Mutational and Gross Deletion Study of the MEN1 Gene and Correlation With
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Endocrine Tumors of the Pancreas
Friday, November 4, 2005 8:30 - 10:30 a. m. Pancreatic Tumors, Session 2 Chairman: R. Jensen, Bethesda, MD, USA 9:00 - 9:30 a. m. Working Group Session Pathology and Genetics Group leaders: J.–Y. Scoazec, Lyon, France Questions to be answered: 12 Medicine and Clinical Pathology Group leader: K. Öberg, Uppsala, Sweden Questions to be answered: 17 Surgery Group leader: B. Niederle, Vienna, Austria Questions to be answered: 11 Imaging Group leaders: S. Pauwels, Brussels, Belgium; D.J. Kwekkeboom, Rotterdam, The Netherlands Questions to be answered: 4 Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging ENETS Guidelines Neuroendocrinology 2004;80:394–424 Endocrine Tumors of the Pancreas - gastrinoma Epidemiology The incidence of clinically detected tumours has been reported to be 4-12 per million inhabitants, which is much lower than what is reported from autopsy series (about 1%) (5,13). Clinicopathological staging (12, 14, 15) Well-differentiated tumours are the large majority of which the two largest fractions are insulinomas (about 40% of cases) and non-functioning tumours (30-35%). When confined to the pancreas, non-angioinvasive, <2 cm in size, with <2 mitoses per 10 high power field (HPF) and <2% Ki-67 proliferation index are classified as of benign behaviour (WHO group 1) and, with the notable exception of insulinomas, are non-functioning. Tumours confined to the pancreas but > 2 cm in size, with angioinvasion and /or perineural space invasion, or >2mitoses >2cm in size, >2 mitoses per 20 HPF or >2% Ki-67 proliferation index, either non-functioning or functioning (gastrinoma, insulinoma, glucagonoma, somastatinoma or with ectopic syndromes, such as Cushing’s syndrome (ectopic ACTH syndrome), hypercaliemia (PTHrpoma) or acromegaly (GHRHoma)) still belong to the (WHO group 1) but are classified as tumours with uncertain behaviour. -

TERT Promoter Mutations Occur Frequently in Gliomas and a Subset of Tumors Derived from Cells with Low Rates of Self-Renewal
TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal Patrick J. Killelaa,1, Zachary J. Reitmana,1, Yuchen Jiaob,1, Chetan Bettegowdab,c,1, Nishant Agrawalb,d, Luis A. Diaz, Jr.b, Allan H. Friedmana, Henry Friedmana, Gary L. Galliac,d, Beppino C. Giovanellae, Arthur P. Grollmanf, Tong-Chuan Heg, Yiping Hea, Ralph H. Hrubanh, George I. Jalloc, Nils Mandahli, Alan K. Meekerh,m, Fredrik Mertensi, George J. Nettoh,l, B. Ahmed Rasheeda, Gregory J. Rigginsc, Thomas A. Rosenquistf, Mark Schiffmanj, Ie-Ming Shihh, Dan Theodorescuk, Michael S. Torbensonh, Victor E. Velculescub, Tian-Li Wangh, Nicolas Wentzensenj, Laura D. Woodh, Ming Zhangb, Roger E. McLendona, Darell D. Bignera, Kenneth W. Kinzlerb, Bert Vogelsteinb,2, Nickolas Papadopoulosb, and Hai Yana,2 aThe Preston Robert Tisch Brain Tumor Center at Duke, Pediatric Brain Tumor Foundation Institute at Duke, and Department of Pathology, Duke University Medical Center, Durham, NC 27710; bLudwig Center for Cancer Genetics and Howard Hughes Medical Institutions, Johns Hopkins Kimmel Cancer Center, Johns Hopkins Medical Institutions, Baltimore, MD 21231; Departments of cNeurosurgery, dOtolaryngology—Head and Neck Surgery, hPathology, lUrology, and mOncology, Johns Hopkins University School of Medicine, Baltimore, MD 21231; eChristus Stehlin Foundation for Cancer Research, Houston, TX 77025; fDepartment of Pharmacological Sciences, Stony Brook University, Stony Brook, NY 11794; gMolecular Oncology Laboratory, Department of Orthopaedic -
C O N F E R E N C E 7 18 October 2017
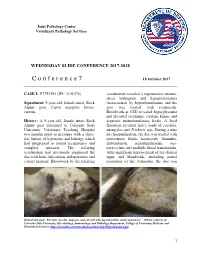
