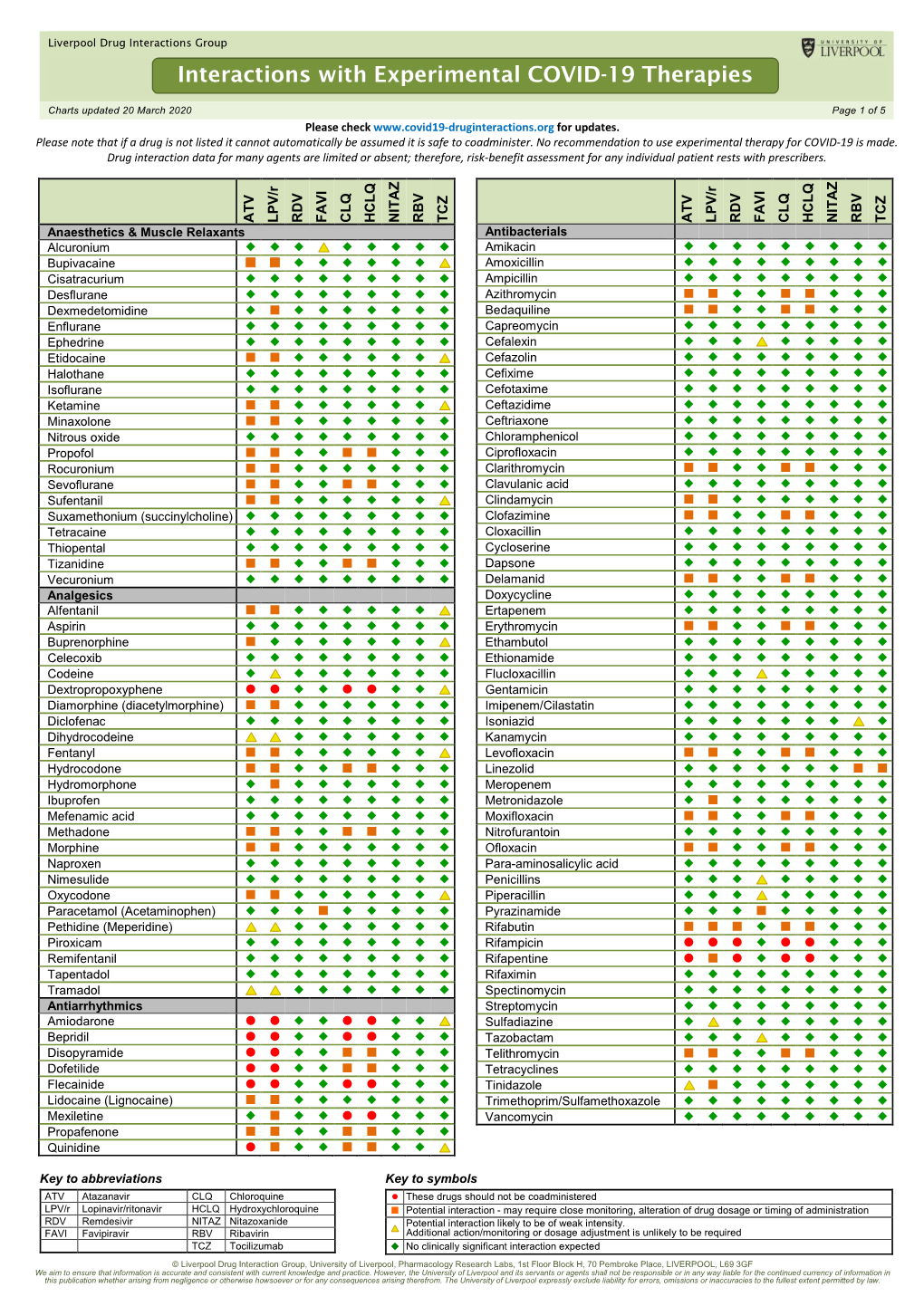
Interactions with Experimental COVID-19 Therapies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table 2. 2012 AGS Beers Criteria for Potentially
Table 2. 2012 AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults Strength of Organ System/ Recommendat Quality of Recomm Therapeutic Category/Drug(s) Rationale ion Evidence endation References Anticholinergics (excludes TCAs) First-generation antihistamines Highly anticholinergic; Avoid Hydroxyzin Strong Agostini 2001 (as single agent or as part of clearance reduced with e and Boustani 2007 combination products) advanced age, and promethazi Guaiana 2010 Brompheniramine tolerance develops ne: high; Han 2001 Carbinoxamine when used as hypnotic; All others: Rudolph 2008 Chlorpheniramine increased risk of moderate Clemastine confusion, dry mouth, Cyproheptadine constipation, and other Dexbrompheniramine anticholinergic Dexchlorpheniramine effects/toxicity. Diphenhydramine (oral) Doxylamine Use of diphenhydramine in Hydroxyzine special situations such Promethazine as acute treatment of Triprolidine severe allergic reaction may be appropriate. Antiparkinson agents Not recommended for Avoid Moderate Strong Rudolph 2008 Benztropine (oral) prevention of Trihexyphenidyl extrapyramidal symptoms with antipsychotics; more effective agents available for treatment of Parkinson disease. Antispasmodics Highly anticholinergic, Avoid Moderate Strong Lechevallier- Belladonna alkaloids uncertain except in Michel 2005 Clidinium-chlordiazepoxide effectiveness. short-term Rudolph 2008 Dicyclomine palliative Hyoscyamine care to Propantheline decrease Scopolamine oral secretions. Antithrombotics Dipyridamole, oral short-acting* May -

