Assessment of Benzodiazepines Dependence in Patients During
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

GABA Receptors
D Reviews • BIOTREND Reviews • BIOTREND Reviews • BIOTREND Reviews • BIOTREND Reviews Review No.7 / 1-2011 GABA receptors Wolfgang Froestl , CNS & Chemistry Expert, AC Immune SA, PSE Building B - EPFL, CH-1015 Lausanne, Phone: +41 21 693 91 43, FAX: +41 21 693 91 20, E-mail: [email protected] GABA Activation of the GABA A receptor leads to an influx of chloride GABA ( -aminobutyric acid; Figure 1) is the most important and ions and to a hyperpolarization of the membrane. 16 subunits with γ most abundant inhibitory neurotransmitter in the mammalian molecular weights between 50 and 65 kD have been identified brain 1,2 , where it was first discovered in 1950 3-5 . It is a small achiral so far, 6 subunits, 3 subunits, 3 subunits, and the , , α β γ δ ε θ molecule with molecular weight of 103 g/mol and high water solu - and subunits 8,9 . π bility. At 25°C one gram of water can dissolve 1.3 grams of GABA. 2 Such a hydrophilic molecule (log P = -2.13, PSA = 63.3 Å ) cannot In the meantime all GABA A receptor binding sites have been eluci - cross the blood brain barrier. It is produced in the brain by decarb- dated in great detail. The GABA site is located at the interface oxylation of L-glutamic acid by the enzyme glutamic acid decarb- between and subunits. Benzodiazepines interact with subunit α β oxylase (GAD, EC 4.1.1.15). It is a neutral amino acid with pK = combinations ( ) ( ) , which is the most abundant combi - 1 α1 2 β2 2 γ2 4.23 and pK = 10.43. -

Mexazolam: Clinical Efficacy and Tolerability in the Treatment of Anxiety
Neurol Ther DOI 10.1007/s40120-014-0016-7 REVIEW Mexazolam: Clinical Efficacy and Tolerability in the Treatment of Anxiety He´lder Fernandes • Ricardo Moreira To view enhanced content go to www.neurologytherapy-open.com Received: March 13, 2014 Ó The Author(s) 2014. This article is published with open access at Springerlink.com ABSTRACT published manuscripts of interest known by the authors (not indexed on PubMed) have been Introduction: Mexazolam is indicated for the added for completeness. Relevant information management of anxiety with or without was selected for inclusion by the authors. psychoneurotic conditions. In adult patients, Results: A number of early studies the recommended daily dosage of mexazolam is demonstrated the ability of mexazolam to 1–3 mg, administered three times daily. The reduce anxiety symptoms with few side effects objective of this article is to review the available in patients with disorders associated with information on the benzodiazepine (BZD) anxiety. Following on from this preliminary mexazolam and its clinical utility in treating evidence, controlled studies directly comparing patients with anxiety. mexazolam with other BZDs showed that the Methods: The PubMed database was searched drug is more effective than bromazepam and using the keyword ‘‘mexazolam’’ with no date or oxazolam, and is at least as effective as language restrictions applied to the search. As alprazolam. A larger, multicenter, phase IV only 11 papers were retrieved, some previously study also showed that mexazolam 2 or 3 mg/ Electronic supplementary material The online day rapidly improved Hamilton Anxiety Rating version of this article (doi:10.1007/s40120-014-0016-7) Scale scores and substantially reduced the contains supplementary material, which is available to authorized users. -

