Adopted Regulation of the State Board of Health Lcb
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table of Contents
ANTICANCER RESEARCH International Journal of Cancer Research and Treatment ISSN: 0250-7005 Volume 32, Number 4, April 2012 Contents Experimental Studies * Review: Multiple Associations Between a Broad Spectrum of Autoimmune Diseases, Chronic Inflammatory Diseases and Cancer. A.L. FRANKS, J.E. SLANSKY (Aurora, CO, USA)............................................ 1119 Varicella Zoster Virus Infection of Malignant Glioma Cell Cultures: A New Candidate for Oncolytic Virotherapy? H. LESKE, R. HAASE, F. RESTLE, C. SCHICHOR, V. ALBRECHT, M.G. VIZOSO PINTO, J.C. TONN, A. BAIKER, N. THON (Munich; Oberschleissheim, Germany; Zurich, Switzerland) .................................... 1137 Correlation between Adenovirus-neutralizing Antibody Titer and Adenovirus Vector-mediated Transduction Efficiency Following Intratumoral Injection. K. TOMITA, F. SAKURAI, M. TACHIBANA, H. MIZUGUCHI (Osaka, Japan) .......................................................................................................... 1145 Reduction of Tumorigenicity by Placental Extracts. A.M. MARLEAU, G. MCDONALD, J. KOROPATNICK, C.-S. CHEN, D. KOOS (Huntington Beach; Santa Barbara; Loma Linda; San Diego, CA, USA; London, ON, Canada) ...................................................................................................................................... 1153 Stem Cell Markers as Predictors of Oral Cancer Invasion. A. SIU, C. LEE, D. DANG, C. LEE, D.M. RAMOS (San Francisco, CA, USA) ................................................................................................ -

Rare Presentation of Metastatic Lobular Breast Carcinoma Involving Clear Cell Renal Cell Carcinoma
Hindawi Case Reports in Oncological Medicine Volume 2020, Article ID 5315178, 5 pages https://doi.org/10.1155/2020/5315178 Case Report Rare Presentation of Metastatic Lobular Breast Carcinoma Involving Clear Cell Renal Cell Carcinoma Dayne Ashman,1 Gabriela Quiroga-Garza,1 and Daniel Lee 2 1Department of Pathology, University of Pittsburgh, 5230 Centre Avenue, Pittsburgh, PA 15232, USA 2Department of Medicine, University of Pittsburgh, 5150 Centre Avenue, Pittsburgh, PA 15232, USA Correspondence should be addressed to Daniel Lee; [email protected] Received 23 March 2020; Accepted 3 September 2020; Published 15 September 2020 Academic Editor: Raffaele Palmirotta Copyright © 2020 Dayne Ashman et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Although the first case of tumor-to-tumor metastasis was reported over a century ago, it remains a rare occurrence. We report a rare case of metastatic infiltrating lobular carcinoma involving clear cell renal cell carcinoma, as well as offer a brief literature review. 1. Introduction Microscopic examination of the biopsy specimen revealed two distinct neoplasms (Figure 3). The first neo- The phenomenon of one malignant tumor metastasizing to plasm identified demonstrated cells arranged in nests and another, unrelated, primary tumor, has been termed solid sheets with delicate vasculature. Cytologically, these “tumor-to-tumor” metastasis (TTM); it is a rare occurrence. neoplastic cells demonstrated clear cytoplasm with round To date, there have been fewer than 200 cases reported in nuclei and inconspicuous nucleoli, morphologically consis- the English literature. -

