ontario, Canada; 2Northwestern University Feinberg School of Medicine, Chicago, Illinois; 3University of Texas Health Science Center and 4South Texas Veterans Health Care System, San Antonio, and 5Michael E. DeBakey Veterans Affairs Medical Center and 6Baylor College of Medicine, Houston, Texas; 7Johns Hopkins University School of Medicine, Baltimore, Maryland; 8Division of Pulmonary, Critical Care, and Sleep Medicine, University of Mississippi School of Medicine, Jackson; 9Division of Pulmonary and Critical Care Medicine, LDS Hospital, and 10University of Utah, Salt Lake City, Utah; 11Centers for Disease Control and Prevention, Atlanta, Georgia; 12Northeastern Ohio Universities College of Medicine, Rootstown, and 13Summa Health System, Akron, Ohio; 14State University of New York at Stony Brook, Stony Brook, and 15Department of Medicine, Winthrop University Hospital, Mineola, New York; and 16Cap de Servei de Pneumologia i Alle`rgia Respirato`ria, Institut Clı´nic del To`rax, Hospital Clı´nic de Barcelona, Facultat de Medicina, Universitat de Barcelona, Institut d’Investigacions Biome`diques August Pi i Sunyer, CIBER CB06/06/0028, Barcelona, Spain. EXECUTIVE SUMMARY priate starting point for consultation by specialists. Substantial overlap exists among the patients whom Improving the care of adult patients with community- these guidelines address and those discussed in the re- acquired pneumonia (CAP) has been the focus of many cently published guidelines for health care–associated different organizations, and several have developed pneumonia (HCAP). -
Introduction to the Respiratory System
C h a p t e r 15 The Respiratory System PowerPoint® Lecture Slides prepared by Jason LaPres Lone Star College - North Harris Copyright © 2010 Pearson Education, Inc. Copyright © 2010 Pearson Education, Inc. Introduction to the Respiratory System • The Respiratory System – Cells produce energy: • For maintenance, growth, defense, and division • Through mechanisms that use oxygen and produce carbon dioxide Copyright © 2010 Pearson Education, Inc. Introduction to the Respiratory System • Oxygen – Is obtained from the air by diffusion across delicate exchange surfaces of the lungs – Is carried to cells by the cardiovascular system, which also returns carbon dioxide to the lungs Copyright © 2010 Pearson Education, Inc. 15-1 The respiratory system, composed of conducting and respiratory portions, has several basic functions Copyright © 2010 Pearson Education, Inc. Functions of the Respiratory System • Provides extensive gas exchange surface area between air and circulating blood • Moves air to and from exchange surfaces of lungs • Protects respiratory surfaces from outside environment • Produces sounds • Participates in olfactory sense Copyright © 2010 Pearson Education, Inc. Components of the Respiratory System • The Respiratory Tract – Consists of a conducting portion • From nasal cavity to terminal bronchioles – Consists of a respiratory portion • The respiratory bronchioles and alveoli The Respiratory Tract Copyright © 2010 Pearson Education, Inc. Components of the Respiratory System • Alveoli – Are air-filled pockets within the lungs: