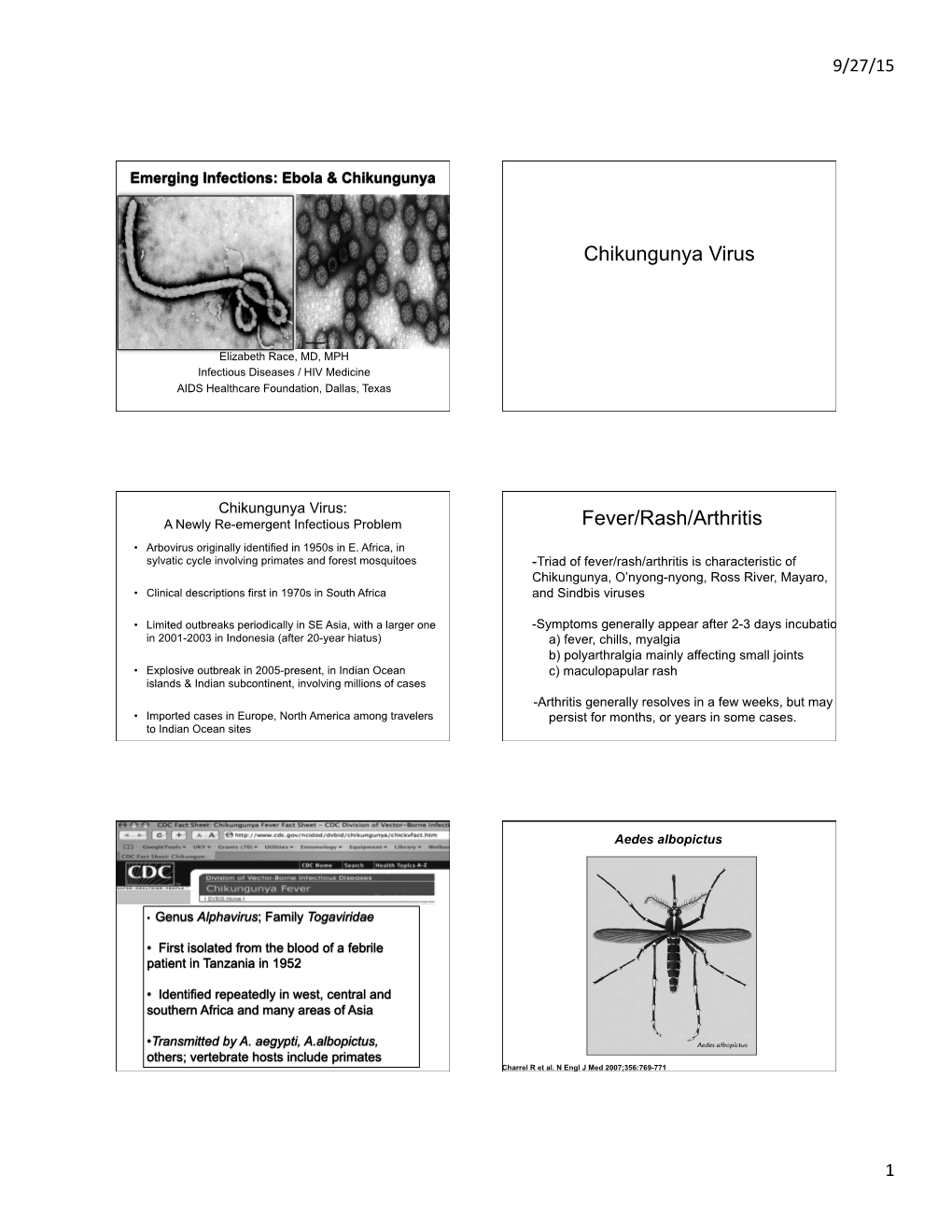
Chikungunya Virus Fever/Rash/Arthritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses
ARIZONA ARBOVIRAL HANDBOOK FOR CHIKUNGUNYA, DENGUE, AND ZIKA VIRUSES 7/31/2017 Arizona Department of Health Services | P a g e 1 Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses OBJECTIVES .............................................................................................................. 4 I: CHIKUNGUNYA ..................................................................................................... 5 Chikungunya Ecology and Transmission ....................................... 6 Chikungunya Clinical Disease and Case Management ............... 7 Chikungunya Laboratory Testing .................................................. 8 Chikungunya Case Definitions ...................................................... 9 Chikungunya Case Classification Algorithm ............................... 11 II: DENGUE .............................................................................................................. 12 Dengue Ecology and Transmission .............................................. 14 Dengue Clinical Disease and Case Management ...................... 14 Dengue Laboratory Testing ......................................................... 17 Dengue Case Definitions ............................................................ 19 Dengue Case Classification Algorithm ....................................... 23 III: ZIKA .................................................................................................................. -

Ebola Virus Disease
Outbreaks Chronology: Ebola Virus Disease Known Cases and Outbreaks of Ebola Virus Disease, in Reverse Chronological Order: Reported number (%) of Reported deaths Ebola number of among Year(s) Country subtype human cases cases Situation August- Democratic Ebola virus 66 49 (74%) Outbreak occurred in November 2014 Republic of multiple villages in the Congo the Democratic Republic of the Congo. The outbreak was unrelated to the outbreak of Ebola in West Africa. March 2014- Multiple Ebola virus 28652 11325 Outbreak across Present countries multiple countries in West Africa. Number of patients is constantly evolving due to the ongoing investigation. 32 November 2012- Uganda Sudan virus 6* 3* (50%) Outbreak occurred in January 2013 the Luwero District. CDC assisted the Ministry of Health in the epidemiologic and diagnostic aspects of the outbreak. Testing of samples by CDC's Viral Special Pathogens Branch occurred at UVRI in Entebbe. 31 June-November Democratic Bundibugyo 36* 13* (36.1%) Outbreak occurred in 2012 Republic of virus DRC’s Province the Congo Orientale. Laboratory support was provided through CDC and the Public Health Agency of Canada (PHAC)’s field laboratory in Isiro, as well as through the CDC/UVRI lab in Uganda. The outbreak in DRC had no epidemiologic link to the near contemporaneous Ebola outbreak in the Kibaale district of Uganda. 31 June-October Uganda Sudan virus 11* 4* (36.4%) Outbreak occurred in 2012 the Kibaale District of Uganda. Laboratory tests of blood samples were conducted by the UVRI and the CDC. 31 May 2011 Uganda Sudan virus 1 1 (100%) The Uganda Ministry of Health informed the public a patient with suspected Ebola Hemorrhagic fever died on May 6, 2011 in the Luwero district, Uganda. -

1.1.1.2 Tick-Borne Encephalitis Virus
This thesis has been submitted in fulfilment of the requirements for a postgraduate degree (e.g. PhD, MPhil, DClinPsychol) at the University of Edinburgh. Please note the following terms and conditions of use: • This work is protected by copyright and other intellectual property rights, which are retained by the thesis author, unless otherwise stated. • A copy can be downloaded for personal non-commercial research or study, without prior permission or charge. • This thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the author. • The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author. • When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given. Transcriptomic and proteomic analysis of arbovirus-infected tick cells Sabine Weisheit Thesis submitted for the degree of Doctor of Philosophy The Roslin Institute and Royal (Dick) School of Veterinary Studies, University of Edinburgh 2014 Declaration .................................................................................................... i Acknowledgements ..................................................................................... ii Abstract of Thesis ....................................................................................... iii List of Figures .............................................................................................. v List -

