Guidelines for the Management of Leprosy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clinicopathological Features of Annular Elastolytic Giant Cell
Original Investigation / Özgün Araştırma Turk J Dermatol 2018;12:85-9 • DOI: 10.4274/tdd.3409 85 Hilal Kaya Clinicopathological Features of Annular Erdoğan, Deniz Arık*, Elastolytic Giant Cell Granuloma Patients Ersoy Acer, Evrim Yılmaz*, Anüler Elastolitik Dev Hücreli Granülom Zeynep Nurhan Hastalarının Klinikopatolojik Özellikleri Saraçoğlu Abstract Objective: Annular elastolytic giant cell granuloma (AEGCG) is a rare granulomatous disease characterized by annular plaques. In this study, we aimed to describe the clinical and pathological features of the patients diagnosed with AEGCG. Methods: The demographic, clinical and pathological features of patients who diagnosed with AEGCG were recorded retrospectively. Results: Ten patients with AEGCG included in the study (nine females and one male). The mean age of the patients was 60±9.53 years. The mean duration of disease was 24.2±36.30 months. On dermatologic examination, multiple, well-demarcated, elevated borders and central atrophic erythematous annular plaques were seen in all patients. In the most of the patients (90%) lesions were on the sun-exposed regions. Six of the patients had accompanying diseases. Histopathologic examination of the punch biopsies revealed foreign body type multinucleated giant cells and lymphocytic cell infiltration in the dermis. There were intracellular elastic fiber fragments as sign of elastophagocytosis in the giant cells. Conclusion: AEGCG is a rare granulomatous disease which can accompany various diseases. There is debate on the terminology, classification and pathogenesis. Further studies are required to elucidate the unknowns. Keywords: Annular elastolytic giant cell granuloma, elastophagocytosis, granulomatous diseases, elastolysis, giant cell, granuloma annulare Eskişehir Osmangazi University Faculty of Medicine, Öz Department of Dermatology and Venereology, Amaç: Anüler elastolitik dev hücreli granülom (AEDHG), anüler plaklar ile karakterize, Eskişehir, Turkey nadir granülomatöz bir hastalıktır. -

White Lesions of the Oral Cavity and Derive a Differential Diagnosis Four for Various White Lesions
2014 self-study course four course The Ohio State University College of Dentistry is a recognized provider for ADA, CERP, and AGD Fellowship, Mastership and Maintenance credit. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at www.ada.org/goto/cerp. The Ohio State University College of Dentistry is approved by the Ohio State Dental Board as a permanent sponsor of continuing dental education ABOUT this FREQUENTLY asked COURSE… QUESTIONS… Q: Who can earn FREE CE credits? . READ the MATERIALS. Read and review the course materials. A: EVERYONE - All dental professionals in your office may earn free CE contact . COMPLETE the TEST. Answer the credits. Each person must read the eight question test. A total of 6/8 course materials and submit an questions must be answered correctly online answer form independently. for credit. us . SUBMIT the ANSWER FORM Q: What if I did not receive a ONLINE. You MUST submit your confirmation ID? answers ONLINE at: A: Once you have fully completed your p h o n e http://dent.osu.edu/sterilization/ce answer form and click “submit” you will be directed to a page with a . RECORD or PRINT THE 614-292-6737 unique confirmation ID. CONFIRMATION ID This unique ID is displayed upon successful submission Q: Where can I find my SMS number? of your answer form. -

Granuloma Annulare: Not As Simple As It Seems
Thomas Jefferson University Jefferson Digital Commons Department of Dermatology and Cutaneous Department of Dermatology and Cutaneous Biology Faculty Papers Biology 9-1-2010 Granuloma annulare: not as simple as it seems. Lawrence Charles Parish Thomas Jefferson University Joseph A. Witkowski University of Pennsylvania School of Medicine Follow this and additional works at: https://jdc.jefferson.edu/dcbfp Part of the Dermatology Commons Let us know how access to this document benefits ouy Recommended Citation Parish, Lawrence Charles and Witkowski, Joseph A., "Granuloma annulare: not as simple as it seems." (2010). Department of Dermatology and Cutaneous Biology Faculty Papers. Paper 76. https://jdc.jefferson.edu/dcbfp/76 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in Department of Dermatology and Cutaneous Biology Faculty Papers by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Granuloma Annulare: Not as simple as -