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2017-2018 C o n f e r e n c e 7 18 October 2017 CASE I: F1753191 (JPC 4101076). veterinarian revealed a regenerative anemia, stress leukogram and hypoproteinemia Signalment: 9-year-old, female intact, Rock characterized by hypoalbuminemia and the Alpine goat, Capra aegagrus hircus, goat was treated with ivermectin. caprine. Bloodwork at CSU revealed hyperglycemia and elevated creatinine, creatine kinase and History: A 9-year-old, female intact Rock aspartate aminotransferase levels. A fecal Alpine goat presented to Colorado State floatation revealed heavy loads of coccidia, University Veterinary Teaching Hospital strongyles and Trichuris spp. During a nine two months prior to necropsy with a three- day hospitalization, the doe was treated with day history of hyporexia and lethargy which intravenous fluids, kaopectate, thiamine, had progressed to lateral recumbency and fenbendazole, sulfadimethoxine, oxy- complete anorexia. The referring tetracycline and multiple blood transfusions. veterinarian had previously diagnosed the After significant improvement of her clinical doe with louse infestation, endoparasites and signs and bloodwork, including partial a heart murmur. Bloodwork by the referring resolution of the dermatitis, the doe was Haired skin goat. The skin was dry, alopecia, and covered with hyperkeratotic crusts and ulcers. (Photo courtesy of: Colorado State University, Microbiology, Immunology, and Pathology Department, College of Veterinary Medicine and Biomedical Sciences, http://csucvmbs.colostate.edu/academics/mip/Pages/default.aspx) 1 discharged. exfoliating epithelial crusts which were often tangled within scant remaining hairs. Two months later, the goat presented with a This lesion most severely affected the skin one month history of progressive scaling and over the epaxials, the ventral abdomen and ulceration over the withers, dew claws, and teats, coronary bands and dew claws. -

SUPPLEMENTARY NOTE Co-Activation of GR and NFKB
SUPPLEMENTARY NOTE Co-activation of GR and NFKB alters the repertoire of their binding sites and target genes. Nagesha A.S. Rao1*, Melysia T. McCalman1,*, Panagiotis Moulos2,4, Kees-Jan Francoijs1, 2 2 3 3,5 Aristotelis Chatziioannou , Fragiskos N. Kolisis , Michael N. Alexis , Dimitra J. Mitsiou and 1,5 Hendrik G. Stunnenberg 1Department of Molecular Biology, Radboud University Nijmegen, the Netherlands 2Metabolic Engineering and Bioinformatics Group, Institute of Biological Research and Biotechnology, National Hellenic Research Foundation, Athens, Greece 3Molecular Endocrinology Programme, Institute of Biological Research and Biotechnology, National Hellenic Research Foundation, Greece 4These authors contributed equally to this work 5 Corresponding authors E-MAIL: [email protected] ; TEL: +31-24-3610524; FAX: +31-24-3610520 E-MAIL: [email protected] ; TEL: +30-210-7273741; FAX: +30-210-7273677 Running title: Global GR and NFKB crosstalk Keywords: GR, p65, genome-wide, binding sites, crosstalk SUPPLEMENTARY FIGURES/FIGURE LEGENDS AND SUPPLEMENTARY TABLES 1 Rao118042_Supplementary Fig. 1 A Primary transcript Mature mRNA TNF/DMSO TNF/DMSO 8 12 r=0.74, p< 0.001 r=0.61, p< 0.001 ) 2 ) 10 2 6 8 4 6 4 2 2 0 Fold change (mRNA) (log Fold change (primRNA) (log 0 −2 −2 −2 0 2 4 −2 0 2 4 Fold change (RNAPII) (log2) Fold change (RNAPII) (log2) B chr5: chrX: 56 _ 104 _ DMSO DMSO 1 _ 1 _ 56 _ 104 _ TA TA 1 _ 1 _ 56 _ 104 _ TNF TNF Cluster 1 1 _ Cluster 2 1 _ 56 _ 104 _ TA+TNF TA+TNF 1 _ 1 _ CCNB1 TSC22D3 chr20: chr17: 25 _ 33 _ DMSO DMSO 1 _ 1 _ 25 _ 33 _ TA TA 1 _ 1 _ 25 _ 33 _ TNF TNF Cluster 3 1 _ Cluster 4 1 _ 25 _ 33 _ TA+TNF TA+TNF 1 _ 1 _ GPCPD1 CCL2 chr6: chr22: 77 _ 35 _ DMSO DMSO 1 _ 77 _ 1 _ 35 _ TA TA 1 _ 1 _ 77 _ 35 _ TNF Cluster 5 Cluster 6 TNF 1 _ 1 _ 77 _ 35 _ TA+TNF TA+TNF 1 _ 1 _ TNFAIP3 DGCR6 2 Supplementary Figure 1. -