Drug and Medication Classification Schedule
KENTUCKY HORSE RACING COMMISSION UNIFORM DRUG, MEDICATION, AND SUBSTANCE CLASSIFICATION SCHEDULE KHRC 8-020-1 (11/2018) Class A drugs, medications, and substances are those (1) that have the highest potential to influence performance in the equine athlete, regardless of their approval by the United States Food and Drug Administration, or (2) that lack approval by the United States Food and Drug Administration but have pharmacologic effects similar to certain Class B drugs, medications, or substances that are approved by the United States Food and Drug Administration. Acecarbromal Bolasterone Cimaterol Divalproex Fluanisone Acetophenazine Boldione Citalopram Dixyrazine Fludiazepam Adinazolam Brimondine Cllibucaine Donepezil Flunitrazepam Alcuronium Bromazepam Clobazam Dopamine Fluopromazine Alfentanil Bromfenac Clocapramine Doxacurium Fluoresone Almotriptan Bromisovalum Clomethiazole Doxapram Fluoxetine Alphaprodine Bromocriptine Clomipramine Doxazosin Flupenthixol Alpidem Bromperidol Clonazepam Doxefazepam Flupirtine Alprazolam Brotizolam Clorazepate Doxepin Flurazepam Alprenolol Bufexamac Clormecaine Droperidol Fluspirilene Althesin Bupivacaine Clostebol Duloxetine Flutoprazepam Aminorex Buprenorphine Clothiapine Eletriptan Fluvoxamine Amisulpride Buspirone Clotiazepam Enalapril Formebolone Amitriptyline Bupropion Cloxazolam Enciprazine Fosinopril Amobarbital Butabartital Clozapine Endorphins Furzabol Amoxapine Butacaine Cobratoxin Enkephalins Galantamine Amperozide Butalbital Cocaine Ephedrine Gallamine Amphetamine Butanilicaine Codeine -
Report on the Investigation Results
Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. Report on the Investigation Results February 28, 2017 Pharmaceuticals and Medical Devices Agency I. Overview of Product [Non-proprietary name] See Attachment 1 [Brand name] See Attachment 1 [Approval holder] See Attachment 1 [Indications] See Attachment 1 [Dosage and administration] See Attachment 1 [Investigating office] Office of Safety II 1 Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. II. Background of the investigation 1. Status in Japan Hypnotics and anxiolytics are prescribed by various specialties and widely used in clinical practice. In particular, benzodiazepine (BZ) receptor agonists, which act on BZ receptors, bind to gamma-aminobutyric acid (GABA)A-BZ receptor complex and enhance the function of GABAA receptors. This promotes neurotransmission of inhibitory systems and demonstrates hypnotic/sedative effects, anxiolytic effects, muscle relaxant effects, and antispasmodic effects. Since the approval of chlordiazepoxide in March 1961, many BZ receptor agonists have been approved as hypnotics and anxiolytics. Currently, hypnotics and anxiolytics are causative agents of drug-related disorders such as drug dependence in Japanese clinical practice. Hypnotics and anxiolitics that rank high in causative agents are BZ receptor agonists for which high frequencies of high doses and multidrug prescriptions have been reported (Japanese Journal of Clinical Psychopharmacology 2013; 16(6): 803-812, Modern Physician 2014; 34(6): 653-656, etc.). -

II.3.4 Benzodiazepines by Hiroshi Seno and Hideki Hattori
3.4 II.3.4 Benzodiazepines by Hiroshi Seno and Hideki Hattori Introduction Benzodiazepines show antianxiety, hypnotic, anticonvulsant and muscle-relaxant eff ects. Th is group of drugs has wide safety dose ranges; it means that the ratio of the LD50 to the ED50 (therapeutic index) is high. Because of its safety, benzodiazepines are being widely used in the world. Some of benzodiazepines are also being abused or used for so-called “ drug facilitated sexual assault”, and thus they are under the control of the Narcotics and Psychotropics Control Law; in Japan, triazolam abuse has become one of the serious social problems. In this chapter, a GC/MS method for simultaneous analysis of 22 kinds of benzodiazepines listed in > Table 4.1 is described. In addition, the LC/MS analysis of triazolam, and its metabolites 4-hydroxy- triazolam and α-hydroxytriazolam is also presented. GC/MS analysis of benzodiazepines in blood and urine Reagents and their preparation • Th e pure powder of the 22 kinds of benzodiazepines was donated by each pharmaceutical manufacturers according to the authors’ request a (some of benzodiazepines now obtaina- ble from Sigma, St. Louis, MO, USA). • 1 M Sodium bicarbonate solution: a 8.4-g aliquot of sodium bicarbonate is dissolved in distilled water to prepare 100 mL solution. • 2 M Sodium acetate solution: a 27.5-g aliquot of sodium acetate is dissolved in distilled water to prepare 100 mL solution. GC/MS conditions Column: a DB-5 fused silica capillary column (30 m × 0.25 mm i.d., fi lm thickness 0.25 µm, J & W Scientifi c, Folsom, CA, USA). -

