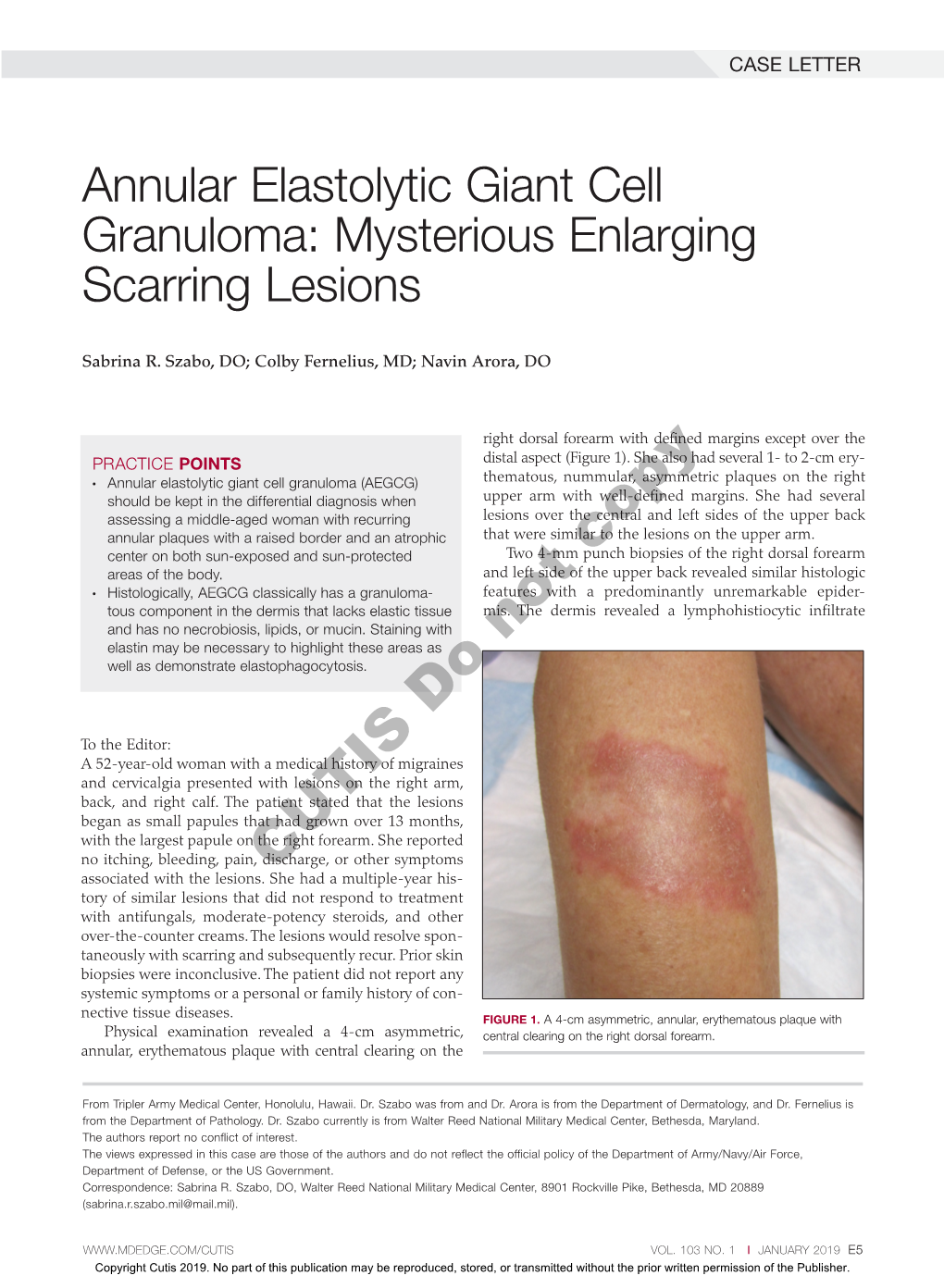
Annular Elastolytic Giant Cell Granuloma: Mysterious Enlarging Scarring Lesions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clinicopathological Features of Annular Elastolytic Giant Cell
Original Investigation / Özgün Araştırma Turk J Dermatol 2018;12:85-9 • DOI: 10.4274/tdd.3409 85 Hilal Kaya Clinicopathological Features of Annular Erdoğan, Deniz Arık*, Elastolytic Giant Cell Granuloma Patients Ersoy Acer, Evrim Yılmaz*, Anüler Elastolitik Dev Hücreli Granülom Zeynep Nurhan Hastalarının Klinikopatolojik Özellikleri Saraçoğlu Abstract Objective: Annular elastolytic giant cell granuloma (AEGCG) is a rare granulomatous disease characterized by annular plaques. In this study, we aimed to describe the clinical and pathological features of the patients diagnosed with AEGCG. Methods: The demographic, clinical and pathological features of patients who diagnosed with AEGCG were recorded retrospectively. Results: Ten patients with AEGCG included in the study (nine females and one male). The mean age of the patients was 60±9.53 years. The mean duration of disease was 24.2±36.30 months. On dermatologic examination, multiple, well-demarcated, elevated borders and central atrophic erythematous annular plaques were seen in all patients. In the most of the patients (90%) lesions were on the sun-exposed regions. Six of the patients had accompanying diseases. Histopathologic examination of the punch biopsies revealed foreign body type multinucleated giant cells and lymphocytic cell infiltration in the dermis. There were intracellular elastic fiber fragments as sign of elastophagocytosis in the giant cells. Conclusion: AEGCG is a rare granulomatous disease which can accompany various diseases. There is debate on the terminology, classification and pathogenesis. Further studies are required to elucidate the unknowns. Keywords: Annular elastolytic giant cell granuloma, elastophagocytosis, granulomatous diseases, elastolysis, giant cell, granuloma annulare Eskişehir Osmangazi University Faculty of Medicine, Öz Department of Dermatology and Venereology, Amaç: Anüler elastolitik dev hücreli granülom (AEDHG), anüler plaklar ile karakterize, Eskişehir, Turkey nadir granülomatöz bir hastalıktır. -

Granuloma Annulare: Not As Simple As It Seems
Thomas Jefferson University Jefferson Digital Commons Department of Dermatology and Cutaneous Department of Dermatology and Cutaneous Biology Faculty Papers Biology 9-1-2010 Granuloma annulare: not as simple as it seems. Lawrence Charles Parish Thomas Jefferson University Joseph A. Witkowski University of Pennsylvania School of Medicine Follow this and additional works at: https://jdc.jefferson.edu/dcbfp Part of the Dermatology Commons Let us know how access to this document benefits ouy Recommended Citation Parish, Lawrence Charles and Witkowski, Joseph A., "Granuloma annulare: not as simple as it seems." (2010). Department of Dermatology and Cutaneous Biology Faculty Papers. Paper 76. https://jdc.jefferson.edu/dcbfp/76 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in Department of Dermatology and Cutaneous Biology Faculty Papers by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Granuloma Annulare: Not as simple as -

