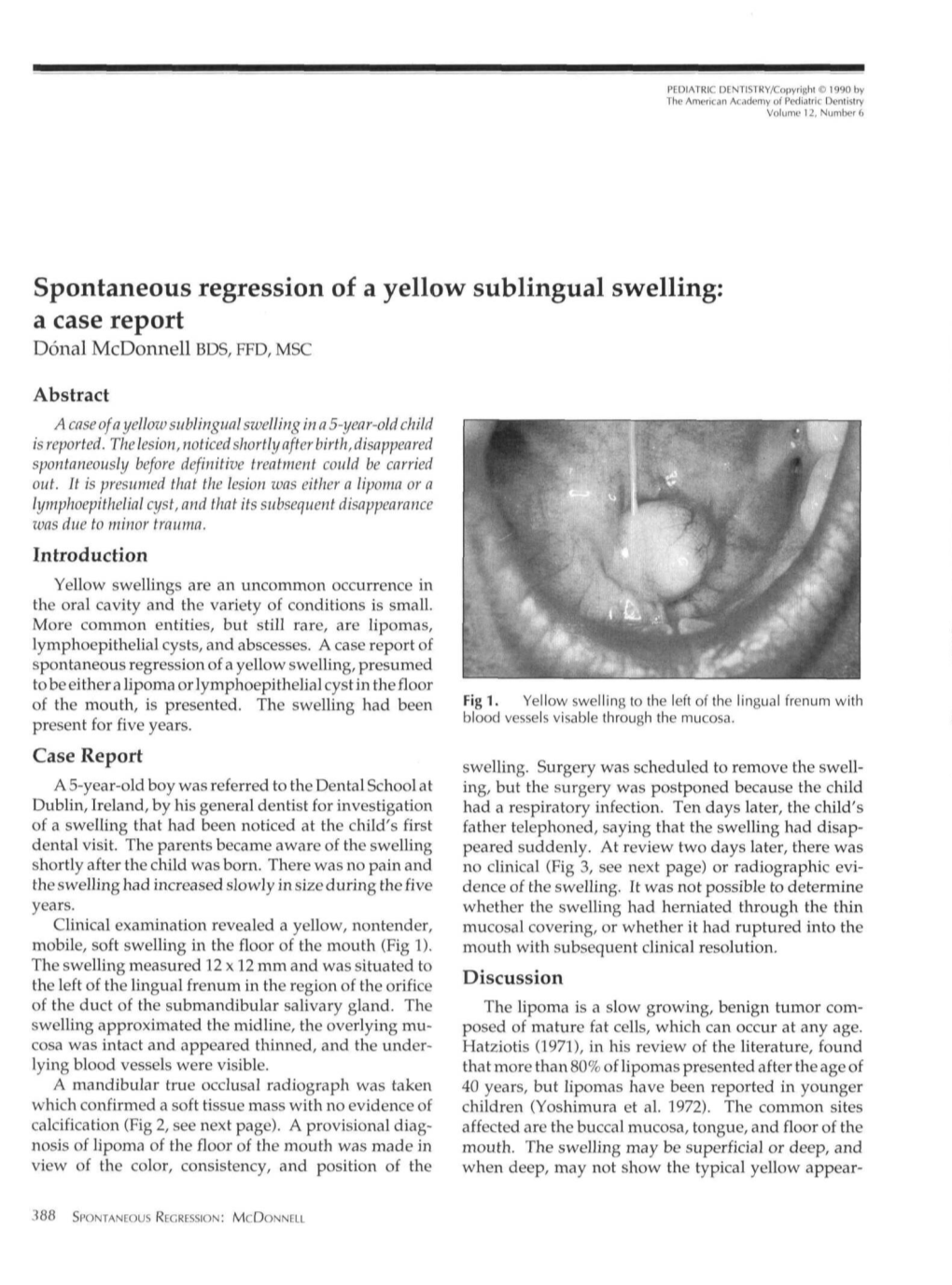
Spontaneous Regression of a Yellow Sublingual Swelling: a Case Report Donal Mcdonnell BDS, FFD, MSC
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pediatric Oral Pathology. Soft Tissue and Periodontal Conditions
PEDIATRIC ORAL HEALTH 0031-3955100 $15.00 + .OO PEDIATRIC ORAL PATHOLOGY Soft Tissue and Periodontal Conditions Jayne E. Delaney, DDS, MSD, and Martha Ann Keels, DDS, PhD Parents often are concerned with “lumps and bumps” that appear in the mouths of children. Pediatricians should be able to distinguish the normal clinical appearance of the intraoral tissues in children from gingivitis, periodontal abnormalities, and oral lesions. Recognizing early primary tooth mobility or early primary tooth loss is critical because these dental findings may be indicative of a severe underlying medical illness. Diagnostic criteria and .treatment recommendations are reviewed for many commonly encountered oral conditions. INTRAORAL SOFT-TISSUE ABNORMALITIES Congenital Lesions Ankyloglossia Ankyloglossia, or “tongue-tied,” is a common congenital condition characterized by an abnormally short lingual frenum and the inability to extend the tongue. The frenum may lengthen with growth to produce normal function. If the extent of the ankyloglossia is severe, speech may be affected, mandating speech therapy or surgical correction. If a child is able to extend his or her tongue sufficiently far to moisten the lower lip, then a frenectomy usually is not indicated (Fig. 1). From Private Practice, Waldorf, Maryland (JED); and Department of Pediatrics, Division of Pediatric Dentistry, Duke Children’s Hospital, Duke University Medical Center, Durham, North Carolina (MAK) ~~ ~ ~ ~ ~ ~ ~ PEDIATRIC CLINICS OF NORTH AMERICA VOLUME 47 * NUMBER 5 OCTOBER 2000 1125 1126 DELANEY & KEELS Figure 1. A, Short lingual frenum in a 4-year-old child. B, Child demonstrating the ability to lick his lower lip. Developmental Lesions Geographic Tongue Benign migratory glossitis, or geographic tongue, is a common finding during routine clinical examination of children. -