Chikungunya Fever: Epidemiology, Clinical Syndrome, Pathogenesis
Antiviral Research 99 (2013) 345–370 Contents lists available at SciVerse ScienceDirect Antiviral Research journal homepage: www.elsevier.com/locate/antiviral Review Chikungunya fever: Epidemiology, clinical syndrome, pathogenesis and therapy ⇑ Simon-Djamel Thiberville a,b, , Nanikaly Moyen a,b, Laurence Dupuis-Maguiraga c,d, Antoine Nougairede a,b, Ernest A. Gould a,b, Pierre Roques c,d, Xavier de Lamballerie a,b a UMR_D 190 ‘‘Emergence des Pathologies Virales’’ (Aix-Marseille Univ. IRD French Institute of Research for Development EHESP French School of Public Health), Marseille, France b University Hospital Institute for Infectious Disease and Tropical Medicine, Marseille, France c CEA, Division of Immuno-Virologie, Institute of Emerging Diseases and Innovative Therapies, Fontenay-aux-Roses, France d UMR E1, University Paris Sud 11, Orsay, France article info abstract Article history: Chikungunya virus (CHIKV) is the aetiological agent of the mosquito-borne disease chikungunya fever, a Received 7 April 2013 debilitating arthritic disease that, during the past 7 years, has caused immeasurable morbidity and some Revised 21 May 2013 mortality in humans, including newborn babies, following its emergence and dispersal out of Africa to the Accepted 18 June 2013 Indian Ocean islands and Asia. Since the first reports of its existence in Africa in the 1950s, more than Available online 28 June 2013 1500 scientific publications on the different aspects of the disease and its causative agent have been pro- duced. Analysis of these publications shows that, following a number of studies in the 1960s and 1970s, Keywords: and in the absence of autochthonous cases in developed countries, the interest of the scientific commu- Chikungunya virus nity remained low. -

2020 Taxonomic Update for Phylum Negarnaviricota (Riboviria: Orthornavirae), Including the Large Orders Bunyavirales and Mononegavirales
Archives of Virology https://doi.org/10.1007/s00705-020-04731-2 VIROLOGY DIVISION NEWS 2020 taxonomic update for phylum Negarnaviricota (Riboviria: Orthornavirae), including the large orders Bunyavirales and Mononegavirales Jens H. Kuhn1 · Scott Adkins2 · Daniela Alioto3 · Sergey V. Alkhovsky4 · Gaya K. Amarasinghe5 · Simon J. Anthony6,7 · Tatjana Avšič‑Županc8 · María A. Ayllón9,10 · Justin Bahl11 · Anne Balkema‑Buschmann12 · Matthew J. Ballinger13 · Tomáš Bartonička14 · Christopher Basler15 · Sina Bavari16 · Martin Beer17 · Dennis A. Bente18 · Éric Bergeron19 · Brian H. Bird20 · Carol Blair21 · Kim R. Blasdell22 · Steven B. Bradfute23 · Rachel Breyta24 · Thomas Briese25 · Paul A. Brown26 · Ursula J. Buchholz27 · Michael J. Buchmeier28 · Alexander Bukreyev18,29 · Felicity Burt30 · Nihal Buzkan31 · Charles H. Calisher32 · Mengji Cao33,34 · Inmaculada Casas35 · John Chamberlain36 · Kartik Chandran37 · Rémi N. Charrel38 · Biao Chen39 · Michela Chiumenti40 · Il‑Ryong Choi41 · J. Christopher S. Clegg42 · Ian Crozier43 · John V. da Graça44 · Elena Dal Bó45 · Alberto M. R. Dávila46 · Juan Carlos de la Torre47 · Xavier de Lamballerie38 · Rik L. de Swart48 · Patrick L. Di Bello49 · Nicholas Di Paola50 · Francesco Di Serio40 · Ralf G. Dietzgen51 · Michele Digiaro52 · Valerian V. Dolja53 · Olga Dolnik54 · Michael A. Drebot55 · Jan Felix Drexler56 · Ralf Dürrwald57 · Lucie Dufkova58 · William G. Dundon59 · W. Paul Duprex60 · John M. Dye50 · Andrew J. Easton61 · Hideki Ebihara62 · Toufc Elbeaino63 · Koray Ergünay64 · Jorlan Fernandes195 · Anthony R. Fooks65 · Pierre B. H. Formenty66 · Leonie F. Forth17 · Ron A. M. Fouchier48 · Juliana Freitas‑Astúa67 · Selma Gago‑Zachert68,69 · George Fú Gāo70 · María Laura García71 · Adolfo García‑Sastre72 · Aura R. Garrison50 · Aiah Gbakima73 · Tracey Goldstein74 · Jean‑Paul J. Gonzalez75,76 · Anthony Grifths77 · Martin H. Groschup12 · Stephan Günther78 · Alexandro Guterres195 · Roy A. -