Production of the a Subunit of Guanine Nucleotide-Binding Protein GO by Neuroendocrine Tumors1
[CANCER RESEARCH 47, 5800-5805, November 1, 1987] Production of the a Subunit of Guanine Nucleotide-binding Protein GO by Neuroendocrine Tumors1 Kanefusa Kato,2 Tomiko Asano, Nobuko Kamiya, Hajime Haimoto, Syun Hosoda, Akio Nagasaka, Yutaka Ariyoshi, and Yukio Ishiguro Department of Biochemistry ¡K.K„T.A., N. K.], Institute for Developmental Research, Aichi Prefectural Colony, Kasugai, Aichi 480-03; Laboratory of Pathology ¡H.H., S. H.] and Department of Internal Medicine [Y, A.], Aichi Cancer Center, Chikusa-ku, Nagoya 464; Department of Internal Medicine [A. N.J. Fujita-Gakuen Health University, School of Medicine, Toyoake, Aichi 470-11; and Department of Surgery [Y. IJ, Nagoya University School of Medicine, Showa-ku, Nagoya 466, Japan ABSTRACT is localized exclusively in the nervous tissues and some endo crine cells in pancreas, pituitary, thyroid, and adrenal,4 which We have found that neuroendocrine tumors (including neuroblastoma, belong to a family designated as APUD (amine precursor ganglioneuroma, gut carcinoid, pheochromocytoma, medullary thyroid uptake and decarboxylation) or diffuse neuroendocrine system carcinoma, insulinoma, glucagonoma, prolactinoma, carotid body tumor, (10). We describe here the presence of G0«in tumors derived and small cell lung carcinoma) produce considerable amounts (about 1000-80,000 ng/g tissue) of the a subunit of guanine nucleotide-binding from the above mentioned neuroendocrine cells and in sera of protein, G0 (Goa), whereas nonneuroendocrine tumors contain less than patients with neuroblastoma, and evaluate G0a for the appli 300 ng of Goa/g tissue. Goat in the neuroendocrine tumors was present cation to clinical and immunohistochemical diagnosis. both in the soluble fraction, and cholate-extractable membrane-bound fraction of tissues. -

Multiple Endocrine Neoplasia Type 1 (MEN1)
Lab Management Guidelines v2.0.2019 Multiple Endocrine Neoplasia Type 1 (MEN1) MOL.TS.285.A v2.0.2019 Introduction Multiple Endocrine Neoplasia Type 1 (MEN1) is addressed by this guideline. Procedures addressed The inclusion of any procedure code in this table does not imply that the code is under management or requires prior authorization. Refer to the specific Health Plan's procedure code list for management requirements. Procedures addressed by this Procedure codes guideline MEN1 Known Familial Mutation Analysis 81403 MEN1 Deletion/Duplication Analysis 81404 MEN1 Full Gene Sequencing 81405 What is Multiple Endocrine Neoplasia Type 1 Definition Multiple Endocrine Neoplasia Type 1 (MEN1) is an inherited form of tumor predisposition characterized by multiple tumors of the endocrine system. Incidence or Prevalence MEN1 has a prevalence of 1/10,000 to 1/100,000 individuals.1 Symptoms The presenting symptom in 90% of individuals with MEN1 is primary hyperparathyroidism (PHPT). Parathyroid tumors cause overproduction of parathyroid hormone which leads to hypercalcemia. The average age of onset is 20-25 years. Parathyroid carcinomas are rare in individuals with MEN1.2,3,4 Pituitary tumors are seen in 30-40% of individuals and are the first clinical manifestation in 10% of familial cases and 25% of simplex cases. Tumors are typically solitary and there is no increased prevalence of pituitary carcinoma in individuals with MEN1.2,5 © eviCore healthcare. All Rights Reserved. 1 of 9 400 Buckwalter Place Boulevard, Bluffton, SC 29910 (800) 918-8924 www.eviCore.com Lab Management Guidelines v2.0.2019 Prolactinomas are the most commonly seen pituitary subtype and account for 60% of pituitary adenomas. -

Rising Incidence of Neuroendocrine Tumors