Title Continuation and Discontinuation of Benzodiazepine Prescriptions: A
Continuation and discontinuation of benzodiazepine Title prescriptions: A cohort study based on a large claims database in Japan( Dissertation_全文 ) Author(s) Takeshima, Nozomi Citation 京都大学 Issue Date 2016-05-23 URL https://doi.org/10.14989/doctor.k19890 Right Type Thesis or Dissertation Textversion ETD Kyoto University Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎ Contents lists available at ScienceDirect Psychiatry Research journal homepage: www.elsevier.com/locate/psychres Continuation and discontinuation of benzodiazepine prescriptions: A cohort study based on A large claims database in Japan Nozomi Takeshima, Yusuke Ogawa, Yu Hayasaka, Toshi A Furukawa n Department of Health Promotion and Human Behavior, Kyoto University Graduate School of Medicine/School of Public Health, Yoshida Konoe-cho, Sakyo-ku, Kyoto 606-8501, Japan article info abstract Article history: Although benzodiazepines (BZDs) are often prescribed to treat a wide range of psychiatric and neuro- Received 29 March 2015 logical conditions, they are also associated with various harms and risks including dependence. However Received in revised form the frequency of its continued use in the real world has not been well studied, especially at longer follow- 15 October 2015 ups. The aim of this study was to clarify the frequency of long-term BZD use among new BZD users over Accepted 15 January 2016 longer follow-ups and to identify its predictors. We conducted a cohort study to examine how frequently new BZD users became chronic users, based on a large claims database in Japan from January 2005 to Keywords: June 2014. We used Cox proportional hazards models to identify potential predictors. A total 84,412 Benzodiazepine patients with new BZD prescriptions were included in our cohort. -
PMDA Alert for Proper Use of Drugs When Using Benzodiazepine
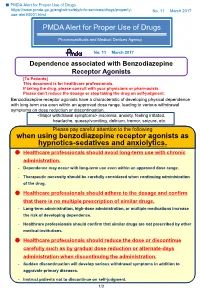
■ PMDA Alert for Proper Use of Drugs https://www.pmda.go.jp/english/safety/info-services/drugs/properly- No. 11 March 2017 use-alert/0001.html PMDA Alert for Proper Use of Drugs Pharmaceuticals and Medical Devices Agency No. 11 March 2017 Dependence associated with Benzodiazepine Receptor Agonists [To Patients] This document is for healthcare professionals. If taking the drug, please consult with your physicians or pharmacists. Please don’t reduce the dosage or stop taking the drug on self-judgment. Benzodiazepine receptor agonists have a characteristic of developing physical dependence with long-term use even within an approved dose range, leading to various withdrawal symptoms on dose reduction or discontinuation. <Major withdrawal symptoms> insomnia, anxiety, feeling irritated, headache, queasy/vomiting, delirium, tremor, seizure, etc. Please pay careful attention to the following when using benzodiazepine receptor agonists as hypnotics-sedatives and anxiolytics. Healthcare professionals should avoid long-term use with chronic administration. - Dependence may occur with long-term use even within an approved dose range. - Therapeutic necessity should be carefully considered when continuing administration of the drug. Healthcare professionals should adhere to the dosage and confirm that there is no multiple prescription of similar drugs. - Long-term administration, high-dose administration, or multiple medications increase the risk of developing dependence. - Healthcare professionals should confirm that similar drugs are not prescribed by other medical institutions. Healthcare professionals should reduce the dose or discontinue carefully such as by gradual dose reduction or alternate-days administration when discontinuing the administration. - Sudden discontinuation will develop serious withdrawal symptoms in addition to aggravate primary diseases. -