S Values in Accordance with Soczewiński-Wachtmeisters Equation
S values in accordance with Soczewiński-Wachtmeisters equation S value from Antiparasitic drugs: Soczewiński’s Metronidazole Ornidazole Secnidazole Tinidazole Equation* S(m) 1.614 2.161 1.921 1.911 S(a) 1.634 2.159 1.887 1.923 S value from Antihypertensive drugs: Soczewiński’s Nilvadipine Felodipine Isradipine Lacidipine equation 4.129 4.597 3.741 5.349 S(m) S(a) 5.330 4.841 4.715 5.690 S value from Non-steroidal anti-inflammatory drugs (NSAIDs): Soczewiński’s Mefenamic Indomethacin Nabumetone Phenylbutazone Carprofen Ketoprofen Flurbiprofen equation acid 2.879 2.773 3.456 2.682 2.854 2.139 2.568 S(m) 3.317 3.442 3.910 2.404 3.394 1.968 2.010 S(a) *where: S(m) – S is the slope of the regression curie in accordance with Soczewiński-Wachtmeisters equation using methanol-water mobile phase S(a) – S is the slope of the regression curie in accordance with Soczewiński-Wachtmeisters equation using acetone-water mobile phase First group of drugs (antiparasitic drugs) 1. Metronidazole (2-Methyl-5-nitroimidazole-1-ethanol) 2. Ornidazole (1-(3-Chloro-2-hydroxypropyl)-2-methyl-5-nitroimidazole) 3. Secnidazole (1-(2-methyl-5-nitro-1H-imidazol-1-yl) propan-2ol, 1-(2Hydroxypropyl)-2-methyl-5- nitroimidazole) 4. Tinidazole (1-[2-(Ethylsulfonyl)ethyl]-2-methyl-5-nitroimidazole) Second group of drugs (antihypertensive drugs) 1. Nilvadipine (2-Cyano-1,4-dihydro-6-methyl-4-(3-nitrophenyl)-3,5-pyridinedicarboxylic acid 3- methyl 5-(1-methylethyl) ester, 5-Isopropyl-3-methyl-2-cyano-1,4-dihydro-6-methyl-4-(m- nitrophenyl)-3,5-pyridinedicarboxylate, FK-235, FR-34235, Isopropyl 6-cyano-5-methoxycarbonyl-2- methyl-4-(3-nitrophenyl)-1,4-dihydropyridine-3-carboxylate) 2. -