Differential Diagnosis of Ovarian Mucinous Tumours Sigurd F
Differential Diagnosis of Ovarian Mucinous Tumours Sigurd F. Lax LKH Graz II Academic Teaching Hospital of the Medical University Graz Pathology Mucinous tumours of the ovary • Primary ➢Seromucinous tumours ➢Mucinous tumours ➢Benign, borderline, malignant • Secondary (metastatic) ➢Metastases (from gastrointestinal tract) • Metastases can mimic primary ovarian tumour Mucinous tumours: General • 2nd largest group after serous tumours • Gastro-intestinal differentiation (goblet cells) • Endocervical type> seromucinous tumours • Majority is unilateral, particularly cystadenomas and borderline tumours • Bilaterality: rule out metastatic origin • Adenoma>carcinoma sequence reflected by a mixture of benign, atypical proliferating and malignant areas within the same tumour Sero-mucinous ovarian tumours • Previous endocervical type of mucinous tumor • Mixture of at least 2 cell types: mostly serous • Association with endometriosis; multifocality • Similarity with endometrioid and serous tumours, also immunophenotype • CK7, ER, WT1 positive; CK20, cdx2 negativ • Most cystadenoma and borderline tumours • Carcinomas rare and difficult to diagnose Shappel et al., 2002; Dube et al., 2005; Vang et al. 2006 Seromucinous Borderline Tumour ER WT1 Seromucinous carcinoma being discontinued? • Poor reproducibility: Low to modest agreement from 39% to 56% for 4 observers • Immunophenotype not unique, overlapped predominantly with endometrioid and to a lesser extent with mucinous and low-grade serous carcinoma • Molecular features overlap mostly with endometrioid -

Endocrine Tumors of the Pancreas
Friday, November 4, 2005 8:30 - 10:30 a. m. Pancreatic Tumors, Session 2 Chairman: R. Jensen, Bethesda, MD, USA 9:00 - 9:30 a. m. Working Group Session Pathology and Genetics Group leaders: J.–Y. Scoazec, Lyon, France Questions to be answered: 12 Medicine and Clinical Pathology Group leader: K. Öberg, Uppsala, Sweden Questions to be answered: 17 Surgery Group leader: B. Niederle, Vienna, Austria Questions to be answered: 11 Imaging Group leaders: S. Pauwels, Brussels, Belgium; D.J. Kwekkeboom, Rotterdam, The Netherlands Questions to be answered: 4 Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging ENETS Guidelines Neuroendocrinology 2004;80:394–424 Endocrine Tumors of the Pancreas - gastrinoma Epidemiology The incidence of clinically detected tumours has been reported to be 4-12 per million inhabitants, which is much lower than what is reported from autopsy series (about 1%) (5,13). Clinicopathological staging (12, 14, 15) Well-differentiated tumours are the large majority of which the two largest fractions are insulinomas (about 40% of cases) and non-functioning tumours (30-35%). When confined to the pancreas, non-angioinvasive, <2 cm in size, with <2 mitoses per 10 high power field (HPF) and <2% Ki-67 proliferation index are classified as of benign behaviour (WHO group 1) and, with the notable exception of insulinomas, are non-functioning. Tumours confined to the pancreas but > 2 cm in size, with angioinvasion and /or perineural space invasion, or >2mitoses >2cm in size, >2 mitoses per 20 HPF or >2% Ki-67 proliferation index, either non-functioning or functioning (gastrinoma, insulinoma, glucagonoma, somastatinoma or with ectopic syndromes, such as Cushing’s syndrome (ectopic ACTH syndrome), hypercaliemia (PTHrpoma) or acromegaly (GHRHoma)) still belong to the (WHO group 1) but are classified as tumours with uncertain behaviour. -

PROPOSED REGULATION of the STATE BOARD of HEALTH LCB File No. R057-16
PROPOSED REGULATION OF THE STATE BOARD OF HEALTH LCB File No. R057-16 Section 1. Chapter 457 of NAC is hereby amended by adding thereto the following provision: 1. The Division may impose an administrative penalty of $5,000 against any person or organization who is responsible for reporting information on cancer who violates the provisions of NRS 457. 230 and 457.250. 2. The Division shall give notice in the manner set forth in NAC 439.345 before imposing any administrative penalty 3. Any person or organization upon whom the Division imposes an administrative penalty pursuant to this section may appeal the action pursuant to the procedures set forth in NAC 439.300 to 439. 395, inclusive. Section 2. NAC 457.010 is here by amended to read as follows: As used in NAC 457.010 to 457.150, inclusive, unless the context otherwise requires: 1. “Cancer” has the meaning ascribed to it in NRS 457.020. 2. “Division” means the Division of Public and Behavioral Health of the Department of Health and Human Services. 3. “Health care facility” has the meaning ascribed to it in NRS 457.020. 4. “[Malignant neoplasm” means a virulent or potentially virulent tumor, regardless of the tissue of origin. [4] “Medical laboratory” has the meaning ascribed to it in NRS 652.060. 5. “Neoplasm” means a virulent or potentially virulent tumor, regardless of the tissue of origin. 6. “[Physician] Provider of health care” means a [physician] provider of health care licensed pursuant to chapter [630 or 633] 629.031 of NRS. 7. “Registry” means the office in which the Chief Medical Officer conducts the program for reporting information on cancer and maintains records containing that information. -