WO 2008/137960 Al
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date PCT 13 November 2008 (13.11.2008) WO 2008/137960 Al (51) International Patent Classification: (74) Agents: GRUMBLING, Matthew, V. et al; Wilson Son- A61K 37/55 (2006.01) sini Goodrich & Rosati, 650 Page Mill Road, Palo Alto, CA 94304-1050 (US). (21) International Application Number: (81) Designated States (unless otherwise indicated, for every PCT/US2008/062961 kind of national protection available): AE, AG, AL, AM, AO, AT,AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, CA, (22) International Filing Date: 7 May 2008 (07.05.2008) CH, CN, CO, CR, CU, CZ, DE, DK, DM, DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, HR, HU, ID, (25) Filing Language: English IL, IN, IS, JP, KE, KG, KM, KN, KP, KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, (26) Publication Language: English MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, PG, PH, PL, PT, RO, RS, RU, SC, SD, SE, SG, SK, SL, SM, SV, (30) Priority Data: SY, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, 60/916,550 7 May 2007 (07.05.2007) US ZA, ZM, ZW (84) Designated States (unless otherwise indicated, for every (71) Applicant (for all designated States except US): kind of regional protection available): ARIPO (BW, GH, QUESTOR PHARMACEUTICALS, INC. [US/US]; GM, KE, LS, MW, MZ, NA, SD, SL, SZ, TZ, UG, ZM, 3260 Whipple Road, Union City, CA 94587 (US). -

Antidepressants Plus Benzodiazepines Lead to Fewer Dropouts and Less Depression Severity at 4 Weeks in Major Depression
Evid Based Mental Health: first published as 10.1136/ebmh.4.2.45 on 1 May 2001. Downloaded from Review: antidepressants plus benzodiazepines lead to Sources of funding: fewer dropouts and less depression severity at 4 weeks Ministry of Health and Welfare, Japan; Uehara in major depression Memorial Foundation, Japan. Furukawa T,Streiner DL, Young LT. Antidepressant plus benzodiazepine for major depression. Cochrane Database Syst Rev For correspondence: 2000;(4):CD001026 (latest version 29 Aug 2000). Professor T Furukawa, Department of Psychiatry, Nagoya City University, School of QUESTION: In adults with major depression, does combination treatment with Medicine, Mizuho-cho antidepressants and benzodiazepines lead to any benefits in terms of short term Mizuho-ku Aichi, Nagoya, Japan, 467 (<8 wks) or long term (>2 mo) symptomatic recovery or side effects? 8601. Fax +81 52 852 0837. Data sources Combined antidepressant and benzodiazepine treatment v antidepressant alone in adults Studies were identified by searching Medline, EMBASE/ with major depression* Excerpta Medica, International Pharmaceutical Ab- Weighted event rates stracts, Biological Abstracts, LILACS, PsycLIT, the Antidepressant Cochrane Library, and the trial register of the Cochrane Outcomes Combined alone RRR (95% CI) NNT (CI) Depression, Anxiety and Neurosis Group (January 1972 to December 1998); handsearching major mental health Dropped out 22% 33% 37% (19 to 51) 10 (6 to 22) and general medicine journals; scanning the reference Dropped out due lists of identified articles; checking SciSearch; and by to side effects 7% 14% 48% (14 to 68) 15 (10 to 40) personal contacts. Antidepressant Combined alone RBI (CI) NNT (CI) Study selection >50% reduction in Studies were selected if they were randomised controlled depression at 4 trials comparing combined antidepressant-benzodiazepine weeks 52% 37% 38% (15 to 66) 7 (5 to 15) treatment with antidepressants alone in adults with major *Abbreviations defined in glossary; RRR, RBI, NNT, and CI calculated from data in article. -