Interstitial Granuloma Annulare Triggered by Lyme Disease
Volume 27 Number 5| May 2021 Dermatology Online Journal || Case Presentation 27(5):11 Interstitial granuloma annulare triggered by Lyme disease Jordan Hyde1 MD, Jose A Plaza1,2 MD, Jessica Kaffenberger1 MD Affiliations: 1Division of Dermatology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA, 2Department of Pathology, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA Corresponding Author: Jessica Kaffenberger MD, Division of Dermatology, The Ohio State University Medical Wexner Medical Center, Suite 240, 540 Officenter Place, Columbus, OH 43230, Tel: 614-293-1707, Email: [email protected] been associated with a variety of systemic diseases Abstract including diabetes mellitus, malignancy, thyroid Granuloma annulare is a non-infectious disease, dyslipidemia, and infection [3,4]. granulomatous skin condition with multiple different associations. We present a case of a man in his 60s There are multiple histological variants of GA, with a three-week history of progressive targetoid including interstitial GA. The histopathology of plaques on his arms, legs, and trunk. Skin biopsy classic GA demonstrates a focal degeneration of demonstrated interstitial granuloma annulare. collagen surrounded by an inflammatory infiltrate Additional testing revealed IgM antibodies to Borrelia composed of lymphocytes and histiocytes. In a less burgdorferi on western blot suggesting interstitial common variant, interstitial GA, scattered histiocytes granuloma annulare was precipitated by the recent are seen -

2017 Oregon Dental Conference® Course Handout
2017 Oregon Dental Conference® Course Handout Nasser Said-Al-Naief, DDS, MS Course 8125: “The Mouth as The Body’s Mirror: Oral, Maxillofacial, and Head and Neck Manifestations of Systemic Disease” Thursday, April 6 2 pm - 3:30 pm 2/28/2017 The Mouth as The Body’s Mirror Oral Maxillofacial and Head and Neck Manifestation of Ulcerative Conditions of Allergic & Immunological Systemic Disease the Oro-Maxillofacial Diseases Region Nasser Said-Al-Naief, DDS, MS Professor & Chair, Oral Pathology and Radiology Director, OMFP Laboratory Oral manifestations of Office 503-494-8904// Direct: 503-494-0041 systemic diseases Oral Manifestations of Fax: 503-494-8905 Dermatological Diseases Cell: 1-205-215-5699 Common Oral [email protected] Conditions [email protected] OHSU School of Dentistry OHSU School of Medicine 2730 SW Moody Ave, CLSB 5N008 Portland, Oregon 97201 Recurrent aphthous stomatitis (RAS) Recurrent aphthous stomatitis (RAS) • Aphthous" comes from the Greek word "aphtha”- • Recurrence of one or more painful oral ulcers, in periods of days months. = ulcer • Usually begins in childhood or adolescence, • The most common oral mucosal disease in North • May decrease in frequency and severity by age America. (30+). • Affect 5% to 66% of the North American • Ulcers are confined to the lining (non-keratinized) population. mucosa: • * 60% of those affected are members of the • Buccal/labial mucosa, lateral/ventral tongue/floor of professional class. the mouth, soft palate/oropharyngeal mucosa • Etiopathogenesis: 1 2/28/2017 Etiology of RAU Recurrent Aphthous Stomatitis (RAS): Types: Minor; small size, shallow, regular, preceeded by prodrome, heal in 7-10 days Bacteria ( S. -

Foot Pain in Scleroderma
Foot Pain in Scleroderma Dr Begonya Alcacer-Pitarch LMBRU Postdoctoral Research Fellow 20th Anniversary Scleroderma Family Day 16th May 2015 Leeds Institute of Rheumatic and Musculoskeletal Medicine Presentation Content n Introduction n Different types of foot pain n Factors contributing to foot pain n Impact of foot pain on Quality of Life (QoL) Leeds Institute of Rheumatic and Musculoskeletal Medicine Scleroderma n Clinical features of scleroderma – Microvascular (small vessel) and macrovascular (large vessel) damage – Fibrosis of the skin and internal organs – Dysfunction of the immune system n Unknown aetiology n Female to male ratio 4.6 : 1 n The prevalence of SSc in the UK is 8.21 per 100 000 Leeds Institute of Rheumatic and Musculoskeletal Medicine Foot Involvement in SSc n Clinically 90% of SSc patients have foot involvement n It typically has a later involvement than hands n Foot involvement is less frequent than hand involvement, but is potentially disabling Leeds Institute of Rheumatic and Musculoskeletal Medicine Different Types of Foot Pain Leeds Institute of Rheumatic and Musculoskeletal Medicine Ischaemic Pain (vascular) Microvascular disease (small vessel) n Intermittent pain – Raynaud’s (spasm) • Cold • Throb • Numb • Tingle • Pain n Constant pain – Vessel center narrows • Distal pain (toes) • Gradually increasing pain • Intolerable pain when necrosis is present Leeds Institute of Rheumatic and Musculoskeletal Medicine Ischaemic Pain (vascular) Macrovascular disease (large vessels) n Intermittent and constant pain – Peripheral Arterial Disease • Intermittent claudication – Muscle pain (ache, cramp) during walking • Aching or burning pain • Night and rest pain • Cramps Leeds Institute of Rheumatic and Musculoskeletal Medicine Ulcer Pain n Ulcer development – Constant pain n Infected ulcer – Unexpected/ excess pain or tenderness Leeds Institute of Rheumatic and Musculoskeletal Medicine Neuropathic Pain n Nerve damage is not always obvious. -