The Health-Related Quality of Life of Sarcoma Patients and Survivors In
Cancers 2020, 12 S1 of S7 Supplementary Materials The Health-Related Quality of Life of Sarcoma Patients and Survivors in Germany—Cross-Sectional Results of A Nationwide Observational Study (PROSa) Martin Eichler, Leopold Hentschel, Stephan Richter, Peter Hohenberger, Bernd Kasper, Dimosthenis Andreou, Daniel Pink, Jens Jakob, Susanne Singer, Robert Grützmann, Stephen Fung, Eva Wardelmann, Karin Arndt, Vitali Heidt, Christine Hofbauer, Marius Fried, Verena I. Gaidzik, Karl Verpoort, Marit Ahrens, Jürgen Weitz, Klaus-Dieter Schaser, Martin Bornhäuser, Jochen Schmitt, Markus K. Schuler and the PROSa study group Includes Entities We included sarcomas according to the following WHO classification. - Fletcher CDM, World Health Organization, International Agency for Research on Cancer, editors. WHO classification of tumours of soft tissue and bone. 4th ed. Lyon: IARC Press; 2013. 468 p. (World Health Organization classification of tumours). - Kurman RJ, International Agency for Research on Cancer, World Health Organization, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: International Agency for Research on Cancer; 2014. 307 p. (World Health Organization classification of tumours). - Humphrey PA, Moch H, Cubilla AL, Ulbright TM, Reuter VE. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part B: Prostate and Bladder Tumours. Eur Urol. 2016 Jul;70(1):106–19. - World Health Organization, Swerdlow SH, International Agency for Research on Cancer, editors. WHO classification of tumours of haematopoietic and lymphoid tissues: [... reflects the views of a working group that convened for an Editorial and Consensus Conference at the International Agency for Research on Cancer (IARC), Lyon, October 25 - 27, 2007]. 4. ed. -