Insomnia and Anxiety in Older People Sleeping Pills Are Usually Not the Best Solution
® Insomnia and anxiety in older people Sleeping pills are usually not the best solution lmost one-third of older people in the people who take one of United States take sleeping pills. These these medicines sleep medicines are also sometimes called only a little longer and A“sedative-hypnotics” or “tranquilizers.” They better than those who affect the brain and spinal cord. don’t take a medicine. Doctors prescribe some of these medicines Sleeping pills can for sleep problems. Some of these medicines have serious side effects. also can be used to treat other conditions, such All sedative-hypnotic medicines have special as anxiety or alcohol withdrawal. Sometimes, risks for older adults. Seniors are likely to be doctors also prescribe certain anti-depressants more sensitive to the medicines’ effects than for sleep, even though that’s not what they’re younger adults. And these medicines may designed to treat. stay in older people’s bodies longer. These Most older adults should first try to treat their medicines can cause confusion and memory insomnia without medicines. According to the problems that: American Geriatrics Society, there are safer and • Increase the risk of falls and hip fractures. better ways to improve sleep or reduce anxiety. These are common causes of hospital stays Here’s why: and death in older people. Sleeping pills may not help much. • Increase the risk of car accidents. Many ads say that sleeping pills help people get a full, restful night’s sleep. But studies show that this is not exactly true in real life. On average, The new “Z” medicines also have risks. -

Drug & Alcohol Testing Program
Pottawattmie County Drug & Alcohol Testing Program Appendix A Table of Contents POLICY STATEMENT ...................................................................................................................................... 3 SCOPE ............................................................................................................................................................ 4 EDUCATION AND TRAINING .......................................................................................................................... 4 DESIGNATED EMPLOYER REPRESENTATIVE (DER): ....................................................................................... 5 DUTY TO COOPERATE ................................................................................................................................... 5 EMPLOYEE ADMISSION OF ALCOHOL AND CONTROLLED SUBSTANCE USE: (49 CFR Part 382.121) ... 6 PROHIBITED DRUGS AND ILLEGALLY USED CONTROLLED SUBSTANCES: ..................................................... 7 PROHIBITED BEHAVIOR AND CONDUCT: ...................................................................................................... 8 DRUG & ALCOHOL TESTING REQUIREMENTS (49 CFR, Part 40 & 382) ............................................... 10 DRUG & ALCOHOL TESTING CIRCUMSTANCES (49 CFR Part 40 & 382) .............................................. 12 A. Pre-Employment Testing: .................................................................................................... 12 B. Reasonable Suspicion Testing: ......................................................................................... -

Dofetilide (Tikosyn): a New Drug to Control Atrial Fibrillation
CURRENT DRUG THERAPY WALID I. SALIBA, MD Section of Cardiac Electrophysiology and Pacing, CREDIT Department of Cardiology, Cleveland Clinic Dofetilide (Tikosyn): A new drug to control atrial fibrillation ABSTRACT OFETILIDE (Tikosyn), a new antiarrhyth- mic drug, can convert atrial fibrillation Dofetilide, a new class III antiarrhythmic agent, selectively and atrial flutter to sinus rhythm in approxi- blocks a specific cardiac potassium channel, lKr, increasing mately 30% of cases and maintain sinus the effective refractory period of the myocyte and thereby rhythm after electrical or pharmacologic con- terminating reentrant arrhythmias. Given orally, it appears version for up to 1 year in 60% to 70% of to effectively convert atrial fibrillation and atrial flutter to cases, without increasing the risk of sudden sinus rhythm and maintain sinus rhythm after conversion in death in patients at high risk. appropriately selected patients. This paper reviews the Such new drugs are needed, as many of the pharmacology of dofetilide, the evidence of its antiarrhythmic drugs in use up to now have effectiveness, and the appropriate precautions in using it. actually produced higher mortality rates in clinical trials than did placebo, or cause unac- ceptable side effects. KEY POINTS This article reviews the mechanism of action, safety, effectiveness, and clinical use of Dofetilide is generally well tolerated but like other class III dofetilide. drugs can cause torsades de pointes. The risk is dose- dependent and can be minimized by adjusting the dosage • PROBLEMS WITH PREVIOUS DRUGS according to creatinine clearance and QT interval, by excluding patients with known risk factors for long QT A variety of drugs have been used to terminate syndrome and torsades de pointes, and by starting or prevent atrial and ventricular arrhythmias, treatment in an inpatient monitored setting for the first 3 but their safety, efficacy, and tolerability in days. -

