Identifying Necrolytic Migratory Erythema in Glucagonoma Syndrome
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Endocrine Tumors of the Pancreas
Friday, November 4, 2005 8:30 - 10:30 a. m. Pancreatic Tumors, Session 2 Chairman: R. Jensen, Bethesda, MD, USA 9:00 - 9:30 a. m. Working Group Session Pathology and Genetics Group leaders: J.–Y. Scoazec, Lyon, France Questions to be answered: 12 Medicine and Clinical Pathology Group leader: K. Öberg, Uppsala, Sweden Questions to be answered: 17 Surgery Group leader: B. Niederle, Vienna, Austria Questions to be answered: 11 Imaging Group leaders: S. Pauwels, Brussels, Belgium; D.J. Kwekkeboom, Rotterdam, The Netherlands Questions to be answered: 4 Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging ENETS Guidelines Neuroendocrinology 2004;80:394–424 Endocrine Tumors of the Pancreas - gastrinoma Epidemiology The incidence of clinically detected tumours has been reported to be 4-12 per million inhabitants, which is much lower than what is reported from autopsy series (about 1%) (5,13). Clinicopathological staging (12, 14, 15) Well-differentiated tumours are the large majority of which the two largest fractions are insulinomas (about 40% of cases) and non-functioning tumours (30-35%). When confined to the pancreas, non-angioinvasive, <2 cm in size, with <2 mitoses per 10 high power field (HPF) and <2% Ki-67 proliferation index are classified as of benign behaviour (WHO group 1) and, with the notable exception of insulinomas, are non-functioning. Tumours confined to the pancreas but > 2 cm in size, with angioinvasion and /or perineural space invasion, or >2mitoses >2cm in size, >2 mitoses per 20 HPF or >2% Ki-67 proliferation index, either non-functioning or functioning (gastrinoma, insulinoma, glucagonoma, somastatinoma or with ectopic syndromes, such as Cushing’s syndrome (ectopic ACTH syndrome), hypercaliemia (PTHrpoma) or acromegaly (GHRHoma)) still belong to the (WHO group 1) but are classified as tumours with uncertain behaviour. -
C O N F E R E N C E 7 18 October 2017
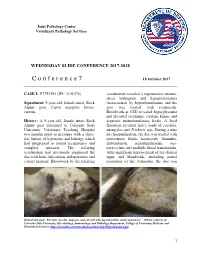
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2017-2018 C o n f e r e n c e 7 18 October 2017 CASE I: F1753191 (JPC 4101076). veterinarian revealed a regenerative anemia, stress leukogram and hypoproteinemia Signalment: 9-year-old, female intact, Rock characterized by hypoalbuminemia and the Alpine goat, Capra aegagrus hircus, goat was treated with ivermectin. caprine. Bloodwork at CSU revealed hyperglycemia and elevated creatinine, creatine kinase and History: A 9-year-old, female intact Rock aspartate aminotransferase levels. A fecal Alpine goat presented to Colorado State floatation revealed heavy loads of coccidia, University Veterinary Teaching Hospital strongyles and Trichuris spp. During a nine two months prior to necropsy with a three- day hospitalization, the doe was treated with day history of hyporexia and lethargy which intravenous fluids, kaopectate, thiamine, had progressed to lateral recumbency and fenbendazole, sulfadimethoxine, oxy- complete anorexia. The referring tetracycline and multiple blood transfusions. veterinarian had previously diagnosed the After significant improvement of her clinical doe with louse infestation, endoparasites and signs and bloodwork, including partial a heart murmur. Bloodwork by the referring resolution of the dermatitis, the doe was Haired skin goat. The skin was dry, alopecia, and covered with hyperkeratotic crusts and ulcers. (Photo courtesy of: Colorado State University, Microbiology, Immunology, and Pathology Department, College of Veterinary Medicine and Biomedical Sciences, http://csucvmbs.colostate.edu/academics/mip/Pages/default.aspx) 1 discharged. exfoliating epithelial crusts which were often tangled within scant remaining hairs. Two months later, the goat presented with a This lesion most severely affected the skin one month history of progressive scaling and over the epaxials, the ventral abdomen and ulceration over the withers, dew claws, and teats, coronary bands and dew claws. -