Table I. Genodermatoses with Known Gene Defects 92 Pulkkinen
92 Pulkkinen, Ringpfeil, and Uitto JAM ACAD DERMATOL JULY 2002 Table I. Genodermatoses with known gene defects Reference Disease Mutated gene* Affected protein/function No.† Epidermal fragility disorders DEB COL7A1 Type VII collagen 6 Junctional EB LAMA3, LAMB3, ␣3, 3, and ␥2 chains of laminin 5, 6 LAMC2, COL17A1 type XVII collagen EB with pyloric atresia ITGA6, ITGB4 ␣64 Integrin 6 EB with muscular dystrophy PLEC1 Plectin 6 EB simplex KRT5, KRT14 Keratins 5 and 14 46 Ectodermal dysplasia with skin fragility PKP1 Plakophilin 1 47 Hailey-Hailey disease ATP2C1 ATP-dependent calcium transporter 13 Keratinization disorders Epidermolytic hyperkeratosis KRT1, KRT10 Keratins 1 and 10 46 Ichthyosis hystrix KRT1 Keratin 1 48 Epidermolytic PPK KRT9 Keratin 9 46 Nonepidermolytic PPK KRT1, KRT16 Keratins 1 and 16 46 Ichthyosis bullosa of Siemens KRT2e Keratin 2e 46 Pachyonychia congenita, types 1 and 2 KRT6a, KRT6b, KRT16, Keratins 6a, 6b, 16, and 17 46 KRT17 White sponge naevus KRT4, KRT13 Keratins 4 and 13 46 X-linked recessive ichthyosis STS Steroid sulfatase 49 Lamellar ichthyosis TGM1 Transglutaminase 1 50 Mutilating keratoderma with ichthyosis LOR Loricrin 10 Vohwinkel’s syndrome GJB2 Connexin 26 12 PPK with deafness GJB2 Connexin 26 12 Erythrokeratodermia variabilis GJB3, GJB4 Connexins 31 and 30.3 12 Darier disease ATP2A2 ATP-dependent calcium 14 transporter Striate PPK DSP, DSG1 Desmoplakin, desmoglein 1 51, 52 Conradi-Hu¨nermann-Happle syndrome EBP Delta 8-delta 7 sterol isomerase 53 (emopamil binding protein) Mal de Meleda ARS SLURP-1 -

Symptomatology, Pathology, Diagnosis
I I I t' 0[ I I I' I Symptomatology, pathology, diagnosis Edited by A.A. Buck I l ! @ World Health Organization Geneva The ll/orld Heolth Organization ( ,yHO ) is one of the specialized agencies in realtion- ship with the United Nations. Through this organization, which came into beine in 7948, the public health and medical professions of more than 130 countries exchange their know- ledge and experience and collaborate in an effort to achieve the highest possible level of health throughout the world. ll/HO is concerned primarily with problems that individual countries or territories cannot solve with their own resources-for example, the eradication or control of malaria, schistosomiasis, smallpox, and other communicable diseases, as well as some cardiovascular diseases and cancer. Progress towards better health throughout the world also demands international cooperation in many other activities: for example, setting up international standards for biological substances, for pesticides andfor pesticide spraying equipment ; compiling aninternationalpharmacopoeia ; drawing up and administer- ing the International Heolth Regulations; revising the international lists of diseases and causes of death ; assembling and disseminating epidemiological information ; recommending nonproprietary names for drugs; and promoting the exchange of scientific knowledge. In many parts ofthe world there is need for improvement in maternal and child health, nutrition, nursing, mental health, dental health, social and occupational health, environmental health, public health administrotion, professional education and training, and health education of the public. Thus a large share oJ'the Organization's resources is devotedtogivingassistance and advice in these fields and to making available-often through publications-the latest information on these subjects. -

Differential Diagnosis of Leprosy
(IfTDICAnOHAL JOutNAL OP UPROSY Volume 59. Number 2 Printed in the U.S.A. Differential Diagnosis of leprosy / K. F. Schaller! From time immemorial leprosy has often Numerous features of macular diseases been mistaken for numerous other diseases resemble leprous disease patterns; howev (I). In countries where leprosy is endemic, er, in most cases these diseases can be other diseases are not infrequently taken to excluded because of the negative result of be leprosy. In areas where leprosy is Dot the sensitivity test. Melanoderma and leu endemic, the disease is easily overlooked or coderma, vitiligo, pinta, tinea versicolor not recognized. The simultaneous presence and nevus anemicus, can be cited as exam of several diseases should also be taken into ples, to mention only a few of them. In one consideration, because they may be con single case, a patient with an extensive fused with one another, or one may conceal vitiligo suffered simultaneously from inde another. It has also not been proven that terminate leprosy. Even clinically normal the presence of leprosy precludes other appearing skin can show the histopatholog diseases or that it is a forerunner of them, ic picture of leprosy, a condition known as with the exception of the sequelae of lepro diffuse lepromatosis, which was first de sy. Thus, in Ethiopia sporadic cases of scribed in Mexican patients (Figs. 1-4). tetanus could be observed, tbough leprosy The papular lesions and plaques may be patients are always said to be immune mistaken for psoriasis, lichen ruber planus, against tetanus. However, with the great superficial mycoses, "tuberculoid" types of number of ulcerations and lesions of the leishmaniasis, syphilis, pityriasis rosea, and skin, a higher occurrence of tetanus cases neurodermitis circumscripta. -

Granuloma Multiforme: a Rare Granulomatous Disease
Hindawi Case Reports in Dermatological Medicine Volume 2019, Article ID 5485034, 3 pages https://doi.org/10.1155/2019/5485034 Case Report Granuloma Multiforme: A Rare Granulomatous Disease Yogesh Poudyal 1 and Anita Shah2 1Sarnath Skin Centre, Shanti Path, Bhairahawa 32900, Nepal 2Department of Pathology, Universal College of Medical Sciences-Teaching Hospital, Ranigaon, Bhairahawa 32900, Nepal Correspondence should be addressed to Yogesh Poudyal; [email protected] Received 28 May 2019; Accepted 5 August 2019; Published 7 October 2019 Academic Editor: Ravi Krishnan Copyright © 2019 Yogesh Poudyal and Anita Shah. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Granuloma Multiforme (GM) is a reactive skin disorder with annular lesion and focal necrobiosis. It was rst described in Nigeria (Africa), since than it was mostly described from various regions of Africa where leprosy was endemic. Outside Africa, this disease is rarely reported. Till 2016 only ve cases were reported from India. is is the second case report from Nepal. A y-nine-year-old female, farmer by occupation, presented with