Replication of Marburg Virus in Human Endothelial Cells a Possible Mechanism for the Development of Viral Hemorrhagic Disease
Replication of Marburg Virus in Human Endothelial Cells A Possible Mechanism for the Development of Viral Hemorrhagic Disease Hans-Joachim Schnittler,$ Friederike Mahner, * Detlev Drenckhahn, * Hans-Dieter Klenk, * and Heinz Feldmann * *Institut fir Virologie, Philipps-Universitdt Marburg, 3550 Marburg, Germany; tInstitutftirAnatomie, Universitdt Wiirzburg, 8700 Wiirzburg, Germany Abstract Rhabdoviridae, within the new proposed order Mononegavi- Marburg and Ebola virus, members of the family Filoviridae, rales (10). Virions are composed of a helical nucleocapsid cause a severe hemorrhagic disease in humans and primates. surrounded by a lipid envelope. The genome is nonsegmented, The disease is characterized as a pantropic virus infection often of negative sense, and 19 kb in length (3, 11, 12). Virion parti- resulting in a fulminating shock associated with hemorrhage, cles contain at least seven structural proteins (8, 13-16). and death. All known histological and pathophysiological pa- Filovirus infections have several pathological features in rameters of the disease are not sufficient to explain the devas- common with other severe viral hemorrhagic fevers such as tating symptoms. Previous studies suggested a nonspecific de- Lassa fever, hemorrhagic fever with renal syndrome, and struction of the endothelium as a possible mechanism. Con- Dengue hemorrhagic fever (5). Among these viruses, filovi- cerning the important regulatory functions of the endothelium ruses cause the highest case-fatality rates ( - 35% for MBG [61 (blood pressure, antithrombogenicity, homeostasis), we exam- and up to 90% for EBO, subtype Zaire [17]) and the most ined Marburg virus replication in primary cultures of human severe hemorrhagic manifestations. The pathophysiologic endothelial cells and organ cultures of human umbilical cord events that make filovirus infections of humans so devastating veins. -

Marburg Hemorrhagic Fever Fact Sheet
Marburg Hemorrhagic Fever Fact Sheet What is Marburg hemorrhagic fever? Marburg hemorrhagic fever is a rare, severe type of hemorrhagic fever which affects both humans and non-human primates. Caused by a genetically unique zoonotic (that is, animal-borne) RNA virus of the filovirus family, its recognition led to the creation of this virus family. The four species of Ebola virus are the only other known members of the filovirus family. Marburg virus was first recognized in 1967, when outbreaks of hemorrhagic fever occurred simultaneously in laboratories in Marburg and Frankfurt, Germany and in Belgrade, Yugoslavia (now Serbia). A total of 37 people became ill; they included laboratory workers as well as several medical personnel and Negative stain image of an isolate of Marburg virus, family members who had cared for them. The first people showing filamentous particles as well as the infected had been exposed to African green monkeys or characteristic "Shepherd's Crook." Magnification their tissues. In Marburg, the monkeys had been imported approximately 100,000 times. Image courtesy of for research and to prepare polio vaccine. Russell Regnery, Ph.D., DVRD, NCID, CDC. Where do cases of Marburg hemorrhagic fever occur? Recorded cases of the disease are rare, and have appeared in only a few locations. While the 1967 outbreak occurred in Europe, the disease agent had arrived with imported monkeys from Uganda. No other case was recorded until 1975, when a traveler most likely exposed in Zimbabwe became ill in Johannesburg, South Africa – and passed the virus to his traveling companion and a nurse. 1980 saw two other cases, one in Western Kenya not far from the Ugandan source of the monkeys implicated in the 1967 outbreak. -