Production of the a Subunit of Guanine Nucleotide-Binding Protein GO by Neuroendocrine Tumors1
[CANCER RESEARCH 47, 5800-5805, November 1, 1987] Production of the a Subunit of Guanine Nucleotide-binding Protein GO by Neuroendocrine Tumors1 Kanefusa Kato,2 Tomiko Asano, Nobuko Kamiya, Hajime Haimoto, Syun Hosoda, Akio Nagasaka, Yutaka Ariyoshi, and Yukio Ishiguro Department of Biochemistry ¡K.K„T.A., N. K.], Institute for Developmental Research, Aichi Prefectural Colony, Kasugai, Aichi 480-03; Laboratory of Pathology ¡H.H., S. H.] and Department of Internal Medicine [Y, A.], Aichi Cancer Center, Chikusa-ku, Nagoya 464; Department of Internal Medicine [A. N.J. Fujita-Gakuen Health University, School of Medicine, Toyoake, Aichi 470-11; and Department of Surgery [Y. IJ, Nagoya University School of Medicine, Showa-ku, Nagoya 466, Japan ABSTRACT is localized exclusively in the nervous tissues and some endo crine cells in pancreas, pituitary, thyroid, and adrenal,4 which We have found that neuroendocrine tumors (including neuroblastoma, belong to a family designated as APUD (amine precursor ganglioneuroma, gut carcinoid, pheochromocytoma, medullary thyroid uptake and decarboxylation) or diffuse neuroendocrine system carcinoma, insulinoma, glucagonoma, prolactinoma, carotid body tumor, (10). We describe here the presence of G0«in tumors derived and small cell lung carcinoma) produce considerable amounts (about 1000-80,000 ng/g tissue) of the a subunit of guanine nucleotide-binding from the above mentioned neuroendocrine cells and in sera of protein, G0 (Goa), whereas nonneuroendocrine tumors contain less than patients with neuroblastoma, and evaluate G0a for the appli 300 ng of Goa/g tissue. Goat in the neuroendocrine tumors was present cation to clinical and immunohistochemical diagnosis. both in the soluble fraction, and cholate-extractable membrane-bound fraction of tissues. -

Rising Incidence of Neuroendocrine Tumors
Rising Incidence of Neuroendocrine Tumors Dasari V, Yao J, et al. JAMA Oncology 2017 S L I D E 1 Overview Pancreatic Neuroendocrine Tumors • Tumors which arise from endocrine cells of the pancreas • 5.6 cases per million – 3% of pancreatic tumors • Median age at diagnosis 60 years • More indolent course compared to adenocarcinoma – 10-year overall survival 40% • Usually sporadic but can be associated with hereditary syndromes – Core genetic pathways altered in sporadic cases • DNA damage repair (MUTYH) Chromatin remodeling (MEN1) • Telomere maintenance (MEN1, DAXX, ATRX) mTOR signaling – Hereditary: 17% of patients with germline mutation Li X, Wang C, et al. Cancer Med 2018 Scarpa A, Grimond S, et al. NatureS L I2017 D E 2 Pathology Classification European American Joint World Health Organization Neuroendocrine Committee on Cancer (WHO) Tumor Society (AJCC) (ENETS) Grade Ki-67 Mitotic rt TNM TNM T1: limit to pancreas, <2 cm T1: limit to pancreas, ≦2 cm T2: limit to pancreas, 2-4 cm T2: >limit to pancreas, 2 cm T3: limit to pancreas, >4 cm, T3: beyond pancreas, no celiac or Low ≤2% <2 invades duodenum, bile duct SMA T4: beyond pancreas, invasion involvement adjacent organs or vessels T4: involves celiac or SMA N0: node negative No: node negative Intermed 3-20% 2-20 N1: node positive N1: node positive M0: no metastases M0: no metastases High >20% >20 M1: metastases M1: metastases S L I D E 3 Classification Based on Functionality • Nonfunctioning tumors – No clinical symptoms (can still produce hormone) – Accounts for 40% of tumors – 60-85% -

Preclinical Cushing's Syndrome Resulting from Adrenal Black
Endocrine Journal 2007, 54 (4), 543–551 Preclinical Cushing’s Syndrome Resulting from Adrenal Black Adenoma Diagnosed with Diabetic Ketoacidosis TOSHIO KAHARA, CHIKASHI SETO*, AKIO UCHIYAMA**, DAISUKE USUDA, HIROSHI AKAHORI, EIJI TAJIKA*, ATSUO MIWA**, RIKA USUDA, TAKASHI SUZUKI*** AND HIRONOBU SASANO*** Department of Internal Medicine, Toyama Prefectural Central Hospital, 2-2-78 Nishinagae, Toyama 930-8550, Japan *Department of Urology, Toyama Prefectural Central Hospital, 2-2-78 Nishinagae, Toyama 930-8550, Japan **Department of Pathology, Toyama Prefectural Central Hospital, 2-2-78 Nishinagae, Toyama 930-8550, Japan ***Department of Pathology, Tohoku University School of Medicine, 2-1 Seiryo-machi, Aoba-ku, Sendai 980-8575, Japan Abstract. A right adrenal tumor was incidentally discovered on abdominal computed tomography performed on a 53- year-old Japanese man, who had been hospitalized with diabetic ketoacidosis. Normal values were obtained for adrenal hormones in the morning after an overnight fast and urinary cortisol excretion after treatment of diabetic ketoacidosis with insulin. However, overnight dexamethasone administration with 1 mg or 8 mg did not completely suppress serum cortisol levels. There were no remarkable physical findings related to Cushing’s syndrome. The patient was diagnosed as having preclinical Cushing’s syndrome (PCS). Histological examination of the adrenalectomy specimen demonstrated adrenal black adenoma. Blood glucose levels subsequently improved after adrenalectomy, and the patient never developed adrenal insufficiency after hydrocortisone withdrawal. The patient was treated with diet therapy alone, and maintained good glycemic control. However, the patient still showed a diabetic pattern in an oral glucose tolerance test. It seems that the existence of PCS in addition to the underlying type 2 diabetes mellitus contributed to aggravation of blood glucose levels. -

The Glucagonoma Syndrome And
European Journal of Endocrinology (2004) 151 531–537 ISSN 0804-4643 REVIEW The glucagonoma syndrome and necrolytic migratory erythema: a clinical review Andre´ P van Beek, Ellen R M de Haas1, Willem A van Vloten2, Cees J M Lips3, Janine F M Roijers3 and Marijke R Canninga-van Dijk4 University Medical Center Groningen, Department of Endocrinology, PO Box 30.001, 9700 RB, Groningen, 1Erasmus MC - University Medical Center Rotterdam, Department of Dermatology, PO Box 1738, 3000 DR, Rotterdam, and Departments of 2Dermatology, 3Endocrinology and 4Pathology, University Medical Center Utrecht, PO Box 85.500, 3508 GA, Utrecht, The Netherlands (Correspondence should be addressed to A P van Beek; Email: [email protected]) Abstract The glucagonoma syndrome is a rare disease in which a typical skin disorder, necrolytic migratory erythema, is often one of the first presenting symptoms. Weight loss and diabetes mellitus are two other prevalent characteristics of this syndrome. Necrolytic migratory erythema belongs to the recently recognized family of deficiency dermatoses of which zinc deficiency, necrolytic acral erythema and pellagra are also members. It is typically characterized on skin biopsies by necrolysis of the upper epidermis with vacuolated keratinocytes. In persistent hyperglucagonemia, excessive stimulation of basic metabolic pathways results in diabetes mellitus at the expense of tissue glycogen stores, and muscle and fat mass. Multiple (essential) nutrient and vitamin B deficiencies develop, which contrib- ute to the dermatosis. In addition, glucagonomas may produce various other products, like pancreatic polypeptide, that add to the catabolic effects of glucagon. European Journal of Endocrinology 151 531–537 Introduction an appendectomy and at age 50 he was operated on because of bilateral inguinal herniae. -