Rising Incidence of Neuroendocrine Tumors Dasari V, Yao J, et al. JAMA Oncology 2017 S L I D E 1 Overview Pancreatic Neuroendocrine Tumors • Tumors which arise from endocrine cells of the pancreas • 5.6 cases per million – 3% of pancreatic tumors • Median age at diagnosis 60 years • More indolent course compared to adenocarcinoma – 10-year overall survival 40% • Usually sporadic but can be associated with hereditary syndromes – Core genetic pathways altered in sporadic cases • DNA damage repair (MUTYH) Chromatin remodeling (MEN1) • Telomere maintenance (MEN1, DAXX, ATRX) mTOR signaling – Hereditary: 17% of patients with germline mutation Li X, Wang C, et al. Cancer Med 2018 Scarpa A, Grimond S, et al. NatureS L I2017 D E 2 Pathology Classification European American Joint World Health Organization Neuroendocrine Committee on Cancer (WHO) Tumor Society (AJCC) (ENETS) Grade Ki-67 Mitotic rt TNM TNM T1: limit to pancreas, <2 cm T1: limit to pancreas, ≦2 cm T2: limit to pancreas, 2-4 cm T2: >limit to pancreas, 2 cm T3: limit to pancreas, >4 cm, T3: beyond pancreas, no celiac or Low ≤2% <2 invades duodenum, bile duct SMA T4: beyond pancreas, invasion involvement adjacent organs or vessels T4: involves celiac or SMA N0: node negative No: node negative Intermed 3-20% 2-20 N1: node positive N1: node positive M0: no metastases M0: no metastases High >20% >20 M1: metastases M1: metastases S L I D E 3 Classification Based on Functionality • Nonfunctioning tumors – No clinical symptoms (can still produce hormone) – Accounts for 40% of tumors – 60-85% -

Reversal of Preexisting Hyperglycemia in Diabetic Mice by Acute Deletion of the Men1 Gene
Reversal of preexisting hyperglycemia in diabetic mice by acute deletion of the Men1 gene Yuqing Yanga, Buddha Gurunga, Ting Wub, Haoren Wanga, Doris A. Stoffersc,d, and Xianxin Huaa,d,1 aAbramson Family Cancer Research Institute, Department of Cancer Biology, Abramson Cancer Center, cDepartment of Medicine, and dInstitute for Diabetes, Obesity, and Metabolism, University of Pennsylvania, Philadelphia, PA 19104; and bDepartment of Basic Medical Sciences, Medical College, Xiamen University, Xiamen 361005, China Edited by Arnold J. Levine, Institute for Advanced Study, Princeton, NJ, and approved September 28, 2010 (received for review August 18, 2010) A hallmark of diabetes is an absolute or relative reduction in the Men1 excision differently from normal β cells. Thus, it is im- number of functional β cells. Therapies that could increase the num- portant to determine whether Men1 excision actually ameliorates ber of endogenous β cells under diabetic conditions would be desir- or reverses hyperglycemia in diabetic mice. able. Prevalent gene targeting mouse models for assessing β-cell How menin regulates β-cell proliferation is not well understood. proliferation and diabetes pathogenesis only address whether de- Although menin has been shown to be crucial for expression of letion of a gene prevents the development of diabetes. Models cyclin-dependent kinase inhibitor p18ink4c (p18 hereafter) and p27 testing whether acute excision of a single gene can ameliorate or in islets (10, 11) and liver cells (12), Men1 excision does not affect reverse preexisting hyperglycemia in established diabetes remain to liver cell proliferation (7). These findings raise the possibility that be explored, which could directly validate the effect of gene exci- menin may also regulate β cell proliferation through effectors sion on treating diabetes. -

Preclinical Cushing's Syndrome Resulting from Adrenal Black