Salivary Glands
GASTROINTESTINAL SYSTEM [Anatomy and functions of salivary gland] 1 INTRODUCTION Digestive system is made up of gastrointestinal tract (GI tract) or alimentary canal and accessory organs, which help in the process of digestion and absorption. GI tract is a tubular structure extending from the mouth up to anus, with a length of about 30 feet. GI tract is formed by two types of organs: • Primary digestive organs. • Accessory digestive organs 2 Primary Digestive Organs: Primary digestive organs are the organs where actual digestion takes place. Primary digestive organs are: Mouth Pharynx Esophagus Stomach 3 Anatomy and functions of mouth: FUNCTIONAL ANATOMY OF MOUTH: Mouth is otherwise known as oral cavity or buccal cavity. It is formed by cheeks, lips and palate. It encloses the teeth, tongue and salivary glands. Mouth opens anteriorly to the exterior through lips and posteriorly through fauces into the pharynx. Digestive juice present in the mouth is saliva, which is secreted by the salivary glands. 4 ANATOMY OF MOUTH 5 FUNCTIONS OF MOUTH: Primary function of mouth is eating and it has few other important functions also. Functions of mouth include: Ingestion of food materials. Chewing the food and mixing it with saliva. Appreciation of taste of the food. Transfer of food (bolus) to the esophagus by swallowing . Role in speech . Social functions such as smiling and other expressions. 6 SALIVARY GLANDS: The saliva is secreted by three pairs of major (larger) salivary glands and some minor (small) salivary glands. Major glands are: 1. Parotid glands 2. Submaxillary or submandibular glands 3. Sublingual glands. 7 Parotid Glands: Parotid glands are the largest of all salivary glands, situated at the side of the face just below and in front of the ear. -

Appendix B: Muscles of the Speech Production Mechanism
Appendix B: Muscles of the Speech Production Mechanism I. MUSCLES OF RESPIRATION A. MUSCLES OF INHALATION (muscles that enlarge the thoracic cavity) 1. Diaphragm Attachments: The diaphragm originates in a number of places: the lower tip of the sternum; the first 3 or 4 lumbar vertebrae and the lower borders and inner surfaces of the cartilages of ribs 7 - 12. All fibers insert into a central tendon (aponeurosis of the diaphragm). Function: Contraction of the diaphragm draws the central tendon down and forward, which enlarges the thoracic cavity vertically. It can also elevate to some extent the lower ribs. The diaphragm separates the thoracic and the abdominal cavities. 2. External Intercostals Attachments: The external intercostals run from the lip on the lower border of each rib inferiorly and medially to the upper border of the rib immediately below. Function: These muscles may have several functions. They serve to strengthen the thoracic wall so that it doesn't bulge between the ribs. They provide a checking action to counteract relaxation pressure. Because of the direction of attachment of their fibers, the external intercostals can raise the thoracic cage for inhalation. 3. Pectoralis Major Attachments: This muscle attaches on the anterior surface of the medial half of the clavicle, the sternum and costal cartilages 1-6 or 7. All fibers come together and insert at the greater tubercle of the humerus. Function: Pectoralis major is primarily an abductor of the arm. It can, however, serve as a supplemental (or compensatory) muscle of inhalation, raising the rib cage and sternum. (In other words, breathing by raising and lowering the arms!) It is mentioned here chiefly because it is encountered in the dissection. -

DLA 1200 Dental Science I
ILLINOIS VALLEY COMMUNITY COLLEGE COURSE OUTLINE DIVISION: Workforce Development COURSE: DLA 1200 Dental Science I Date: Fall 2020 Credit Hours: 1 Prerequisite(s): Acceptance into the Dental Assisting Program Delivery Method: Lecture 1 Contact Hours (1 contact = 1 credit hour) Seminar 0 Contact Hours (1 contact = 1 credit hour) Lab 0 Contact Hours (2-3 contact = 1 credit hour) Clinical 0 Contact Hours (3 contact = 1 credit hour) Online Blended Offered: Fall Spring Summer CATALOG DESCRIPTION: This 8-week course will familiarize students with the foundations of anatomical terminology and the basic dental structures, nomenclature, structures of the oral cavity, information about the tooth and its surrounding structures, tooth identification systems, and an in-depth study of the different types of teeth, the description, surfaces, and additional details needed to identify the tooth inside or outside of the oral cavity. Students will study embryology and histology, occlusion, as well as form and function of the permanent and primary dentitions. Curriculum Committee – Course Outline Form Revised 12/5/2016 Page 1 of 10 GENERAL EDUCATION GOALS ADDRESSED [See last page for Course Competency/Assessment Methods Matrix.] Upon completion of the course, the student will be able: [Choose up to three goals that will be formally assessed in this course.] To apply analytical and problem solving skills to personal, social, and professional issues and situations. To communicate successfully, both orally and in writing, to a variety of audiences. To construct a critical awareness of and appreciation for diversity. To understand and use technology effectively and to understand its impact on the individual and society. -

Oropharyngeal Isthmus (Isthmus Faucium) – Soft Palate, Palatoglossal and Palatopharyngeal Arches, the Root of the Tongue
Oropharyngeal isthmus (isthmus faucium) – soft palate, palatoglossal and palatopharyngeal arches, the root of the tongue. Approximation of the arches, to shut off the mouth from the oropharynx, is essential to deglutition. Palatine tonsil (tonsilla palatina) sinus tonsillaris plica triangularis fossa supratonsillaris cryptae tonsillares tonsillitis – tonsillar pegs paratonsillar vein – venous hemorrage tonsillectomy Muscles of the tongue aponeurosis linguae, septum linguae, hypoglossal nerve (CN XII). Extrinsic muscles: M. genioglossus M. styloglossus M. palatoglossus M. hyoglossus – (canalis paralingualis contains the lingual artery ) Intrinsic muscles: Superior longitudinal muscle (m. longitudinalis superior) Inferior longitudinal musle (m. longitudinalis inferior) Transverse muscle (m. transversus ) Vertical muscle (m. verticalis Muscles of the soft palate M. tensor veli palatini - trigeminal nerve (IX., X.) M. levator veli palatini - plexus pharyngeus (IX., X.) Musculus uvulae - plexus pharyngeus (IX., X.) M. palatoglossus - plexus pharyngeus (IX., X.) M. palatopharyngeus plexus pharyngeus (IX., X.) Movements of the palate are essential to swallowing, blowing and speech; all requires variable degrees of closure of the nasopharynx. In deglutition closure prevents regurgitation into the nasopharynx. During closure levatores veli palatini pull the soft palate up and back towards the posterior pharyngeal wall while simultaneously the palatopharyngeal muscle raises the wall. PHARYNX fornix pharyngis pharyngeal recess cavum pharyngis fascia -