A Patient with Plaque Type Morphea Mimicking Systemic Lupus Erythematosus
CASE REPORT A Patient With Plaque Type Morphea Mimicking Systemic Lupus Erythematosus Wardhana1, EA Datau2 1 Department of Internal Medicine, Siloam International Hospitals. Karawaci, Indonesia. 2 Department of Internal Medicine, Prof. Dr. RD Kandou General Hospital & Sitti Maryam Islamic Hospital, Manado, North Sulawesi, Indonesia. Correspondence mail: Siloam Hospitals Group’s CEO Office, Siloam Hospital Lippo Village. 5th floor. Jl. Siloam No.6, Karawaci, Indonesia. email: [email protected] ABSTRAK Morfea merupakan penyakit jaringan penyambung yang jarang dengan gambaran utama berupa penebalan dermis tanpa disertai keterlibatan organ dalam. Penyakit ini juga dikenal sebagai bagian dari skleroderma terlokalisir. Berdasarkan gambaran klinis dan kedalaman jaringan yang terlibat, morfea dikelompokkan ke dalam beberapa bentuk dan sekitar dua pertiga orang dewasa dengan morfea mempunyai tipe plak. Produksi kolagen yang berlebihan oleh fibroblast merupakan penyebab kelainan pada morfea dan mekanisme terjadinya aktivitas fibroblast yang berlebihan ini masih belum diketahui, meskipun beberapa mekanisme pernah diajukan. Morfe tipe plak biasanya bersifat ringan dan dapat sembuh dengan sendirinya. Morfea tipe plak yang penampilan klinisnya menyerupai lupus eritematosus sistemik, misalnya meliputi alopesia dan ulkus mukosa di mulut, jarang dijumpai. Sebuah kasus morfea tipe plak pada wanita berusia 20 tahun dibahas. Pasien ini diobati dengan imunosupresan dan antioksidan local maupun sistemik. Kondisi paisen membaik tanpa disertai efek samping yang berarti. Kata kunci: morfea, tipe plak. ABSTRACT Morphea is an uncommon connective tissue disease with the most prominent feature being thickening or fibrosis of the dermal without internal organ involvement. It is also known as a part of localized scleroderma. Based on clinical presentation and depth of tissue involvement, morphea is classified into several forms, and about two thirds of adults with morphea have plaque type. -

Tocaloma Spa Services Menu
Massage Tocaloma Signature 80 min. $210 Seaweed Body Wrap 50 min. $130 Restore Moisture Miracle Facial 50 min. $170 A decadent massage fully customizable to your specific Helps release stored toxins and relieve fluid retention, as When skin is stressed and compromised, it needs a needs. Includes a hydrating hand treatment and scalp well as hormonal and adrenal balancing. A body brush is restorative moisture miracle. This anti-aging facial will massage for the ultimate relaxation. used to exfoliate dead skin cells. Next, a warmed infuse deep hydration while boosting firmness leaving your application of seaweed envelopes the body while a skin feeling soft, nourished and renewed. Swedish 20 mins. $80 | 50 min. $120 | 80 min. $180 relaxing scalp massage soothes stress. After a eucalyptus Acne Clarifying Facial 50 min. $140 This treatment is ideal when arriving at Tapatio to welcome shower, moisture-rich body lotion is applied to leave skin you and ground your energy. Therapists focus on areas silky smooth. Improve skin clarity while combating acne and unbalanced prone to tension after traveling while utilizing long, relaxing skin. Improve skin smoothness, balance oil production, Sedona Purification Body Wrap 50 min. $130 strokes of light to medium pressure, providing instant relief unclog pores and speed up skin cell turnover while creating of pain and stiffness. Rich in minerals from the Arizona desert and derived from an overall glow and revealing healthy skin. the clays of the Southwest, this treatment will nourish, tone Therapeutic 20 mins. $100 | 50 min. $140 | 80 min. $200 Lighten & Brighten Facial 50 min. $160 and purify your skin. -