A Case of Krukenberg Tumor Metastasized from Colon Cancer In
A case of Krukenberg tumor metastasized from colon cancer in pregnancy Oztas E, Ozler S, Ersoy AO, Turker M, Zengın NI, Caglar AT, Danisman N Zekai Tahir Burak Women's Health Education and Research Hospital, Ankara, Turkey Objective Krukenberg tumor refers to gastrointestinal cancer metastatic to the ovaries and has an extremely poor prognosis, with a 5-year survival rate ranging from 12% to 23. 4%. Gastric cancer has been reported as the most frequent primary source of Krukenberg tumor; however, tumors of the colon, appendix, breast, lung, and pancreas have also been reported to metastasize into the ovaries. Krukenberg tumors are usually seen in the fifth decade of life, with an average age of 45 years and cases diagnosed during pregnancy are thus extremely rare. Methods We report a case of a Krukenberg tumor secondary to colon carcinoma in a pregnant woman with acute pelvic pain. The prenatal diagnosis was made at 17 weeks’ gestation. Results A 27-year-old, primigravida with a semisolid right adnexial mass was presented with acute pelvic pain at 17 weeks’ gestation. Ultrasonography revealed a semisolid right adnexial mass of 140×130 mm and ascites, as well as a single live fetus compatible for gestational age. The abdomen was tense, tender and distended so exploratory laparotomy was performed with the suspicion of ovarian torsion. During the operation, ascites, enlarged right ovary with the presence of a necrotic tumor measuring 160×140 mm causing ovarian torsion and omental metastasis were seen. Unilateral oophorectomy and omentectomy were then performed. Histopathological examination of the specimen revealed adenocarcinoma metastasis to the ovary and the omentum probably originating from a primary gastrointestinal carcinoma (Figure-1). -
C O N F E R E N C E 7 18 October 2017
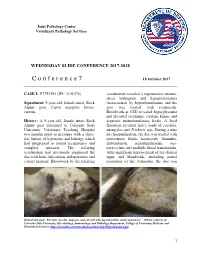
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2017-2018 C o n f e r e n c e 7 18 October 2017 CASE I: F1753191 (JPC 4101076). veterinarian revealed a regenerative anemia, stress leukogram and hypoproteinemia Signalment: 9-year-old, female intact, Rock characterized by hypoalbuminemia and the Alpine goat, Capra aegagrus hircus, goat was treated with ivermectin. caprine. Bloodwork at CSU revealed hyperglycemia and elevated creatinine, creatine kinase and History: A 9-year-old, female intact Rock aspartate aminotransferase levels. A fecal Alpine goat presented to Colorado State floatation revealed heavy loads of coccidia, University Veterinary Teaching Hospital strongyles and Trichuris spp. During a nine two months prior to necropsy with a three- day hospitalization, the doe was treated with day history of hyporexia and lethargy which intravenous fluids, kaopectate, thiamine, had progressed to lateral recumbency and fenbendazole, sulfadimethoxine, oxy- complete anorexia. The referring tetracycline and multiple blood transfusions. veterinarian had previously diagnosed the After significant improvement of her clinical doe with louse infestation, endoparasites and signs and bloodwork, including partial a heart murmur. Bloodwork by the referring resolution of the dermatitis, the doe was Haired skin goat. The skin was dry, alopecia, and covered with hyperkeratotic crusts and ulcers. (Photo courtesy of: Colorado State University, Microbiology, Immunology, and Pathology Department, College of Veterinary Medicine and Biomedical Sciences, http://csucvmbs.colostate.edu/academics/mip/Pages/default.aspx) 1 discharged. exfoliating epithelial crusts which were often tangled within scant remaining hairs. Two months later, the goat presented with a This lesion most severely affected the skin one month history of progressive scaling and over the epaxials, the ventral abdomen and ulceration over the withers, dew claws, and teats, coronary bands and dew claws. -
Malignant Transformation of Liver Cysts Into Cholangiocarcinoma During Follow-Up: Potential Dangers of Liver Cysts
Malignant Transformation of Liver Cysts Into Cholangiocarcinoma During Follow-up: Potential Dangers of Liver Cysts Fu-sheng Liu Wuhan University Second Clinical Hospital: Wuhan University Zhongnan Hospital https://orcid.org/0000-0003-1175-5209 Ke-lu Li Department of Pathology, Wuhan University Zhongnan Hospital Yue-ming He Department of Hepatobiliary&Pancreatic Surgery, Zhongnan Hospital of Wuhan University Zhong-lin Zhang Department of Hepatobiliary&Pancreatic Surgery, Zhongnan Hospital of Wuhan University Yu-feng Yuan Department of Hepatobiliary&Pancreatic Surgery, Zhongnan Hospital of Wuhan University Hai-tao Wang ( [email protected] ) Wuhan University Second Clinical Hospital: Wuhan University Zhongnan Hospital Case Report Keywords: Liver cysts, intrahepatic cholangiocarcinoma, malignant transformation Posted Date: July 9th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-684869/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/12 Abstract Background: The liver cyst is a common disease in hepatobiliary surgery. Most patients have no apparent symptoms and are usually diagnosed accidentally during imaging examinations. The vast majority of patients with liver cysts follow a benign course, with very few serious complications and rare reports of malignant changes. Case Presentation: We present two cases of liver cysts that evolved into intrahepatic tumors during the follow-up process. The rst patient had undergone a fenestration and drainage operation for the liver cyst, and the cancer was found at the cyst’s position in the third year after the procedure. Microscopically, bile duct cells formed the cyst wall. Tumor cells can be seen on the cyst wall and its surroundings to form adenoid structures of different sizes, shapes, and irregular arrangements, some of which are arranged in clusters. -