Chapter 1 Oral Structures and Tissues Arthur R
Chapter 1 Oral Structures and Tissues Arthur R. Hand1 and Marion E. Frank2 1 Department of Craniofacial Sciences and Cell Biology , School of Dental Medicine, University of Connecticut 2 Department of Oral Health and Diagnostic Sciences , University of Connecticut The oral cavity and its component cells, tissues, and structures the lips and the mucosa lining the inside of the lips, and extends constitute a unique and complex organ system and environment. posteriorly to the palatoglossal folds or arch . Beyond the palato- Of necessity, we study its various parts individually, but the glossal folds are the palatopharyngeal folds and the beginning health and function of the components of the oral cavity depend of the oropharynx , where the digestive and respiratory tracts upon and influence one another. Importantly, the oral cavity come together. The palatine tonsils are located in the tonsillar relies on as well as influences the health and function of the fauces between the palatoglossal and palatopharyngeal folds. entire body. The lymphoid tissue of the palatine tonsils, along with that of the The oral cavity is the gateway to the body, and most of the pharyngeal tonsil ( adenoids ) and the lingual tonsils , guards the substances that enter our bodies do so through the oral cavity. It entrance to the oropharynx. Anteriorly, the respiratory tract is exposed to the physical insults of mastication, hard objects and (nasal cavity) is separated from the oral cavity by the hard palate , various food substances, and extremes of temperature. A variety and posteriorly by the soft palate . The hard palate has an arch-like of chemicals, including those present in foods and drinks and shape that varies in width and height among individuals. -

The Palate and Faucial Isthmus
The palate and faucial isthmus He who guards his mouth and his tongue keeps himself from calamity. Proverbs 21:23 Ph.D., Dr. David Lendvai Parts of the oral cavity Parts of the oral cavity 1. Vestibule of the oral cavity Borders: - lips and cheek (bucca) - dental arches 2. Oral cavity proper Borders: - roof: hard and soft palate - floor: oral diaphragm (mylohoid m.) - antero-laterally: dental arches - posteriorly: isthmus of the fauces Etrance of the oral cavity - Philtrum - Upper & lower lip - Angulus - Rubor labii - Nasolabial groove (Facial palsy) Roof of the oral cavity: hard and soft palate Structures of the hard palate - incisive papilla - palatine rugae - palatine raphe - torus Hard and soft palate Muscles of the soft palate - Levator veli palatini m. - Tensor veli palatini m. - Palatoglossus m. - Palatopharyngeus m. - M. uvulae Muscles of the soft palate Muscles of the soft palate Structures of the hard and soft palate - mucous membrane - palatine glands - bone / muscles Histology of the hard palate Mucoperiosteum Histology of the soft palate NASAL SURFACE - pseudostratified ciliated columnar epithelium - lamina propria - mucous glands - striated muscle ORAL SURFACE - stratified squamous non keratinized epithelium Leukoplakia (precancerosal stage!!!) Allergic reaction Blood supply and innervation of the hard and soft palate - greater and lesser palatine nerves (maxillary nerve) greater and lesser palatine arteries - nasopalatine nerve ISTHMUS OF THE FAUCES Borders: superior: soft palate inferior: root of the tonque lateral: palatoglossal and palatopharngeal arch / fold Pharynx 3 levels: Nasopharynx Choana Oropharynx Isthmus faucium C6 Laryngopharynx Laryngeal inlet Oesophagus Waldeyer’s lymphatic ring • pharyngeal tonsil • tubarian tonsils • palatine tonsils • lingual tonsil Blood supply of palatine tonsil: - descending palatine artery (maxillary a.) - ascending palatine a. -