Clinical Presentation and Diagnosis of Pancreatic Neuroendocrine Tumors
Clinical Presentation and Diagnosis of Pancreatic Neuroendocrine Tumors Carinne W. Anderson, MD*, Joseph J. Bennett, MD KEYWORDS Pancreatic neuroendocrine tumor Nonfunctional pancreatic neuroendocrine tumor Insulinoma Gastrinoma Glucagonoma VIPoma Somatostatinoma KEY POINTS Pancreatic neuroendocrine tumors are a rare group of neoplasms, most of which are nonfunctioning. Functional pancreatic neoplasms secrete hormones that produce unique clinical syndromes. The key management of these rare tumors is to first suspect the diagnosis; to do this, cli- nicians must be familiar with their clinical syndromes. Pancreatic neuroendocrine tumors (PNETs) are a rare group of neoplasms that arise from multipotent stem cells in the pancreatic ductal epithelium. Most PNETs are nonfunctioning, but they can secrete various hormones resulting in unique clinical syn- dromes. Clinicians must be aware of the diverse manifestations of this disease, as the key step to management of these rare tumors is to first suspect the diagnosis. In light of that, this article focuses on the clinical features of different PNETs. Surgical and medical management will not be discussed here, as they are addressed in other arti- cles in this issue. EPIDEMIOLOGY Classification PNETs are classified clinically as nonfunctional or functional, based on the properties of the hormones they secrete and their ability to produce a clinical syndrome. Nonfunctional PNETs (NF-PNETs) do not produce a clinical syndrome simply because they do not secrete hormones or because the hormones that are secreted do not The authors have nothing to disclose. Department of Surgery, Helen F. Graham Cancer Center, 4701 Ogletown-Stanton Road, S-4000, Newark, DE 19713, USA * Corresponding author. E-mail address: [email protected] Surg Oncol Clin N Am 25 (2016) 363–374 http://dx.doi.org/10.1016/j.soc.2015.12.003 surgonc.theclinics.com 1055-3207/16/$ – see front matter Ó 2016 Elsevier Inc. -

Evaluation of Hereditary Syndromes That Include Pancreatic Cancer
Evaluation of hereditary syndromes that include pancreatic cancer UPR CCC 04/12/13 Jeffrey N. Weitzel, M.D. Chief, Division of Clinical Cancer Genetics Cancer Screening & Prevention Program City of Hope Comprehensive Cancer Center and Beckman Research Institute PANCREATIC CANCER Worldwide estimates: • Incidence- 232,306 • Deaths- 227,000 A deadly disease CA Cancer J Clin 2012 PANCREATIC CANCER Non-Genetic Risk Factors Cigarette Smoking • Doubles Risk • Causes 26% of pancreatic cancer Obesity • Increases risk by ~70% Diabetes • Longterm (>10yrs) 2-Fold increase (Everhart 1995) • 1% of new-onset diabetics develop pancreatic cancer within 3 years (Chari 2005) DDx: Start with Pathology Adenocarcinoma = >75% 5-year survival <5% Endocrine (AKA: islet cell) = ~ 1% Hormone-producing; control blood sugar levels Insulinoma, gastrinoma, VIPoma, glucagonoma, somatostatinoma, non-functional “oma’s” Slower-growing better prognosis 5-year survival 50-70% if surgically resectable DDx: Endocrine pancreatic tumor(s) MEN1 VHL NF1 TSC sporadic MEN 1 and MEN 2 MEN 1 MEN 2 Anterior Pituitary Thyroid C-cells (MTC) Parathyroid Parathyroid Adrenal Adrenal medulla cortex (pheochromocytoma) Pancreatic islet cells Germline mutations Germline mutations in MEN1, chr 11 in RET, chr 10 Genetics of MEN 1: The Menin Gene Mutations in the MENIN (MEN1) gene on chromosome 11q13 Cloned in 1997 Tumor suppressor gene Involved in transcriptional regulation/cell growth and regulation > 400 distinct mutations identified throughout the gene; most are protein truncating MEN 1 mutation -