Life Expectancy and Incidence of Malignant Disease Iv
LIFE EXPECTANCY AND INCIDENCE OF MALIGNANT DISEASE IV. CARCINOMAOF THE GENITO-URINARYTRACT CLAUDE E. WELCH,' M.D., AND IRA T. NATHANSON,? MS., M.D. (Front the Collis P. Huntington Memorial Hospital of Harvard University, and the Pondville State Hospitul, Wre~ztham,Mass.) In previous communications the life expectancy of patients with cancer of the breast (I), oral cavity (2), and gastro-intestinal tract (3) has been discussed. In the present paper the life expectancy of patients with carci- noma of the genito-urinary tract will be considered. The discussion will include cancer of the vulva, vagina, cervix and fundus uteri, ovary, penis, testicle, prostate, bladder, and kidney. All cases of cancer of these organs admitted to the Collis P. Huntington Memorial and Pondville Hospitals in the years 1912-1933 have been reviewed personally. It must again be stressed that these hospitals are organized strictly for the care of cancer patients. All those with cancer that apply are admitted for treatment; many of them have only terminal care. Only those cases in which a definite history of the date of onset could not be determined or in which the diagnosis was uncertain have been omitted in the present study. In compiling statistics on age and sex incidence all cases entering the hospitals before Jan. 1, 1936, have been included. The method of calculation of the life expectancy curves was fully described in the first paper (1). No at- tempt to evaluate the number of five-year survivals has been made, since many of the patients did not receive their initial treatment in these hospitals. -

Soft Tissue Sarcoma Classifications
Soft Tissue Sarcoma Classifications Contents: 1. Introduction 2. Summary of SSCRG’s decisions 3. Issue by issue summary of discussions A: List of codes to be included as Soft Tissue Sarcomas B: Full list of codes discussed with decisions C: Sarcomas of neither bone nor soft tissue D: Classifications by other organisations 1. Introduction We live in an age when it is increasingly important to have ‘key facts’ and ‘headline messages’. The national registry for bone and soft tissue sarcoma want to be able to produce high level factsheets for the general public with statements such as ‘There are 2000 soft tissue sarcomas annually in England’ or ‘Survival for soft tissue sarcomas is (eg) 75%’ It is not possible to write factsheets and data briefings like this, without a shared understanding from the SSCRG about which sarcomas we wish to include in our headline statistics. The registry accepts that soft tissue sarcomas are a very complex and heterogeneous group of cancers which do not easily reduce to headline figures. We will still strive to collect all data from cancer registries about anything that is ‘like a sarcoma’. We will also produce focussed data briefings on sites such as dermatofibrosarcomas and Kaposi’s sarcomas – the aim is not to forget any sites we exclude! The majority of soft tissue sarcomas have proved fairly uncontroversial in discussions with individual members of the SSCRG, but there were 7 particular issues it was necessary to make a group decision on. This paper records the decisions made and the rationale behind these decisions. 2. Summary of SSCRG’s decisions: Include all tumours with morphology codes as listed in Appendix A for any cancer site except C40 and C41 (bone). -

Human Anatomy As Related to Tumor Formation Book Four
SEER Program Self Instructional Manual for Cancer Registrars Human Anatomy as Related to Tumor Formation Book Four Second Edition U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutesof Health SEER PROGRAM SELF-INSTRUCTIONAL MANUAL FOR CANCER REGISTRARS Book 4 - Human Anatomy as Related to Tumor Formation Second Edition Prepared by: SEER Program Cancer Statistics Branch National Cancer Institute Editor in Chief: Evelyn M. Shambaugh, M.A., CTR Cancer Statistics Branch National Cancer Institute Assisted by Self-Instructional Manual Committee: Dr. Robert F. Ryan, Emeritus Professor of Surgery Tulane University School of Medicine New Orleans, Louisiana Mildred A. Weiss Los Angeles, California Mary A. Kruse Bethesda, Maryland Jean Cicero, ART, CTR Health Data Systems Professional Services Riverdale, Maryland Pat Kenny Medical Illustrator for Division of Research Services National Institutes of Health CONTENTS BOOK 4: HUMAN ANATOMY AS RELATED TO TUMOR FORMATION Page Section A--Objectives and Content of Book 4 ............................... 1 Section B--Terms Used to Indicate Body Location and Position .................. 5 Section C--The Integumentary System ..................................... 19 Section D--The Lymphatic System ....................................... 51 Section E--The Cardiovascular System ..................................... 97 Section F--The Respiratory System ....................................... 129 Section G--The Digestive System ......................................... 163 Section