Epidemiological and Molecular Analysis of Virulence and Antibiotic Resistance in Acinetobacter Baumannii
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Insight Into the Resistome and Quorum Sensing System of a Divergent Acinetobacter Pittii Isolate from an Untouched Site of the Lechuguilla Cave
bioRxiv preprint doi: https://doi.org/10.1101/745182; this version posted August 28, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Insight into the resistome and quorum sensing system of a divergent Acinetobacter pittii isolate from an untouched site of the Lechuguilla Cave Han Ming Gan1,2,3*, Peter Wengert4 ,Trevor Penix4, Hazel A. Barton5, André O. Hudson4 and Michael A. Savka4 1 Centre for Integrative Ecology, School of Life and Environmental Sciences, Deakin University, Geelong 3220 ,Victoria, Australia 2 Deakin Genomics Centre, Deakin University, Geelong 3220 ,Victoria, Australia 3 School of Science, Monash University Malaysia, Bandar Sunway, 47500 Petaling Jaya, Selangor, Malaysia 4 Thomas H. Gosnell School of Life Sciences, Rochester Institute of Technology, Rochester, NY, USA 5 Department of Biology, University of Akron, Akron, Ohio, USA *Corresponding author Name: Han Ming Gan Email: [email protected] Key words Acinetobacter, quorum sensing, antibiotic resistance Abstract Acinetobacter are Gram-negative bacteria belonging to the sub-phyla Gammaproteobacteria, commonly associated with soils, animal feeds and water. Some members of the Acinetobacter have been implicated in hospital-acquired infections, with broad-spectrum antibiotic resistance. Here we report the whole genome sequence of LC510, an Acinetobacter species isolated from deep within a pristine location of the Lechuguilla Cave. Pairwise nucleotide comparison to three type strains within Acinetobacter assigned LC510 as an Acinetobacter pittii isolate. Scanning of the LC510 genome identified two genes coding for β-lactamase resistance, despite the fact that LC510 was isolated from a portion of the cave not previously visited by humans and protected from anthropogenic input. -
Insight Into the Resistome and Quorum Sensing System of a Divergent Acinetobacter Pittii Isolate from 1 an Untouched Site Of
bioRxiv preprint doi: https://doi.org/10.1101/745182; this version posted November 27, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Insight into the resistome and quorum sensing system of a divergent Acinetobacter pittii isolate from 2 an untouched site of the Lechuguilla Cave 3 4 Han Ming Gan1,2,3*, Peter Wengert4 , Hazel A. Barton5, André O. Hudson4 and Michael A. Savka4 5 1 Centre for Integrative Ecology, School of Life and Environmental Sciences, Deakin University, Geelong 6 3220 ,Victoria, Australia 7 2 Deakin Genomics Centre, Deakin University, Geelong 3220 ,Victoria, Australia 8 3 School of Science, Monash University Malaysia, Bandar Sunway, 47500 Petaling Jaya, Selangor, 9 Malaysia 10 4 Thomas H. Gosnell School of Life Sciences, Rochester Institute of Technology, Rochester, NY, USA 11 5 Department of Biology, University of Akron, Akron, Ohio, USA 12 *Corresponding author 13 Name: Han Ming Gan 14 Email: [email protected] 15 Key words 16 Acinetobacter, quorum sensing, antibiotic resistance 17 18 Abstract 19 Acinetobacter are Gram-negative bacteria belonging to the sub-phyla Gammaproteobacteria, commonly 20 associated with soils, animal feeds and water. Some members of the Acinetobacter have been 21 implicated in hospital-acquired infections, with broad-spectrum antibiotic resistance. Here we report the 22 whole genome sequence of LC510, an Acinetobacter species isolated from deep within a pristine 23 location of the Lechuguilla Cave. -

Evolutionary Genomics of Conjugative Elements and Integrons