Endocrine Journal 2007, 54 (4), 543–551 Preclinical Cushing’s Syndrome Resulting from Adrenal Black Adenoma Diagnosed with Diabetic Ketoacidosis TOSHIO KAHARA, CHIKASHI SETO*, AKIO UCHIYAMA**, DAISUKE USUDA, HIROSHI AKAHORI, EIJI TAJIKA*, ATSUO MIWA**, RIKA USUDA, TAKASHI SUZUKI*** AND HIRONOBU SASANO*** Department of Internal Medicine, Toyama Prefectural Central Hospital, 2-2-78 Nishinagae, Toyama 930-8550, Japan *Department of Urology, Toyama Prefectural Central Hospital, 2-2-78 Nishinagae, Toyama 930-8550, Japan **Department of Pathology, Toyama Prefectural Central Hospital, 2-2-78 Nishinagae, Toyama 930-8550, Japan ***Department of Pathology, Tohoku University School of Medicine, 2-1 Seiryo-machi, Aoba-ku, Sendai 980-8575, Japan Abstract. A right adrenal tumor was incidentally discovered on abdominal computed tomography performed on a 53- year-old Japanese man, who had been hospitalized with diabetic ketoacidosis. Normal values were obtained for adrenal hormones in the morning after an overnight fast and urinary cortisol excretion after treatment of diabetic ketoacidosis with insulin. However, overnight dexamethasone administration with 1 mg or 8 mg did not completely suppress serum cortisol levels. There were no remarkable physical findings related to Cushing’s syndrome. The patient was diagnosed as having preclinical Cushing’s syndrome (PCS). Histological examination of the adrenalectomy specimen demonstrated adrenal black adenoma. Blood glucose levels subsequently improved after adrenalectomy, and the patient never developed adrenal insufficiency after hydrocortisone withdrawal. The patient was treated with diet therapy alone, and maintained good glycemic control. However, the patient still showed a diabetic pattern in an oral glucose tolerance test. It seems that the existence of PCS in addition to the underlying type 2 diabetes mellitus contributed to aggravation of blood glucose levels. -

Twenty Years of Menin: Emerging Opportunities for Restoration of Transcriptional Regulation in MEN1
2410 K M A Dreijerink et al. Molecular mechanism of MEN1 24:10 T135–T145 Thematic Review Twenty years of menin: emerging opportunities for restoration of transcriptional regulation in MEN1 Koen M A Dreijerink1, H T Marc Timmers2 and Myles Brown3 1 Department of Endocrinology, VU University Medical Center, Amsterdam, The Netherlands Correspondence 2 German Cancer Consortium (DKTK) partner site Freiburg, German Cancer Research Center (DKFZ) and Department should be addressed of Urology, Medical Center-University of Freiburg, Freiburg, Germany to M Brown 3 Department of Medical Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts, USA Email [email protected] Abstract Since the discovery of the multiple endocrine neoplasia type 1 (MEN1) gene in 1997, Key Words elucidation of the molecular function of its protein product, menin, has been a challenge. f multiple endocrine Biochemical, proteomics, genetics and genomics approaches have identified various neoplasia type 1 (MEN1) potential roles, which converge on gene expression regulation. The most consistent f menin findings show that menin connects transcription factors and chromatin-modifying f transcriptional regulation enzymes, in particular, the histone H3K4 methyltransferase complexes MLL1 and MLL2. f histone H3K4 trimethylation Chromatin immunoprecipitation combined with next-generation sequencing has enabled studying genome-wide dynamics of chromatin binding by menin. We propose that menin regulates cell type-specific transcriptional programs by linking chromatin regulatory Endocrine-Related Cancer Endocrine-Related complexes to specific transcription factors. In this fashion, the MEN1 gene is a tumor suppressor gene in the endocrine tissues that are affected in MEN1. Recent studies have hinted at possibilities to pharmacologically restore the epigenetic changes caused by loss of menin function as therapeutic strategies for MEN1, for example, by inhibition of histone demethylases. -

International Journal of Infection Prevention Issn No: 2690-4837