Comparison and Evaluation of Real-Time Taqman PCR for Detection and Quantification of Ebolavirus
viruses Article Comparison and Evaluation of Real-Time Taqman PCR for Detection and Quantification of Ebolavirus Yi Huang 1,* , Shuqi Xiao 2 and Zhiming Yuan 1,* 1 National Biosafety Laboratory, Chinese Academy of Sciences, Wuhan 430020, China 2 Wuhan Institute of Virology, Chinese Academy of Sciences, Wuhan 430020, China; [email protected] * Correspondence: [email protected] (Y.H.); [email protected] (Z.Y.) Abstract: Given that ebolavirus causes severe and frequently lethal disease, its rapid and accurate detection using available and validated methods is essential for controlling infection. Real-time reverse-transcription PCR (RT-PCR) has proven to be an invaluable tool for ebolaviruses diagnostics. Many assays with different targets have been developed, but they have not been externally compared or validated, and limits of detection are not uniformly reported. Here we compared and evaluated the sensitivity, reproducibility and specificity of 23 in-house assays under the same conditions. Our results showed that these assays were highly gene- and species- specific when evaluated using in vitro RNA transcripts and viral RNA, and the potential limits of detection were uniformly reported 2 6 ranging from 10 to 10 in vitro synthesized RNA transcripts copies perµL and 1–100 TCID50/mL. The comparison of these assays indicated that those targeting the more conservative NP gene could be the better option for EVD case definition and quantitative measurement because of its higher sensitivity for the same species. Our analysis could contribute to the standardization of ebolavirus detection and quantification assays, which can offer a better understanding of the meaning of results across laboratories and time points, as well as make them easy to implement, especially under outbreak conditions. -

Antibody-Mediated Enhancement Aggravates Chikungunya Virus
www.nature.com/scientificreports OPEN Antibody-mediated enhancement aggravates chikungunya virus infection and disease severity Received: 14 July 2017 Fok-Moon Lum 1,2, Thérèse Couderc3,4, Bing-Shao Chia1,8, Ruo-Yan Ong1,9, Zhisheng Her1,10, Accepted: 17 January 2018 Angela Chow5, Yee-Sin Leo5, Yiu-Wing Kam1, Laurent Rénia1, Marc Lecuit 3,4,6 & Published: xx xx xxxx Lisa F. P. Ng1,2,7 The arthropod-transmitted chikungunya virus (CHIKV) causes a fu-like disease that is characterized by incapacitating arthralgia. The re-emergence of CHIKV and the continual risk of new epidemics have reignited research in CHIKV pathogenesis. Virus-specifc antibodies have been shown to control virus clearance, but antibodies present at sub-neutralizing concentrations can also augment virus infection that exacerbates disease severity. To explore this occurrence, CHIKV infection was investigated in the presence of CHIKV-specifc antibodies in both primary human cells and a murine macrophage cell line, RAW264.7. Enhanced attachment of CHIKV to the primary human monocytes and B cells was observed while increased viral replication was detected in RAW264.7 cells. Blocking of specifc Fc receptors (FcγRs) led to the abrogation of these observations. Furthermore, experimental infection in adult mice showed that animals had higher viral RNA loads and endured more severe joint infammation in the presence of sub-neutralizing concentrations of CHIKV-specifc antibodies. In addition, CHIKV infection in 11 days old mice under enhancing condition resulted in higher muscles viral RNA load detected and death. These observations provide the frst evidence of antibody-mediated enhancement in CHIKV infection and pathogenesis and could also be relevant for other important arboviruses such as Zika virus. -

MARBURG HEMORRHAGIC FEVER (Marburg HF)
MARBURG HEMORRHAGIC FEVER (Marburg HF) REPORTING INFORMATION • Class A: Report immediately via telephone the case or suspected case and/or a positive laboratory result to the local public health department where the patient resides. If patient residence is unknown, report immediately via telephone to the local public health department in which the reporting health care provider or laboratory is located. Local health departments should report immediately via telephone the case or suspected case and/or a positive laboratory result to the Ohio Department of Health (ODH). • Reporting Form(s) and/or Mechanism: o Immediately via telephone. o For local health departments, cases should also be entered into the Ohio Disease Reporting System (ODRS) within 24 hours of the initial telephone report to the ODH. • Key fields for ODRS reporting include: import status (whether the infection was travel-associated or Ohio-acquired), date of illness onset, and all the fields in the Epidemiology module. AGENT Marburg hemorrhagic fever is a rare, severe type of hemorrhagic fever which affects both humans and non-human primates. Caused by a genetically unique zoonotic RNA virus of the family Filoviridae, its recognition led to the creation of this virus family. The five species of Ebola virus are the only other known members of the family Filoviridae. Marburg virus was first recognized in 1967, when outbreaks of hemorrhagic fever occurred simultaneously in laboratories in Marburg and Frankfurt, Germany and in Belgrade, Yugoslavia (now Serbia). A total of 31 people became ill, including laboratory workers as well as several medical personnel and family members who had cared for them. -