Université Paris Descartes École doctorale Interdisciplinaire Européenne 474 Frontières du Vivant Microbial Evolutionary Genomic, Pasteur Institute Evolutionary genomics of conjugative elements and integrons Thèse de doctorat en Biologie Interdisciplinaire Présentée par Jean Cury Pour obtenir le grade de Docteur de l’Université Paris Descartes Sous la direction de Eduardo Rocha Soutenue publiquement le 17 Novembre 2017, devant un jury composé de: Claudine MÉDIGUE Rapporteure CNRS, Genoscope, Évry Marie-Cécile PLOY Rapporteure Université de Limoges Érick DENAMUR Examinateur Université Paris Diderot, Paris Philippe LOPEZ Examinateur Université Pierre et Marie Curie, Paris Alan GROSSMAN Examinateur MIT, Cambdridge, USA Eduardo ROCHA Directeur de thèse CNRS, Institut Pasteur, Paris ِ عمحمود ُبدرويش َالنرد َم ْن انا ِٔ َقول ُلك ْم ما ا ُقول ُلك ْم ؟ وانا لم أ ُك ْن َ َج ًرا َص َق َل ْت ُه ُالمياه َفأ ْص َب َح ِوهاً و َق َصباً َثق َب ْت ُه ُالرياح َفأ ْص َب َح ًنايا ... انا ِع ُب َالن ْرد ، ا َرب ُح يناً وا َس ُر يناً انا ِم ُثل ُك ْم ا وا قل قليً ... The dice player Mahmoud Darwish Who am I to say to you what I am saying to you? I was not a stone polished by water and became a face nor was I a cane punctured by the wind and became a lute… I am a dice player, Sometimes I win and sometimes I lose I am like you or slightly less… Contents Acknowledgments 7 Preamble 9 I Introduction 11 1 Background for friends and family . 13 2 Horizontal Gene Transfer (HGT) . 16 2.1 Mechanisms of horizontal gene transfer . -

The Microbiota Continuum Along the Female Reproductive Tract and Its Relation to Uterine-Related Diseases
ARTICLE DOI: 10.1038/s41467-017-00901-0 OPEN The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases Chen Chen1,2, Xiaolei Song1,3, Weixia Wei4,5, Huanzi Zhong 1,2,6, Juanjuan Dai4,5, Zhou Lan1, Fei Li1,2,3, Xinlei Yu1,2, Qiang Feng1,7, Zirong Wang1, Hailiang Xie1, Xiaomin Chen1, Chunwei Zeng1, Bo Wen1,2, Liping Zeng4,5, Hui Du4,5, Huiru Tang4,5, Changlu Xu1,8, Yan Xia1,3, Huihua Xia1,2,9, Huanming Yang1,10, Jian Wang1,10, Jun Wang1,11, Lise Madsen 1,6,12, Susanne Brix 13, Karsten Kristiansen1,6, Xun Xu1,2, Junhua Li 1,2,9,14, Ruifang Wu4,5 & Huijue Jia 1,2,9,11 Reports on bacteria detected in maternal fluids during pregnancy are typically associated with adverse consequences, and whether the female reproductive tract harbours distinct microbial communities beyond the vagina has been a matter of debate. Here we systematically sample the microbiota within the female reproductive tract in 110 women of reproductive age, and examine the nature of colonisation by 16S rRNA gene amplicon sequencing and cultivation. We find distinct microbial communities in cervical canal, uterus, fallopian tubes and perito- neal fluid, differing from that of the vagina. The results reflect a microbiota continuum along the female reproductive tract, indicative of a non-sterile environment. We also identify microbial taxa and potential functions that correlate with the menstrual cycle or are over- represented in subjects with adenomyosis or infertility due to endometriosis. The study provides insight into the nature of the vagino-uterine microbiome, and suggests that sur- veying the vaginal or cervical microbiota might be useful for detection of common diseases in the upper reproductive tract. -

Elucidation of Spatiotemporal Variations in Functional Genes Involved in the Nitrogen Cycle Along the West Coast of India
Elucidation of spatiotemporal variations in functional genes involved in the nitrogen cycle along the west coast of India A thesis submitted to Goa University for the award of degree of Doctor of Philosophy In MICROBIOLOGY By JASMINE GOMES Under the guidance of Dr. RAKHEE KHANDEPARKER Senior Scientist Biological Oceanography Division CSIR-National Institute of Oceanography Dona Paula-Goa 403004 April 2018 CERTIFICATE Certified that the research work embodied in this thesis entitled ―Elucidation of spatiotemporal variations in functional genes involved in the nitrogen cycle along the west coast of India‖ submitted by Ms. Jasmine Gomes for the award of Doctor of Philosophy degree in Microbiology at Goa University, Goa, is the original work carried out by the candidate himself under my supervision and guidance. Dr. Rakhee Khandeparker Senior Scientist Biological Oceanography Division CSIR-National Institute of Oceanography, Dona Paula – Goa 403004 DECLARATION As required under the University ordinance, I hereby state that the present thesis for Ph.D. degree entitled ―Elucidation of spatiotemporal variations in functional genes involved in the nitrogen cycle along the west coast of India" is my original contribution and that the thesis and any part of it has not been previously submitted for the award of any degree/diploma of any University or Institute. To the best of my knowledge, the present study is the first comprehensive work of its kind from this area. The literature related to the problem investigated has been cited. Due acknowledgement have been made whenever facilities and suggestions have been availed of. JASMINE GOMES Acknowledgment I take this privilege to express my heartfelt thanks to everyone involved to complete my Ph.D successfully. -