annular and polycyclic plaques with elevated beaded border for one year. It was distributed over upper trunk, lower back, and arms, and was mildly pruritic. Histopathologically, loss of elastic bres at focal area of upper dermis, with elastic bres engulfed histiocytes were noted. GM was mostly noted from leprosy endemic areas of Africa. Clinically, it is very dicult to distinguish from granuloma annulare. is report adds the number of GM occurrence in Asia especially from area where leprosy is still prevalent. -

Granuloma Multiforme: a Report from India
Case GGranulomaranuloma multiforme:multiforme: A rreporteport ffromrom IIndiandia Report RRashmiashmi Kumari,Kumari, DDevinderevinder MMohanohan Thappa,Thappa, AbhijitAbhijit Chougule,Chougule, BalajiBalaji AdityanAdityan Department of Dermatology ABSTRACT and STD, Jawaharlal Institute of Postgraduate Medical Education Granuloma multiforme (GM) is a reactive skin disorder of unknown etiology, characterized and Research (JIPMER), clinically by conß uent annular lesions and histologically by focal necrobiosis and histiocytic Pondicherry - 605 006, India granulomas. GM is signiÞ cant because of its clinical resemblance to tuberculoid leprosy, with which it can be confused. Here, we report a case of granuloma multiforme from India in Address for correspondence: Dr. Devinder Mohan Thappa, a 70-year-old male farmer, with multiple asymptomatic large annular rings of papules over Departments of Dermatology the back and thighs on photodistributed sites. Histopathology helps to clinch the diagnosis and STD, JIPMER, and differentiate from similar clinical and histologic mimics such as granuloma annulare, Pondicherry - 605 006, India. tuberculoid leprosy, actinic granuloma and annular sarcoid. Nevertheless, a very high degree E-mail:[email protected] of suspicion is required to diagnose GM. DOI: 10.4103/0378-6323.51259 PMID: 19439886 Key words: Granuloma multiforme, Annular lesions, Leprosy IINTRODUCTIONNTRODUCTION no history of itching, scaling, burning or decreased sensation associated with the lesions. The largest Leiker[1] in 1964 coined the -

The Post Kala-Azar Dermal Leishmaniasis (PKDL) Atlas a Manual for Health Workers WHO Library Cataloguing-In-Publication Data
The Post Kala-azar Dermal Leishmaniasis (PKDL) Atlas A Manual for Health Workers WHO Library Cataloguing-in-Publication Data The Post Kala-azar Dermal Leishmaniasis (PKDL) atlas: a manual for health workers. 1. Leishmaniasis, Visceral - diagnosis. 2. Leishmaniasis, Cutaneous – diagnosis. 3. Health personnel – education. 4. Handbooks. I. World Health Organization. ISBN 978 92 4 150410 2 (NLM classification: WC 715) WHO/HTM/NTD/IDM/2012.4 © World Health Organization 2012 All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form/en/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -
Colour Atlas of Tropical Dermatology and Venerology