Freely Available Online INTERNATIONAL JOURNAL OF INFECTION PREVENTION ISSN NO: 2690-4837 Research DOI: 10.14302/issn.2690-4837.ijip-20-3176 The Genetic Multiplicity- Multiple Endocrine Neoplasia type I Anubha Bajaj1,* 1MD. (Pathology) Panjab University, Department of Histopathology, A.B. Diagnostics, A-1, Ring Road, Rajouri Garden, New Delhi, 110027, India Abstract Multiple endocrine neoplasia type 1 (MEN1) is a syndrome emerging from characteristic mutations of MEN1 gene with concurrently enunciated multiple endocrine and tumours and associated non-endocrine neoplasm. Previously designated as Werner’s syndrome, MEN1 syndrome denominates genomic mutation within chromosome 11q13 or a tumour suppressor gene with a distinctive protein product nomenclated as “menin”. MEN1 syndrome demonstrates an autosomal dominant pattern of disease inheritance where genomic mutations delineate a comprehensive (100%) disease penetrance. MEN1 gene was initially identified in 1997 upon chromosome 11q13. Although twelve genetic mutations were primarily identified, currently beyond eighteen hundred genomic mutations are scripted [1,2]. MEN1 syndrome is comprised of diverse combination of twenty or more endocrine and non-endocrine tumours exemplifying a classic triad of pituitary, parathyroid and pancreatic neoplasm. Diverse non endocrine tumours enunciated with MEN1 syndrome are denominated with meningioma, ependymoma or angiofibroma [1,2]. Endocrine tumours are discerned on account of excessive hormonal secretion engendered from various neoplasm or on account of neoplastic evolution. Approximately 10% instances can occur due to a de-novo genomic variant. Offspring of an individual with MEN1 syndrome quantifies a 50% possibility of inheriting the genomic variant. Cogent prenatal diagnosis can be determined in instances where specific genomic variant of a particular family is known. -

Cdx4 and Menin Co-Regulate Hoxa9 Expression in Hematopoietic Cells Jizhou Yan, Ya-Xiong Chen, Angela Desmond, Albert Silva, Yuqing Yang, Haoren Wang, Xianxin Hua*
Cdx4 and Menin Co-Regulate Hoxa9 Expression in Hematopoietic Cells Jizhou Yan, Ya-Xiong Chen, Angela Desmond, Albert Silva, Yuqing Yang, Haoren Wang, Xianxin Hua* Abramson Family Cancer Research Institute, Department of Cancer Biology, Abramson Cancer Center, University of Pennsylvania, Philadelphia, Pennsylvania, United States of America Background. Transcription factor Cdx4 and transcriptional coregulator menin are essential for Hoxa9 expression and normal hematopoiesis. However, the precise mechanism underlying Hoxa9 regulation is not clear. Methods and Findings. Here, we show that the expression level of Hoxa9 is correlated with the location of increased trimethylated histone 3 lysine 4 (H3K4M3). The active and repressive histone modifications co-exist along the Hoxa9 regulatory region. We further demonstrate that both Cdx4 and menin bind to the same regulatory region at the Hoxa9 locus in vivo, and co-activate the reporter gene driven by the Hoxa9 cis-elements that contain Cdx4 binding sites. Ablation of menin abrogates Cdx4 access to the chromatin target and significantly reduces both active and repressive histone H3 modifications in the Hoxa9 locus. Conclusion. These results suggest a functional link among Cdx4, menin and histone modifications in Hoxa9 regulation in hematopoietic cells. Citation: Yan J, Chen Y-X, Desmond A, Silva A, Yang Y, et al. (2006) Cdx4 and Menin Co-Regulate Hoxa9 Expression in Hematopoietic Cells. PLoS ONE 1(1): e47. doi:10.1371/journal.pone.0000047 INTRODUCTION Hoxa9 overexpression is a common feature of acute myeloid Homeo-box-containing transcription factors (Hox proteins) play leukemia [19–21]. Although both menin and Cdx4 have been a pivotal role in normal differentiation and expansion of hemato- shown to participate in regulating Hoxa9 gene transcription and poietic cells [1,2].