Update on the Epidemiology, Treatment, and Outcomes of Carbapenem-Resistant Acinetobacter Infections
Review Article www.cmj.ac.kr Update on the Epidemiology, Treatment, and Outcomes of Carbapenem-resistant Acinetobacter infections Uh Jin Kim, Hee Kyung Kim, Joon Hwan An, Soo Kyung Cho, Kyung-Hwa Park and Hee-Chang Jang* Department of Infectious Diseases, Chonnam National University Medical School, Gwangju, Korea Carbapenem-resistant Acinetobacter species are increasingly recognized as major no- Article History: socomial pathogens, especially in patients with critical illnesses or in intensive care. received 18 July, 2014 18 July, 2014 The ability of these organisms to accumulate diverse mechanisms of resistance limits revised accepted 28 July, 2014 the available therapeutic agents, makes the infection difficult to treat, and is associated with a greater risk of death. In this review, we provide an update on the epidemiology, Corresponding Author: resistance mechanisms, infection control measures, treatment, and outcomes of carba- Hee-Chang Jang penem-resistant Acinetobacter infections. Department of Infectious Diseases, Chonnam National University Medical Key Words: Acinetobacter baumannii; Colistin; Drug therapy School, 160, Baekseo-ro, Dong-gu, Gwangju 501-746, Korea This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial TEL: +82-62-220-6296 License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, FAX: +82-62-225-8578 distribution, and reproduction in any medium, provided the original work is properly cited. E-mail: [email protected] INTRODUCTION species by their phenotypic traits is difficult, and identi- fication of individual species by use of current automated Acinetobacter species are aerobic gram-negative bacilli or manual commercial systems will require further con- that are ubiquitous in natural environments such as soil firmation testing. -

Etude De L'épidémiologie Moléculaire Et De L'écologie D'acinetobacter Spp
Etude de l’épidémiologie moléculaire et de l’écologie d’Acinetobacter spp au Liban Ahmad Al Atrouni To cite this version: Ahmad Al Atrouni. Etude de l’épidémiologie moléculaire et de l’écologie d’Acinetobacter spp au Liban. Médecine humaine et pathologie. Université d’Angers; Université libannaise de Beyrouth, 2017. Français. NNT : 2017ANGE0004. tel-01599268 HAL Id: tel-01599268 https://tel.archives-ouvertes.fr/tel-01599268 Submitted on 2 Oct 2017 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. AHMAD AL ATROUNI Mémoire présenté en vue de l’obtention du grade de Docteur de l'Université d'Angers sous le sceau de l’Université Bretagne Loire École doctorale : Ecole Doctorale Biologie Santé Discipline : Microbiologie Spécialité : Microbiologie Unité de recherche : ATOMycA, Inserm Atip-Avenir Team, CRCNA, Inserm U892, 6299 CNRS, Angers, France ET L’Université Libanaise École doctorale : Sciences et Technologie Spécialité :Microbiologie Medicale et Alimentaire Unité de recherche: Laboratoire de Microbiologie Santé et Environnement Soutenue le 19 Mai 2017 -
Cultivation-Based Quantification and Identification of Bacteria at Two
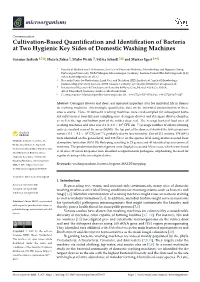
microorganisms Communication Cultivation-Based Quantification and Identification of Bacteria at Two Hygienic Key Sides of Domestic Washing Machines Susanne Jacksch 1,2 , Huzefa Zohra 1, Mirko Weide 3, Sylvia Schnell 2 and Markus Egert 1,* 1 Faculty of Medical and Life Sciences, Institute of Precision Medicine, Microbiology and Hygiene Group, Furtwangen University, 78054 Villingen-Schwenningen, Germany; [email protected] (S.J.); [email protected] (H.Z.) 2 Research Centre for BioSystems, Land Use, and Nutrition (IFZ), Institute of Applied Microbiology, Justus-Liebig-University Giessen, 35392 Giessen, Germany; [email protected] 3 International Research & Development–Laundry & Home Care, Henkel AG & Co. KGaA, 40191 Düsseldorf, Germany; [email protected] * Correspondence: [email protected]; Tel.: +49-(7720)-307-4554; Fax: +49-(7720)-307-4207 Abstract: Detergent drawer and door seal represent important sites for microbial life in domes- tic