K.F. Schaller (Editor) Colour Atlas of Tropical Dermatology and Venerology In collaboration with F. A. Bahmer • D. W. Biittner • H. Lieske • H. Rieth S. W. Wassilew • F. Weyer With 601 Figures in Colour Springer-Verlag Berlin Heidelberg New York London Paris Tokyo Hong Kong Barcelona Budapest Table of Contents Chapter 1 Viral Diseases of the Skin 1 Ecthyma 49 Erysipelas 50 Variola Vera 1 Scarlatina 51 Molluscum Contagiosum 3 Varicella 4 Nonpyococcal Infections 52 Herpes Zoster 5 Pseudofolliculitis 52 Herpes Simplex 6 Folliculitis Cheloidalis 53 Verrucae Planae 7 Tropical Ulcer 54 Verrucae Vulgares 8 Anthrax 55 Verrucae Plantares 9 Bartonellosis 56 Condylomata Acuminata 10 Rhinoscleroma 57 Epidermodysplasia Verruciformis 11 Erysipeloid 58 Measles 12 Cancrum Oris 58 Rubella 13 Erythrasma 59 Dengue Fever 13 Plague 60 Sandfly Fever 14 Rat Bite Fever 62 Human Immunodeficiency Virus Infection 15 Chapter 4 Endemic Treponematoses 63 Chapter 2 Rickettsial Diseases 16 Yaws 64 Epidemic Typhus 16 Pinta 68 Endemic Typhus 17 Endemic Syphilis 69 Rocky Mountain Spotted Fever 18 Tick Bite Fever 19 Chapter 5 Sexually Transmitted Diseases 70 Rickettsial Pox 20 Scrub Typhus 21 Syphilis 70 Gonorrhoea 74 Chancroid 75 Chapter 3 Bacterial Dermatoses 22 Lymphogranuloma Venereum 76 Granuloma Inguinale 77 Mycobacterial Infections 22 Leprosy 22 Tuberculosis 37 Chapter 6 Superficial Fungal Dermatoses 79 Mycobacterium ulcerans Infection 39 Tinea Imbricata 79 Mycobacterium marinum Infection ' 40 Tinea Nigra 80 Pyococcal Infections 41 Piedra 81 Follicular Impetigo 41 -
Copyrighted Material
1 Index Note: Page numbers in italics refer to figures, those in bold refer to tables and boxes. References are to pages within chapters, thus 58.10 is page 10 of Chapter 58. A definition 87.2 congenital ichthyoses 65.38–9 differential diagnosis 90.62 A fibres 85.1, 85.2 dermatomyositis association 88.21 discoid lupus erythematosus occupational 90.56–9 α-adrenoceptor agonists 106.8 differential diagnosis 87.5 treatment 89.41 chemical origin 130.10–12 abacavir disease course 87.5 hand eczema treatment 39.18 clinical features 90.58 drug eruptions 31.18 drug-induced 87.4 hidradenitis suppurativa management definition 90.56 HLA allele association 12.5 endocrine disorder skin signs 149.10, 92.10 differential diagnosis 90.57 hypersensitivity 119.6 149.11 keratitis–ichthyosis–deafness syndrome epidemiology 90.58 pharmacological hypersensitivity 31.10– epidemiology 87.3 treatment 65.32 investigations 90.58–9 11 familial 87.4 keratoacanthoma treatment 142.36 management 90.59 ABCA12 gene mutations 65.7 familial partial lipodystrophy neutral lipid storage disease with papular elastorrhexis differential ABCC6 gene mutations 72.27, 72.30 association 74.2 ichthyosis treatment 65.33 diagnosis 96.30 ABCC11 gene mutations 94.16 generalized 87.4 pityriasis rubra pilaris treatment 36.5, penile 111.19 abdominal wall, lymphoedema 105.20–1 genital 111.27 36.6 photodynamic therapy 22.7 ABHD5 gene mutations 65.32 HIV infection 31.12 psoriasis pomade 90.17 abrasions, sports injuries 123.16 investigations 87.5 generalized pustular 35.37 prepubertal 90.59–64 Abrikossoff -
Granuloma Multiforme: First Report from Nepal