PACKAGE LEAFLET: INFORMATION for the USER Lercanidipine
PACKAGE LEAFLET: INFORMATION FOR THE USER Lercanidipine Hydrochloride 10 mg Film-coated Tablets Lercanidipine Hydrochloride 20 mg Film-coated Tablets lercanidipine hydrochloride Read all of this leaflet carefully before you start using this medicine because it contains important information for you. - Keep this leaflet. You may need to read it again. - If you have any further questions, ask your doctor or pharmacist. - This medicine has been prescribed for you only. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours. - If you get any of the side effects talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. See section 4. What is in this leaflet: 1. What Lercanidipine Hydrochloride Film-coated Tablets is and what it is used for 2. What you need to know before you take Lercanidipine Hydrochloride Film-coated Tablets 3. How to take Lercanidipine Hydrochloride Film-coated Tablets 4. Possible side effects 5. How to store Lercanidipine Hydrochloride Film-coated Tablets 6. Contents of the pack and other information 1. WHAT LERCANIDIPINE HYDROCHLORIDE FILM-COATED TABLETS IS AND WHAT IT IS USED FOR Lercanidipine belongs to a group of medicines called calcium channel blockers (dihydropyridine derivatives) that lower blood pressure.. Lercanidipine is used to treat high blood pressure also known as hypertension in adults over the age of 18 years (it is not recommended for children under 18 years old). 2. WHAT YOU NEED TO KNOW BEFORE YOU TAKE LERCANIDIPINE -

Management of Chronic Problems
MANAGEMENT OF CHRONIC PROBLEMS INTERACTIONS BETWEEN ALCOHOL AND DRUGS A. Leary,* T. MacDonald† SUMMARY concerned. Alcohol may alter the effects of the drug; drug In western society alcohol consumption is common as is may change the effects of alcohol; or both may occur. the use of therapeutic drugs. It is not surprising therefore The interaction between alcohol and drug may be that concomitant use of these should occur frequently. The pharmacokinetic, with altered absorption, metabolism or consequences of this combination vary with the dose of elimination of the drug, alcohol or both.2 Alcohol may drug, the amount of alcohol taken, the mode of affect drug pharmacokinetics by altering gastric emptying administration and the pharmacological effects of the drug or liver metabolism. Drugs may affect alcohol kinetics by concerned. Interactions may be pharmacokinetic or altering gastric emptying or inhibiting gastric alcohol pharmacodynamic, and while coincidental use of alcohol dehydrogenase (ADH).3 This may lead to altered tissue may affect the metabolism or action of a drug, a drug may concentrations of one or both agents, with resultant toxicity. equally affect the metabolism or action of alcohol. Alcohol- The results of concomitant use may also be principally drug interactions may differ with acute and chronic alcohol pharmacodynamic, with combined alcohol and drug effects ingestion, particularly where toxicity is due to a metabolite occurring at the receptor level without important changes rather than the parent drug. There is both inter- and intra- in plasma concentration of either. Some interactions have individual variation in the response to concomitant drug both kinetic and dynamic components and, where this is and alcohol use. -

Summary of Product Characteristics, Labelling and Package Leaflet
SUMMARY OF PRODUCT CHARACTERISTICS, LABELLING AND PACKAGE LEAFLET 1 SUMMARY OF PRODUCT CHARACTERISTICS 2 1. NAME OF THE MEDICINAL PRODUCT /.../ 10 mg film-coated tablet /.../ 20 mg film-coated tablet 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One film-coated tablet contains 10 mg lercanidipine hydrochloride, equivalent to 9.4 mg lercanidipine. One film-coated tablet contains 20 mg lercanidipine hydrochloride, equivalent to 18.8 mg lercanidipine. Excipient with known effect: /.../ 10 mg film-coated tablet: Lactose monohydrate 30 mg Excipient with known effect: /.../ 20 mg film-coated tablet: Lactose monohydrate 60 mg For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Film--coated tablet /.../ 10 mg film-coated tablet: Yellow, round, biconvex 6.5 mm film-coated tablets, scored on one side, marked 'L' on the other side. /.../ 20 mg film-coated tablet: Pink, round, biconvex 8.5 mm film-coated tablets, scored on one side, marked 'L' on the other side. The score line is only to facilitate breaking for ease of swallowing and not to divide into equal doses. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications /.../ is indicated for the treatment of mild to moderate essential hypertension. 4.2 Posology and method of administration Posology Route of administration: For oral use. The recommended dosage is 10 mg orally once a day at least 15 minutes before meals; the dose may be increased to 20 mg depending on the individual patient's response. Dose titration should be gradual, because it may take about 2 weeks before the maximal antihypertensive effect is apparent. Some individuals, not adequately controlled on a single antihypertensive agent, may benefit from the addition of lercandipine to therapy with a beta-adrenoreceptor blocking drug, a diuretic (hydrochlorothiazide) or an angiotensin converting enzyme inhibitor. -