Pituitary, Endocrine Pancreas, and Adrenal Pathology
Pituitary, endocrine pancreas, and adrenal pathology Hannes Vogel [email protected] 650-723-9672 Learning Objectives: 1. Describe the histogenesis and normal anatomy of the pituitary gland. 2. Itemize the distinguishing features of normal and neoplastic pituitary parenchyma. 3. Describe the histologic features of various sellar/suprasellar epithelial lesions. 4. Describe the functional and malignant potentials of pancreatic islet-cell tumors. 5. Name the major causes of adrenocortical hyperfunction and insufficiency Reading: Robbins and Cotran pathologic basis of disease. Ninth edition Online: The Endocrine system, pp 1074-1082, 1105-1134 Pituitary Anatomy • Anterior pituitary – Pars distalis (adenohypophysis) – Pars intermedia – Pars tuberalis • Posterior pituitary (neurohypophysis, pars nervosa) • Stalk Histogenesis • Anterior pituitary (adenohypophysis) – Arises from invagination of Rathke’s pouch – Residual small cystic epithelial lined remnants are common at interface with posterior pituitary • Posterior pituitary (neurohypophysis) – Composed of nerve fibers (arising in hypothalamic nuclei), axon terminals and stromal cells Anencephaly Area cerebrovasculosa + anterior pituitary Adenohypophysis Cell type predominance and distribution Neurohypophysis • Composed of nerve fibers, few astrocytes • Herring bodies – eosinophilic intracellular secretory material Types and sources of neoplasm that can affect the pituitary gland Adenohypophysis Cell Type Hormone Stain Somatotroph Growth Hormone (GH) Mammosomatotroph GH, Prolactin (PRL) Lactotroph -

A Rapid and Easy Method for Multiple Endocrine Neoplasia Type 1 Mutation Detection Using Conformation-Sensitive Gel Electrophoresis
4600/190J Hum Genet (2002) 47:190–195 N. Matsuda et al.: © Jpn EGF Soc receptor Hum Genet and osteoblastic and Springer-Verlag differentiation 2002 ORIGINAL ARTICLE Arancha Cebrián · Sergio Ruíz-Llorente · Alberto Cascón Ana Osorio · Beatriz Martínez-Delgado · Javier Benítez Mercedes Robledo A rapid and easy method for multiple endocrine neoplasia type 1 mutation detection using conformation-sensitive gel electrophoresis Received: November 29, 2001 / Accepted: January 28, 2002 Abstract Until now, the study of the multiple endocrine individuals may also show other complex lesions such as neoplasia type 1 (MEN1) gene in patients suspected of neuroendocrine tumors (carcinoids), secreting or non- having the disease was expensive and laborious due to the secreting adrenal tumors, paraganglioma, thyroid adenoma, large size of the gene. We have optimized the conformation- or lipoma (Lips et al. 1984; Raue and Zink 1992; Trump et sensitive gel electrophoresis (CSGE) technique to analyze al. 1996). MEN1 is known to have very high penetrance, by four rather simple multiplex PCR reactions, and a single about 98.8% by the age of 53 (Trump et al. 1996). The electrophoresis run, the entire coding region of the MEN1 MEN1 gene is a tumor-suppressor gene that contains ten gene, plus the exon–intron boundaries. This improvement exons (with the first exon untranslated) and extends across of the CSGE technique was confirmed as an effective proce- 9kb. It encodes for a product of 610 amino acids named dure for screening for the MEN1 gene by detecting ten menin (Chandrasekharappa et al. 1997) that has been previously known MEN1 gene mutations and four polymor- identified as a nuclear protein, suggesting possible roles as a phisms. -

Glucagonoma and Pseudoglucagonoma Syndrome