washing machines. Interestingly, quantitative data on the microbial contamination of these sites is scarce. Here, 10 domestic washing machines were swab-sampled for subsequent bacte- rial cultivation at four different sampling sites: detergent drawer and detergent drawer chamber, as well as the top and bottom part of the rubber door seal. The average bacterial load over all washing machines and sites was 2.1 ± 1.0 × 104 CFU cm−2 (average number of colony forming units ± standard error of the mean (SEM)). The top part of the door seal showed the lowest contami- 1 −2 nation (11.1 ± 9.2 × 10 CFU cm ), probably due to less humidity. Out of 212 isolates, 178 (84%) were identified on the genus level, and 118 (56%) on the species level using matrix-assisted laser Citation: Jacksch, S.; Zohra, H.; desorption/ionization (MALDI) Biotyping, resulting in 29 genera and 40 identified species across all Weide, M.; Schnell, S.; Egert, M. -

International Journal of Systematic and Evolutionary Microbiology
International Journal of Systematic and Evolutionary Microbiology Acinetobacter dijkshoorniae sp. nov., a new member of the Acinetobacter calcoaceticus-Acinetobacter baumannii complex mainly recovered from clinical samples in different countries --Manuscript Draft-- Manuscript Number: IJSEM-D-16-00397R2 Full Title: Acinetobacter dijkshoorniae sp. nov., a new member of the Acinetobacter calcoaceticus-Acinetobacter baumannii complex mainly recovered from clinical samples in different countries Short Title: Acinetobacter dijkshoorniae sp. nov. Article Type: Note Section/Category: New taxa - Proteobacteria Keywords: ACB complex; MLSA; rpoB; ANIb; Acinetobacter Corresponding Author: Ignasi Roca, Ph.D Institut de Salut Global de Barcelona(ISGlobal) Barcelona, Barcelona SPAIN First Author: Clara Cosgaya Order of Authors: Clara Cosgaya Marta Marí-Almirall Ado Van Assche Dietmar Fernández-Orth Noraida Mosqueda Murat Telli Geert Huys Paul G. Higgins Harald Seifert Bart Lievens Ignasi Roca, Ph.D Jordi Vila Manuscript Region of Origin: SPAIN Abstract: The recent advances in bacterial species identification methods have led to the rapid taxonomic diversification of the genus Acinetobacter. In the present study, phenotypic and molecular methods have been used to determine the taxonomic position of a group of 12 genotypically distinct strains belonging to the Acinetobacter calcoaceticus- Acinetobacter baumannii (ACB) complex, initially described by Gerner-Smidt and Tjernberg in 1993, that are closely related to A. pittii. Strains characterized in this study originated mostly from human samples obtained in different countries over a period of 15 years. rpoB and MLST sequences were compared against those of 94 strains representing all species included in the ACB complex. Cluster analysis based on such sequences showed that all 12 strains grouped together in a distinct clade closest to A. -

Exploring the Microbiome: Diversity of the Microbial Community of Three Foam Nesting Frogs, Genus: Polypedates, Across a Developmental Gradient Sarah Mcgrath
James Madison University JMU Scholarly Commons Masters Theses The Graduate School Summer 2018 Exploring the microbiome: diversity of the microbial community of three foam nesting frogs, Genus: Polypedates, across a developmental gradient Sarah McGrath Follow this and additional works at: https://commons.lib.jmu.edu/master201019 Part of the Environmental Microbiology and Microbial Ecology Commons, and the Other Microbiology Commons Recommended Citation McGrath, Sarah, "Exploring the microbiome: diversity of the microbial community of three foam nesting frogs, Genus: Polypedates, across a developmental gradient" (2018). Masters Theses. 575. https://commons.lib.jmu.edu/master201019/575 This Thesis is brought to you for free and open access by the The Graduate School at JMU Scholarly Commons. It has been accepted for inclusion in Masters Theses by an authorized administrator of JMU Scholarly Commons. For more information, please contact [email protected]. Exploring the microbiome: diversity of the microbial community of three foam nesting frogs, Genus: Polypedates, across a developmental gradient Sarah McGrath A thesis submitted to the Graduate Faculty of JAMES MADISON UNIVERSITY In Partial Fulfillment of the Requirements for the degree of Master of Science Department of Biology August 2018 FACULTY COMMITTEE: Committee Chair: Dr. David S. McLeod Committee Members/Readers: Dr. Morgan Steffen Dr. Reid Harris Dedication This work is dedicated to my father, John Robinson McGrath, for instilling in me a love of nature; my mother, Susanna Terrell McGrath, for continuously demonstrating that hard work pays off; Nicholas Blaser, for being an unwavering source of support; and Jennifer A. Sheridan, for providing me with my first opportunity to fully understand the demand and intricacy of tropical fieldwork. -