Botulinum Toxin in the Treatment of Sweatworsened Foot Problems In
15 March 2005 Use of Articles in the Pachyonychia Congenita Bibliography The articles in the PC Bibliography may be restricted by copyright laws. These have been made available to you by PC Project for the exclusive use in teaching, scholar- ship or research regarding Pachyonychia Congenita. To the best of our understanding, in supplying this material to you we have followed the guidelines of Sec 107 regarding fair use of copyright materials. That section reads as follows: Sec. 107. - Limitations on exclusive rights: Fair use Notwithstanding the provisions of sections 106 and 106A, the fair use of a copyrighted work, including such use by reproduction in copies or phonorecords or by any other means specified by that section, for purposes such as criticism, comment, news reporting, teaching (including multiple copies for classroom use), scholarship, or research, is not an infringement of copyright. In determining whether the use made of a work in any particular case is a fair use the factors to be considered shall include - (1) the purpose and character of the use, including whether such use is of a commercial nature or is for nonprofit educational purposes; (2) the nature of the copyrighted work; (3) the amount and substantiality of the portion used in relation to the copyrighted work as a whole; and (4) the effect of the use upon the potential market for or value of the copyrighted work. The fact that a work is unpublished shall not itself bar a finding of fair use if such finding is made upon consideration of all the above factors. -

“Relationship Between Smoking and Plantar Callus
C HA PTER 3 8 RELATIONSHIP BETWEEN SMOKING AND PLANTAR CALLUS FORMATION OF THE FOOT Thomas J. Merrill, DPM Virginio Vena, DPM Luis A. Rodriguez, DPM Despite the decline in cigarette smoking in the last few smoke can remain in the body (6). The tobacco smoke years as reported by the Centers for Disease Control and components absorbed from the lungs reach the heart Prevention, and the well known health risks in cardiovascular immediately. Smoking increases the heart rate, arterial blood and pulmonary diseases, millions of Americans continue to pressure, and cardiac output. There is a 42% reduction in the smoke cigarettes. It has been proven by both experimental digital blood flow after a single cigarette (7, 8). Nicotine has and clinical observation that cigarettes impair bone and a direct cutaneous vasoconstrictive effect and is the principle wound healing. The purpose of this article is to review the vasoactive component in the gas phase of cigarette smoke. chemical components of cigarette smoke and its relationship It is an odorless, colorless, and poisonous alkaloid that when with plantar callus formation. inhaled or injected, can activate the adrenal catecholamines Increased plantar callus formation with patients who from the adrenergic nerve endings and from the adrenal smoke cigarettes seems to be a common problem. There are medulla, which cause vasoconstriction of vessels especially in approximately 46.6 million smokers in the US. There was a the extremities. Nicotine also induces the sympathetic decline during 1997-2003 in the youth population but nervous system, which results in the release of epinephrine during the last years the rates are stable (1). -
Nodular Morphea
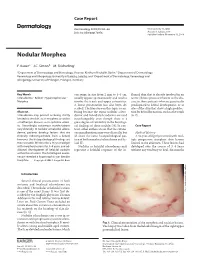
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable. -

For Peer Review Only
Expert Opinion On Drug Metabolism & Toxicology For Peer Review Only Please download and read the Referee Guidelines Intravenous immunoglobulin: pharmacological properties and use in polyneuropathies Journal: Expert Opinion On Drug Metabolism and Toxicology Manuscript ID EOMT-2016-0106.R1 Manuscript Type: Review IVIg, CIDP, GBS, anti-idiotype antibodies, anti-ganglioside antibodies, Keywords: sialylation, IgG molecule., Fc receptors URL: http://mc.manuscriptcentral.com/eomt Email: [email protected] Page 1 of 60 Expert Opinion On Drug Metabolism & Toxicology 1 2 Abstract 3 4 Introduction: Intravenous immunoglobulin (IVIg) is increasingly used for the treatment of 5 6 autoimmune and systemic inflammatory diseases with both licensed and off-label indications. The 7 mechanism of action is complex and not fully understood, involving the neutralization of 8 9 pathological antibodies, Fc receptor blockade, complement inhibition, immunoregulation of 10 11 dendritic cells, B cells and T cells and the modulation of apoptosis. 12 13 14 Areas covered:For First, this Peerreview describes Review the pharmacological propertiesOnly of IVIg, including the 15 16 composition, mechanism of action, and adverse events. The second part gives an overview of some 17 of the immune-mediated polyneuropathies, with special focus on the pathomechanism and clinical 18 19 trials assessing the efficacy of IVIg. A literature search on PubMed was performed using the terms 20 21 IVIg, IVIg preparations, side effects, mechanism of action, clinical trials, GBS, CIDP. 22 23 24 Expert opinion: Challenges associated with IVIg therapy and the treatment possibilities for 25 26 immune-mediated polyneuropathies are discussed. The availability of IVIg is limited, the expenses 27 are high, and, in several diseases, a chronic therapy is necessary to maintain the immunomodulatory 28 29 effect.