Effect of Lacidipine and Nifedipine GITS on Platelet Function in Patients with Essential Hypertension
Journal of Human Hypertension (2000) 14, Suppl 1, S91–S95 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh Effect of lacidipine and nifedipine GITS on platelet function in patients with essential hypertension MC Armas-Padilla1, MJ Armas-Herna´ndez1, R Herna´ndez-Herna´ndez1, M Velasco2, B Pacheco1, AR Carvajal1 and A Castillo-Moreno1 1Clinical Pharmacology Unit, School of Medicine, Universidad Centroccidental Lisandro Alvarado, Barquisimeto, Venezuela; 2Clinical Pharmacology Unit, Vargas Medical School, Central University of Venezuela, Caracas, Venezuela With the aim of evaluating the effects on blood pressure, Both drugs reduced systolic and diastolic blood press- platelet function and insulin sensitivity of the dihydro- ure at the same level, however there were observable piridines lacidipine and nifedipine GITS, a parallel dou- differences in the rate of reduction. The nifedipine GITS ble-blind study was carried out in a group of 20 patients reduced supine systolic blood pressure by 25 mm Hg in with mild to moderate essential hypertension. They the first week, while the lacidipine did so by 11 mm Hg. received a placebo for 4 weeks; then were divided at At the end of the study period nifedipine reduced supine random into two groups of 10 patients each. Nifedipine systolic blood pressure by 28 mm Hg and lacidipine by GITS, 30 mg and lacidipine, 4 mg, were given during 16 20 mm Hg. Heart rate was increased slightly but signifi- weeks of active treatment. Blood pressure and heart cantly in the nifedipine GITS group only in the standing rate were measured at the clinic in supine, sitting and position. -

Classification of Medicinal Drugs and Driving: Co-Ordination and Synthesis Report
Project No. TREN-05-FP6TR-S07.61320-518404-DRUID DRUID Driving under the Influence of Drugs, Alcohol and Medicines Integrated Project 1.6. Sustainable Development, Global Change and Ecosystem 1.6.2: Sustainable Surface Transport 6th Framework Programme Deliverable 4.4.1 Classification of medicinal drugs and driving: Co-ordination and synthesis report. Due date of deliverable: 21.07.2011 Actual submission date: 21.07.2011 Revision date: 21.07.2011 Start date of project: 15.10.2006 Duration: 48 months Organisation name of lead contractor for this deliverable: UVA Revision 0.0 Project co-funded by the European Commission within the Sixth Framework Programme (2002-2006) Dissemination Level PU Public PP Restricted to other programme participants (including the Commission x Services) RE Restricted to a group specified by the consortium (including the Commission Services) CO Confidential, only for members of the consortium (including the Commission Services) DRUID 6th Framework Programme Deliverable D.4.4.1 Classification of medicinal drugs and driving: Co-ordination and synthesis report. Page 1 of 243 Classification of medicinal drugs and driving: Co-ordination and synthesis report. Authors Trinidad Gómez-Talegón, Inmaculada Fierro, M. Carmen Del Río, F. Javier Álvarez (UVa, University of Valladolid, Spain) Partners - Silvia Ravera, Susana Monteiro, Han de Gier (RUGPha, University of Groningen, the Netherlands) - Gertrude Van der Linden, Sara-Ann Legrand, Kristof Pil, Alain Verstraete (UGent, Ghent University, Belgium) - Michel Mallaret, Charles Mercier-Guyon, Isabelle Mercier-Guyon (UGren, University of Grenoble, Centre Regional de Pharmacovigilance, France) - Katerina Touliou (CERT-HIT, Centre for Research and Technology Hellas, Greece) - Michael Hei βing (BASt, Bundesanstalt für Straßenwesen, Germany). -