Presentation
COMPLETE HEMORRHAGIC FEVER VIRUS INACTIVATION DURING LYSIS IN THE FILMARRAY BIOTHREAT-E ASSAY DEMONSTRATES THE BIOSAFETY OF THIS TEST. Olivier Ferraris (3), Françoise Gay-Andrieu (1), Marie Moroso (2), Fanny Jarjaval (3), Mark Miller (1), Christophe N. Peyrefitte (3) (1) bioMérieux, Marcy l’Etoile, France, (2) Fondation Mérieux, France (3) Unité de Virologie, Institut de recherche biomédicale des armées, Brétigny sur Orge, France Background : Viral hemorrhagic fevers (VHFs) are a group of illnesses caused by mainly five families of viruses namely Arenaviridae, Filoviridae , Bunyaviridae (Orthonairovirus genus ), Flaviviruses and Paramyxovirus (Henipavirus genus). The filovirus species known to cause disease in humans, Ebola virus (Zaire Ebolavirus), Sudan virus (Sudan Ebolavirus), Tai Forest virus (Tai Forest Ebolavirus), Bundibugyo virus (Bundibugyo Ebolavirus), and Marburg virus are restricted to Central Africa for 35 years, and spread to Guinea, Liberia, Sierra Leone in early 2014. Lassa fever is responsible for disease outbreaks across West Africa and in Southern Africa in 2008, with the identification of novel world arenavirus (Lujo virus). Henipavirus spread South Asia to Australia. CCHFv spread asia to south europa. They are transmitted from host reservoir by direct contacts or through vectors such as ticks bits. Working with VHF viruses, need a Biosafety Level 4 (BSL-4) laboratory, however during epidemics such observed with Ebola virus in 2014, the need to diagnose rapidly the patients raised the necessity to develop local laboratories These viruses represents a threat to healthcare workers and researches who manage infected diagnostic samples in laboratories. Aim : 1 Inactivation step An FilmArray Bio Thereat-E assay for detection of Hemorrhagic fever viruse Interfering substance HF virus + FA Lysis Buffer such as Ebola virus was developed to respond to Hemorrhagic fever virus 106 Ebola virus Whole blood + outbreak. -

Dengue Fever/Severe Dengue Fever/Chikungunya Fever! Report on Suspicion of Infection During Business Hours
Dengue Fever/Severe Dengue Fever/Chikungunya Fever! Report on suspicion of infection during business hours PROTOCOL CHECKLIST Enter available information into Merlin upon receipt of initial report Review background information on the disease (see Section 2), case definitions (see Section 3 for dengue and for chikungunya), and laboratory testing (see Section 4) Forward specimens to the Florida Department of Health (DOH) Bureau of Public Health Laboratories (BPHL) for confirmatory laboratory testing (as needed) Inform local mosquito control personnel of suspected chikungunya or dengue case as soon as possible (if applicable) Inform state Arbovirus Surveillance Coordinator on suspicion of locally acquired arbovirus infection Contact provider (see Section 5A) Interview case-patient Review disease facts (see Section 2) Mode of transmission Ask about exposure to relevant risk factors (see Section 5. Case Investigation) History of travel, outdoor activities, and mosquito bites two weeks prior to onset History of febrile illness or travel for household members or other close contacts in the month prior to onset History of previous arbovirus infection or vaccination (yellow fever, Japanese encephalitis) Provide education on transmission and prevention (see Section 6) Awareness of mosquito-borne diseases Drain standing water at least weekly to stop mosquitoes from multiplying Discard items that collect water and are not being used Cover skin with clothing or Environmental Protection Agency (EPA)-registered repellent such as DEET (N,N-diethyl-meta-toluamide) Use permethrin on clothing (not skin) according to manufacturer’s directions Cover doors and windows with intact screens to keep mosquitoes out of the house Enter additional data obtained from interview into Merlin (see Section 5D) Arrange for a convalescent specimen to be taken (if necessary) Dengue/Chikungunya Guide to Surveillance and Investigation Dengue Fever/Severe Dengue/Chikungunya 1.