Generalised Anxiety Disorder
Evid Based Mental Health: first published as 10.1136/ebmh.7.2.34 on 23 April 2004. Downloaded from 32 EBMH Notebook............................................................................... Generalised anxiety disorder he EBMH Notebook summarises key messages about AETIOLOGY/RISK FACTORS generalised anxiety disorder, sourced from: Clin Evid Generalised anxiety disorder is believed to be associated with Concise 2004 (in press); www.clinicalevidence.com. For an increase in the number of minor stressors, independent of T 14 15 this review, Clinical Evidence Concise searched and appraised demographic factors, but this finding is also common in material published until June 2003. people with other diagnoses in the clinical population.10 One non-systematic review (five case control studies) of psycho- DEFINITION logical sequelae to civilian trauma found that rates of GAD Generalised anxiety disorder (GAD) is defined as excessive reported in four of the five studies were significantly worry and tension about every day events and problems on increased compared with a control population (rate ratio most days, for at least six months, to the point where the 3.3, 95% CI 2.0 to 5.5).16 One systematic review (search date person experiences distress or has marked difficulty in 1997) of cross sectional studies found that bullying (or peer performing day to day tasks.1 It may be characterised by victimisation) was associated with a significant increase in the following symptoms and signs: increased motor tension the incidence of GAD (effect size -

List of Benzodiazepines - Wikipedia, the Free Encyclopedia
List of benzodiazepines - Wikipedia, the free encyclopedia Log in / create account Article Talk Read Edit Our updated Terms of Use will become effective on May 25, 2012. Find out more. List of benzodiazepines From Wikipedia, the free encyclopedia Main page The below tables contain a list of benzodiazepines that Benzodiazepines Contents are commonly prescribed, with their basic pharmacological Featured content characteristics such as half-life and equivalent doses to other Current events benzodiazepines also listed, along with their trade names and Random article primary uses. The elimination half-life is how long it takes for Donate to Wikipedia half of the drug to be eliminated by the body. "Time to peak" Interaction refers to when maximum levels of the drug in the blood occur Help after a given dose. Benzodiazepines generally share the About Wikipedia same pharmacological properties, such as anxiolytic, Community portal sedative, hypnotic, skeletal muscle relaxant, amnesic and Recent changes anticonvulsant (hypertension in combination with other anti The core structure of benzodiazepines. Contact Wikipedia hypertension medications). Variation in potency of certain "R" labels denote common locations of effects may exist among individual benzodiazepines. Some side chains, which give different Toolbox benzodiazepines produce active metabolites. Active benzodiazepines their unique properties. Print/export metabolites are produced when a person's body metabolizes Benzodiazepine the drug into compounds that share a similar pharmacological -
High-Sensitivity and Simultaneous Analysis of Psychoactive Drugs Using LC-MS/MS with Full-Automated Pretreatment System
PO-CON1714E High-sensitivity and simultaneous analysis of Psychoactive drugs using LC-MS/MS with full-automated pretreatment system ASMS 2017 WP358 Daisuke Kawakami1, Toshikazu Minohata1 1 Shimadzu Corporation. 1, Nishinokyo-Kuwabaracho Nakagyo-ku, Kyoto 604–8511, Japan High-sensitivity and simultaneous analysis of Psychoactive drugs using LC-MS/MS with full-automated pretreatment system Introduction LC-MS/MS has become a preferred method for the routine also increasing to investigate the cause of death. However, analysis for forensic toxicology. LC-MS/MS allows for the manual sample preparation often involves several simultaneous analysis of multiple compounds in a single complicated manual steps which can introduce error into run, thus enabling a fast and high throughput analysis. In the results. In this study, we investigated the processing recent years that it seems the number of incident and capability to analyze serum, whole blood and urine spiked accident is increasing caused by dosed with psychotropic sixty psychotropic drugs by LC-MS/MS with automated drugs and the number of drug testing with LC-MS/MS is sample preparation unit. Group 1. Eight Barbiturate drug and Bromovalerylurea Allobarbital Amobarbital Barbital Pentobarbital Phenobarbital Secobarbital Thiamylal Thiopental Bromovalerylurea Group 2. twelve Tri-/Tetra-cyclic antidepressant Amitriptyline Amoxapine Clomipramine Desipramine Dosulepin Imipramine Maprotiline Mianserin Nortriptyline Promethazine Setiptiline Group 3. Thirty-nine Benzodiazepines and their metabolites