The Digestive System
The Digestive System We need food for cellular utilization: nutrients as building blocks for synthesis sugars, etc to break down for energy most food that we eat cannot be directly used by the body too large and complex to be absorbed chemical composition must be modified to be useable by cells Functions of Digestive System: 1. physical and chemical digestion 2. absorption 3. collect & eliminate nonuseable components Anatomy of Digestive System organs of digestive system form essentially: a long continuous tube open at both ends alimentary canal (gastrointestinal tract) mouthpharynxesophagusstomachsmall intestinelarge intestine attached to this tube are assorted accessory organs and structures that aid in the digestive processes salivary glands teeth liver gall bladder pancreas mesenteries The GI tract (digestive system) is located mainly in abdominopelvic cavity surrounded by serous membrane = visceral peritoneum this serous membrane is continuous with parietal peritoneum and extends between digestive organs as mesenteries hold organs in place, prevent tangling Intro to A & P: Digestive Anatomy; Ziser Lecture Notes, 2005 1 The wall of the alimentary canal consists of 4 layers: outer serosa: visceral peritoneum, mainly fibrous and areolar CT muscularis several layers of smooth muscle submucosa blood vessels, lymphatic vessels, nerves, connective tissue inner mucosa: mucous membrane lining these layers are modified within various organs some have muscle layers well developed some with mucous lining modified for secretion of digestive -

Pleomorphic Adenoma of the Cheek. Case Report with Review
Int. J. Odontostomat., 14(4):653-657, 2020. Pleomorphic Adenoma of the Cheek. Case Report with Review Adenoma Pleomórfico de Mejilla. Reporte de Caso con Revisión Soukayna Bahbah & Saliha Chbicheb BAHBAH, S. & CHBICHEB, S. Pleomorphic adenoma of the cheek. Case report with review. Int. J. Odontostomat., 14(4):653- 657, 2020. ABSTRACT: Pleomorphic adenoma (PA), also called benign mixed tumor, is the most common tumor of the salivary glands. About 70 % of these tumors occur in the parotid gland and an uncommon site are the minor salivary glands. The most common sites of PA of the minor salivary glands are the palate followed by lips and cheek. Other rare reported sites include the fauces, floor of the mouth, tongue, tonsil, pharynx, retromolar area and nasal cavity. Here we report a case of pleomorphic adenoma of minor salivary glands of the cheek in a 22-year-old male. The mass was removed by wide local excision with adequate margins, and the patient was followed for 1-year post operatively with no recurrence. KEY WORDS: pleomorphic adenoma, minor salivary gland, cheek. INTRODUCTION Pleomorphic adenomas are benign salivary They are more common in adult females from gland tumors that represent about 3-10 % of the the 3rd to 5th decades (Aro et al.). neoplasm of the head and neck region. They are the most common tumors (50 %) of the major and minor PA presents as a mobile slowly growing, painless salivary glands. The palate is considered as the most firm swelling that does not cause ulceration of the common intraoral site (42.8-68.8 %), followed by the overlying mucosa (Garcia Berrocal et al., 2000). -

Calculous Sialadenitis: Clinic, Diagnostics, Medical Treatment
MINISTRY OF HEALTH OF UKRAINE Ukrainian medical stomatological academy “Approved” On the meeting chair Of Propaedeutics Surgical Stomatology The Head of the Department prof. Novikov V.M. ___________ “ ____ ” _____________ 20 ____ GUIDELINES Individual work of students During preparation for Practical classes Educational discipline Surgical stomatology Module № 2 Inflammatory diseases in maxillofacial region. Nonodontogenous inflammatory diseases in Content module № 4 maxillofacial region Calculous sialadenitis: clinic, diagnostics, medical treatment. Fistuls of salivary glands, mechanism of their formation. Examination methods, diagnostics, methods of surgical medical treatment (C.P.Sapozhcov, A.N.Limbexg, G.A.Vasilev and Theme lesson in.). Contribution of chairs of surgical stomatology Ukrainian medicine stomatology academy to working out of questions of an etiology, a pathogenesis and treatment of diseases of salivary glands. Course 3 Faculty Stomatological Poltava 2018 1. Actuality of the topic: On statistical given to N.D. Lesovoj (1979) sialolithiasis compounds 40-61,1 % among all diseases of sialadens. Sialolithiasis - polyetiological disease of sialadens, therefore is a lot of questions of an etiology, a pathogeny, clinic and treatments of this pathology remain thoroughly not investigated to this time (to I.F. Romacheva and joint authors, 1987). 2. The objectives of the studies: To learn students to diagnose and define medical tactics at manifestations a calculus sialadenitis (sialolithiasis). To be able: To make a diagnosis of a calculus sialadenitis (sialolithiasis; To draw up a plan of examination of the patient with a calculus sialadenitis (sialolithiasis); To prescribe proper treatment of a calculus sialadenitis (sialolithiasis). 3. Basic knowledge, skills, skills necessary for study topics (interdisciplinary integration). Name of previous These skills courses Physiopathology Inflammatory processes Anatomical pathology Inflammatory processes Microbiology The infestant, microbic flora of an oral cavity and a secret of sialadens. -