Identification, Molecular Epidemiology, and Antibiotic Resistance Characterization of Acinetobacter Spp
FACULTY OF HEALTH SCIENCES DEPARTMENT OF MEDICAL BIOLOGY UNIVERSITY HOSPITAL OF NORTH NORWAY DEPARTMENT OF MICROBIOLOGY AND INFECTION CONTROL REFERENCE CENTRE FOR DETECTION OF ANTIMICROBIAL RESISTANCE Identification, molecular epidemiology, and antibiotic resistance characterization of Acinetobacter spp. clinical isolates Nabil Karah A dissertation for the degree of Philosophiae Doctor June 2011 Acknowledgments The work presented in this thesis has been carried out between January 2009 and September 2011 at the Reference Centre for Detection of Antimicrobial Resistance (K-res), Department of Microbiology and Infection Control, University Hospital of North Norway (UNN); and the Research Group for Host–Microbe Interactions, Department of Medical Biology, Faculty of Health Sciences, University of Tromsø (UIT), Tromsø, Norway. I would like to express my deep and truthful acknowledgment to my main supervisor Ørjan Samuelsen. His understanding and encouraging supervision played a major role in the success of every experiment of my PhD project. Dear Ørjan, I am certainly very thankful for your indispensible contribution in all the four manuscripts. I am also very grateful to your comments, suggestions, and corrections on the present thesis. I am sincerely grateful to my co-supervisor Arnfinn Sundsfjord for his important contribution not only in my MSc study and my PhD study but also in my entire career as a “Medical Microbiologist”. I would also thank you Arnfinn for your nonstop support during my stay in Tromsø at a personal level. My sincere thanks are due to co-supervisors Kristin Hegstad and Gunnar Skov Simonsen for the valuable advice, productive comments, and friendly support. I would like to thank co-authors Christian G. -
Comparative Genomic Analysis of Acinetobacter Strains Isolated From
Saffarian et al. BMC Genomics (2017) 18:525 DOI 10.1186/s12864-017-3925-x RESEARCHARTICLE Open Access Comparative genomic analysis of Acinetobacter strains isolated from murine colonic crypts Azadeh Saffarian1, Marie Touchon2, Céline Mulet1, Régis Tournebize3, Virginie Passet2, Sylvain Brisse2, Eduardo P. C. Rocha2, Philippe J. Sansonetti1,4 and Thierry Pédron1* Abstract Background: A restricted set of aerobic bacteria dominated by the Acinetobacter genus was identified in murine intestinal colonic crypts. The vicinity of such bacteria with intestinal stem cells could indicate that they protect the crypt against cytotoxic and genotoxic signals. Genome analyses of these bacteria were performed to better appreciate their biodegradative capacities. Results: Two taxonomically different clusters of Acinetobacter were isolated from murine proximal colonic crypts, one was identified as A. modestus and the other as A. radioresistens. Their identification was performed through biochemical parameters and housekeeping gene sequencing. After selection of one strain of each cluster (A. modestus CM11G and A. radioresistens CM38.2), comparative genomic analysis was performed on whole-genome sequencing data. The antibiotic resistance pattern of these two strains is different, in line with the many genes involved in resistance to heavy metals identified in both genomes. Moreover whereas the operon benABCDE involved in benzoate metabolism is encoded by the two genomes, the operon antABC encoding the anthranilate dioxygenase, and the phenol hydroxylase gene cluster are absent in the A. modestus genomic sequence, indicating that the two strains have different capacities to metabolize xenobiotics. A common feature of the two strains is the presence of a type IV pili system, and the presence of genes encoding proteins pertaining to secretion systems such as Type I and Type II secretion systems.