Reference List of Drugs with Potential Anticholinergic Effects 1, 2, 3, 4, 5
ANTICHOLINERGICS: Reference List of Drugs with Potential Anticholinergic Effects 1, 2, 3, 4, 5 J Bareham BSP © www.RxFiles.ca Aug 2021 WHENEVER POSSIBLE, AVOID DRUGS WITH MODERATE TO HIGH ANTICHOLINERGIC ACTIVITY IN OLDER ADULTS (>65 YEARS OF AGE) Low Anticholinergic Activity; Moderate/High Anticholinergic Activity -B in combo Beers Antibiotics Antiparkinsonian Cardiovascular Agents Immunosuppressants ampicillin *ALL AVAILABLE AS amantadine SYMMETREL atenolol TENORMIN azaTHIOprine IMURAN cefOXitin GENERIC benztropine mesylate COGENTIN captopril CAPOTEN cyclosporine NEORAL clindamycin bromocriptine PARLODEL chlorthalidone GENERIC ONLY hydrocortisone CORTEF gentamicin (Oint & Sol’n NIHB covered) carbidopa/levodopa SINEMET digoxin LANOXIN, TOLOXIN methylprednisolone MEDROL piperacillin entacapone COMTAN dilTIAZem CARDIZEM, TIAZAC prednisone WINPRED dipyridamole PERSANTINE, ethopropazine PARSITAN vancomycin phenelzine NARDIL AGGRENOX disopyramide RYTHMODAN Muscle Relaxants pramipexole MIRAPEX Antidepressants baclofen LIORESAL ( on intrathecal only) procyclidine KEMADRIN furosemide LASIX amitriptyline ELAVIL cyclobenzaprine FLEXERIL selegiline ELDEPRYL hydrALAZINE APRESOLINE clomiPRAMINE ANAFRANIL isosorbide ISORDIL methocarbamol ROBAXIN OTC trihexyphenidyl ARTANE desipramine NORPRAMIN metoprolol LOPRESOR orphenadrine NORFLEX OTC doxepin >6mg SINEQUAN Antipsychotics NIFEdipine ADALAT tiZANidine ZANAFLEX A imipramine TOFRANIL quiNIDine GENERIC ONLY C ARIPiprazole ABILIFY & MAINTENA -

Endocrine Drugs
PharmacologyPharmacologyPharmacology DrugsDrugs thatthat AffectAffect thethe EndocrineEndocrine SystemSystem TopicsTopicsTopics •• Pituitary Pituitary DrugsDrugs •• Parathyroid/Thyroid Parathyroid/Thyroid DrugsDrugs •• Adrenal Adrenal DrugsDrugs •• Pancreatic Pancreatic DrugsDrugs •• Reproductive Reproductive DrugsDrugs •• Sexual Sexual BehaviorBehavior DrugsDrugs FunctionsFunctionsFunctions •• Regulation Regulation •• Control Control GlandsGlandsGlands ExocrineExocrine EndocrineEndocrine •• Secrete Secrete enzymesenzymes •• Secrete Secrete hormoneshormones •• Close Close toto organsorgans •• Transport Transport viavia bloodstreambloodstream •• Require Require receptorsreceptors NervousNervous EndocrineEndocrine WiredWired WirelessWireless NeurotransmittersNeurotransmitters HormonesHormones ShortShort DistanceDistance LongLong Distance Distance ClosenessCloseness ReceptorReceptor Specificity Specificity RapidRapid OnsetOnset DelayedDelayed Onset Onset ShortShort DurationDuration ProlongedProlonged Duration Duration RapidRapid ResponseResponse RegulationRegulation MechanismMechanismMechanism ofofof ActionActionAction HypothalamusHypothalamusHypothalamus HypothalamicHypothalamicHypothalamic ControlControlControl PituitaryPituitaryPituitary PosteriorPosteriorPosterior PituitaryPituitaryPituitary Target Actions Oxytocin Uterus ↑ Contraction Mammary ↑ Milk let-down ADH Kidneys ↑ Water reabsorption AnteriorAnteriorAnterior PituitaryPituitaryPituitary Target Action GH Most tissue ↑ Growth TSH Thyroid ↑ TH secretion ACTH Adrenal ↑ Cortisol Cortex