A Case Against the Use of the Throat Culture in the Management of Streptoccocal Pharyngitis
A Case Against the Use of the Throat Culture in the Management of Streptoccocal Pharyngitis Clive Caplan, MB Islip Terrace, New York Acute pharyngitis is a common problem for the clinician and yet a difficult one. The throat culture appears to offer defini tive diagnostic information, but this is illusory. The culture is inconvenient, subject to too many false negative and false positive results, and does not denote active streptococcal in fection. Clinical assessment of the acute pharyngitis patient is shown to be the better approach. Streptoccocal pharyngitis cannot be diagnosed pharyngitis due to this organism is still extremely by clinical methods—there must be a throat cul difficult. ture. It is suggested here that the throat culture has So speaks current wisdom in medicine, es too many problems associated with its use and in poused by teachers and repeated in textbooks, and terpretation, that it is of little value in supplying so transmitted to generations of students and concrete bacteriological diagnosis, and that clini practitioners. The evidence of the clinician’s own cal decision making in acute pharyngitis, without a senses must defer to an impersonal laboratory re throat culture, is both rational and acceptable. port, and the diagnosis of pharyngitis becomes an exercise in divination of a blood agar plate. Although one hundred years have now passed since the discovery of streptococcus pyogenes by Louis Pasteur, in the blood of a patient with puer The Misleadingly Negative Throat Culture peral septicemia,1 the definitive identification of In streptococcal pharyngitis the throat culture may be negative for the streptococcus since re covery rates for the organism are never 100 per cent and are often very much less. -

Oral Cavity and Glands
Dr. Randall E. Merchant [email protected] THE ORAL CAVITY AND GLANDS Objectives 1. Define the limits of the oral cavity and understand the varying features of the oral mucosa. 2. Compare and contrast the structure of the four types of papillae over the dorsum of the tongue. 3. Describe the basic structure of a taste bud. 4. Define the major subdivisions of a tooth. 5. With the microscope, identify the three types of major salivary glands and the morphologic features that distinguish them from each other. Recognize and know the function of other structures in BOLD in the laboratory guide. 6. Describe the function of striated ducts and how they affect the consistency of the saliva. 7. Identify the structures on the CD listed in the laboratory guide. I. General Features of Oral Cavity A. Definitions 1. Vestibule - internal to the lips and cheeks, as far back as the teeth 2. Oral Cavity Proper - behind the teeth (forward and lateral), bounded above by the hard and soft palate, the tongue below, ends posteriorly at the fauces (beginning of the oropharynx) B. Masticatory Mucosa - present on gingiva, dorsum of tongue, and hard palate 1. Stratified squamous keratinized (parakeratinized) epithelium 2. Underlying connective tissue contains Meissner's corpuscles & minor salivary glands (mostly mucus-secreting) Lingual Minor Salivary Glands Submandibular Duct Frenulum of Tongue Sublingual Gland O penings of Sublingual Ducts Opening of Submandibular Duct C. Lining Mucosa - found everywhere else except gingiva, dorsum of tongue, and hard palate 1. Stratified squamous nonkeratinized epithelium 2. Underlying connective tissue contains Meissner's corpuscles & minor salivary glands (mostly mucus-secreting and classified morphologically as compound tubuloacinar) II.