JOP. J Pancreas (Online) 2004; 5(4):179-185. ORIGINAL ARTICLE Glucagonoma and Pseudoglucagonoma Syndrome Miguel Echenique-Elizondo1, Ana Tuneu Valls2, José Luis Elorza Orúe2, Ignacio Martinez de Lizarduy3, Javier Ibáñez Aguirre4 1Department of Surgery, Basque Country University; 2Department of Dermatology, Donostia Hospital; 3Department of Dermatology Hospital de Basurto; 4Department of Surgery, Zumárraga Hospital. San Sebastián, Spain ABSTRACT Discussion Necrolytic migratory erythema was the key diagnosis in all cases. Surgery Context Glucagonoma syndrome may present was intended to be curative. The follow-up either associated with a pancreatic neoplasm was of 8, 37 and 57 months in the cases of which secretes glucagon or as a pseudo- true glucagonoma syndrome. glucagonoma associated with other diseases. It is extremely infrequent but well-known Conclusions A real prevalence of with a current prevalence estimated at glucagonoma syndrome could be greater than 1/20,000,000. currently estimated. In our series, it was 13.5/20,000,000. Pseudoglucagonoma Design A retrospective review of syndrome remains a rarity. glucagonoma and pseudoglucagonoma cases observed between January 1998 and December 2003 in three hospitals. INTRODUCTION Patients Five cases: 3 with a demonstrable First described by Becker et al. in 1942 [1], glucagon-secreting tumor and 2 cases without glucagonoma syndrome is a very infrequent, an associated neoplasm. although well-known, disease. It is characterized by the existence of a glucagons- Main outcome measures Age, sex, initial secreting neoplasm associated with diagnosis, associated symptoms, and hyperglucagonemia, necrolytic migratory pathology were analyzed as were procedures erythema (NME), diabetes mellitus, hypo- employed in diagnosis, imaging studies, aminoacidemia, cheilitis, normocytic anemia, laboratory data, surgery and follow-up. -
Pancreatic Glucagonoma Metastasising to the Right Ovary Five Years After Initial Surgery: a Case Report
JOP. J Pancreas (Online) 2013 Sep 10; 14(5):510-514. CASE REPORT Pancreatic Glucagonoma Metastasising to the Right Ovary Five Years after Initial Surgery: A Case Report David Graham Watt 1, Sanjay Pandanaboyana 4, Charles Simon Herrington 2, Iain S Tait 3 1General Surgery, 2Department of Pathology, and 3Hepatobiliary and Pancreatic Surgery, Ninewells Hospital and Medical School. Dundee, Scotland, United Kingdom. 4Hepatobiliary and Transplant Surgery, St James University Hospital. Leeds, West Yorkshire, United Kingdom ABSTRACT Context Glucagonomas of the pancreas are neuroendocrine tumours (NETs) that arise from well-differentiated neuroendocrine cells within the pancreatic islets. They are considered to be aggressive NETs and often have metastases at initial presentation. In contrast localised glucagonoma without metastatic spread may have prolonged disease free survival with radical resectional surgery. Case report The authors present a case of a glucagonoma that initially presented with classical necrolytic migratory erythema and a large solitary mass in the body and tail of the pancreas that was surgically resected. Five years after surgery the patient presented with increased serum glucagon levels and a mass in the right ovary. Pathology of the resected ovary after oophorectomy identified this as an isolated metastatic glucagonoma. Conclusion Glucagonoma is a rare pancreatic NET that has significant malignant potential. This is the first case of a pancreatic glucagonoma metastasising to the ovary 5 years after radical distal pancreatosplenectomy. INTRODUCTION [3] and has an incidence of 1 in 20,000,000 per year [4]. Pancreatic neuroendocrine tumours (NETs) are rare tumours of the pancreatic islet cells. NETs arise The authors present a case of pancreatic from mature endocrine cells in the pancreas or glucagonoma localised to the body and tail of the multi-potent stem cells and express chromogranin pancreas that was resected in 2007 by laparoscopic A, synaptophysin and/or neuron-specific enolase.