Case Report Nepal Journal of Dermatology, Venereology & Leprology, Vol 17, No. 1, 2019 http://dx.doi.org/10.3126/njdvl.v17i1.23292 Granuloma Multiforme: First Report from Nepal Paudel S1, Marahatta S2 1Department of Dermatology, 2Department of Pathology, Civil Servive Hospital, Kathmandu. Abstract Granuloma multiforme (GM) is a reactive skin disorder of unknown etiology, characterized clinically by confluent annular lesions and histologically by focal necrobiosis and histiocytic granulomas. GM is significant because it mimics various conditions and diagnosis is often missed if not taken into consideration. Here, we report a case of granuloma multiforme from Nepal in a 40 year old female with multiple skin colored to mildly erythematous, occasionally itchy annular plaques of duration 6 months, over the upper back and upper chest. Histopathology helped to clinch the diagnosis and differentiate from similar clinical and histologic mimics. Key words: Granuloma; Necrobiotic disorders; Nepal; Skin Introduction from 2 to 6 cm in diameter (Figures 1,2). The border was soft to firm in consistency. There was no loss of he term Granuloma Multiforme (GM) was coined sensation over the lesions and no peripheral nerve 1 Tin 1964 by Leiker et al, to describe a reactive thickening. Systemic examination was normal. skin disorder of unknown etiology which resembled leprosy but had different histology. GM is a chronic Clinical possibilities considered were granuloma granulomatous skin condition, characterized clinically annulare, actinic granuloma, annular sarcoid and by firm papules aggregated into plaques or forming granuloma multiforme. Routine lab investigations and the edges of annular lesions, and histologically by focal Chest X ray were all normal. -

Dnb- Dermatology, Venereology & Leprosy
Guidelines for Competency Based Training Programme in DNB- DERMATOLOGY, VENEREOLOGY & LEPROSY NATIONAL BOARD OF EXAMINATIONS Medical Enclave, Ansari Nagar, New Delhi-110029, INDIA Email: [email protected] Phone: 011 45593000 1 CONTENTS I. OBJECTIVES OF THE PROGRAMME a) Programme goal b) Programme objective II. ELIGIBILITY CRITERIA FOR ADMISSION III. TEACHING AND TRAINING ACTIVITIES IV. SYLLABUS V. COMPETENCIES VI. THESIS & THESIS PROTOCOL VII. LOG BOOK VIII. NBE LEAVE GUIDELINES IX. EXAMINATION – a) FORMATIVE ASSESSMENT b) FINAL THEORY & PRACTICAL X. RECOMMENDED TEXT BOOKS AND JOURNALS 2 PROGRAMME GOAL To provide uniform, standard training in Dermatology, Venereology and Leprosy to the candidates so that after 3 years of training they are able to acquire the necessary competencies in the specialty to work as Senior Resident/ Junior Consultant PROGRAMME OBJECTIVES The students after the training should be able to: Provide quality patient care Able to perform Clinical examination & relevant laboratory investigations Adopt a compassionate attitude towards the patient (and their families) under his/her charge Describe preventive measures at individual and community levels against communicable Skin, Leprosy and Venereal diseases Manage independently and efficiently all medical emergencies related with skin, leprosy and venereal disease Describe the current treatment modalities and awareness of latest treatment of various diseases of skin, STD and leprosy. Teach the medical and Paramedical students in the specialties Conduct research in the field of Skin, Venereal diseases & Leprosy Describe the preventive aspects, education, counseling services to the patient and National Control Program of India for Leprosy, STDs and HIV infections. 3 ELIGIBILITY CRITERIA FOR ADMISSIONS TO THE PROGRAMME (A) DNB Dermatology , Venereology and Leprosy Course: 1.