Cutaneous Diseases of the External Genitalia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/05 (2006.01) A61P 31/02 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/CA20 14/000 174 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 4 March 2014 (04.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13/790,91 1 8 March 2013 (08.03.2013) US (84) Designated States (unless otherwise indicated, for every (71) Applicant: LABORATOIRE M2 [CA/CA]; 4005-A, rue kind of regional protection available): ARIPO (BW, GH, de la Garlock, Sherbrooke, Quebec J1L 1W9 (CA). GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, (72) Inventors: LEMIRE, Gaetan; 6505, rue de la fougere, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, Sherbrooke, Quebec JIN 3W3 (CA). -

15. Dermatology Eponyms
Dermatology Eponyms DERMATOLOGY EPONYMS – PHENOMEN / SIGN – LEXICON (D) Brzeziński Piotr1, Wollina Uwe2, Poklękowska Katarzyna3, Khamesipour Ali4, Herrero Gonzalez Jose Eugenio5, Bimbi Cesar6, Di Lernia Vito7, Karwan Krzysztof 8 16th Military Support Unit, Ustka, Poland. [email protected] 2Department of Dermatology & Allergology, Hospital Dresden-Friedrichstadt, Academic Teaching Hospital of the Technical University of Dresden, Dresden, Germany [email protected] 3Mazowiecki Branch of the National Health Fund, Warsaw, Poland [email protected] 4Center for Research and Training in Skin Diseases and Leprosy, Tehran University of Medical Sciences, Tehran, Iran [email protected] 5Malalties Ampul.lars i Porfíries, Departament de Dermatologia, Hospital del Mar, Barcelona, Spain [email protected] 6Brazilian Society of Dermatology [email protected] 7Department of Dermatology, Arcispedale Santa Maria Nuova, Reggio Emilia, Italy [email protected] 8The Emergency Department, Military Institute of Medicine, Warsaw, Poland [email protected] N Dermatol Online. 2011; 2(3): 158-170 Date of submission: 08.04.2011 / acceptance: 29.05.2011 Conflicts of interest: None DANIELSSEN’S SIGN Anesthetic leprosy. A form of leprosy chiefly affecting the nerves, marked by hyperesthesia succeeded by anesthesia, and by paralysis, ulceration, and various trophic disturbances, terminating in gangrene and mutilation. In 1895 I presented to the Ohio State Medical Society two sisters, natives of Ohio, who manifested appearances of anesthetic leprosy. Synonyms: Danielssen disease, Danielssen-Boeck disease, dry leprosy, trophoneurotic leprosy. OBJAW DANIELSSENA Anesthetic leprosy. Postać trądu głównie wpływająca na nerwy, początkowo charakteryzuje się oznaczone przeczulicą, następcą znieczulicą i paraliŜem, owrzodzeniem i róŜnymi zaburzeniami troficznymi, kończąca się w gangreną i okaleczeniem. W 1895 roku przedstawiono w Ohio State Medical Society dwie siostry z Ohio, u których występowały objawy anesthetic Figure 1. -

CHAPTER E16 Atlas of Skin Manifestations of Internal Disease CHAPTER E16 Thomas J
CHAPTER e16 Atlas of Skin Manifestations of Internal Disease CHAPTER e16 Thomas J. Lawley Robert A. Swerlick In the practice of medicine, virtually every clinician encounters patients with skin disease. Physicians of all specialties face the daily task of determining the nature and clinical implication of dermatologic disease. In patients with skin eruptions and rashes, the physician must confront the question of whether the cutaneous Atlas of Skin Manifestations Internal Disease process is confined to the skin, representing a pure dermatologic event, or whether it is a manifestation of internal disease relating to the patient’s overall medical condition. Evaluation and accurate diagnosis of skin lesions are also critical given the marked rise in both melanoma and nonmelanoma skin cancer. Dermatologic conditions can be classified and categorized in many different ways, Figure e16-2 Acne rosacea with prominent facial erythema, telangiecta- and in this Atlas, a selected group of inflammatory skin eruptions sias, scattered papules, and small pustules. (Courtesy of Robert Swerlick, and neoplastic conditions are grouped in the following manner: MD; with permission.) (A) common skin diseases and lesions, (B) nonmelanoma skin cancer, (C) melanoma and pigmented lesions, (D) infectious dis- ease and the skin, (E) immunologically mediated skin disease, and (F) skin manifestations of internal disease. COMMON SKIN DISEASES AND LESIONS ( Figs. e16-1 to e16-19) In this section, several common inflamma- tory skin diseases and benign neoplastic and reactive lesions are presented. While most of these dermatoses usually present as a pre- dominantly dermatologic process, underlying systemic associations may be made in some settings. Atopic dermatitis is often present in patients with an atopic diathesis, including asthma and sinusitis. -
Ecthyma Gangrenosum of a Single Limb
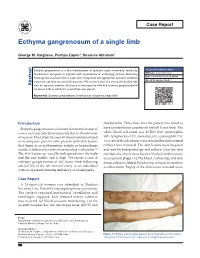
Case Report Ecthyma gangrenosum of a single limb George M. Varghese, Pushpa Eapen1, Susanne Abraham1 Ecthyma gangrenosum is a skin manifestation of systemic sepsis commonly caused by Access this article online Pseudomonas aeruginosa in patients with neutropenia or underlying immune deficiency. Website: www.ijccm.org Although the usual outcome is poor, early recognition and appropriate systemic antibiotic DOI: 10.4103/0972-5229.84898 treatment can lead to successful outcome. We report a case of a previously healthy lady Quick Response Code: Abstract with no apparent immune deficiency or neutropenia who had ecthyma gangrenosum of left lower limb in which the arterial line was placed. Keywords: Ecthyma gangrenosum, Pseudomonas aeruginosa, single limb Introduction thachycardia. Three days later the patient was noted to Ecthyma gangrenosum is a known skin manifestation of have erythematous papules on the left lower limb. The 3 severe systemic infection commonly due to Pseudomonas white blood cell count was 16,500/mm (neutrophils aeruginosa. Most often it is seen in immunocompromised 84%, lymphocytes 12%, monocytes 3%, eosinophils 1%). or neutropenic patients who present with skin lesions Two sets of blood cultures were sent and the intra-arterial that begin as an erythematous nodule or hemorrhagic catheter was removed. The skin lesions were biopsied vesicle, which evolves into a necrotic ulcer with eschar. [1] and sent for histopathology and culture. Over the next The skin lesions are usually widespread over the body few days the skin lesions became blackish with necrotic and the case fatality rate is high. We report a case of areas (arrow) [Figure 1]. The blood, catheter tip, and skin ecthyma gangrenosum of left lower limb following lesion cultures yielded Pseudomonas aeruginosa sensitive arterial line in the left femoral artery in an individual to ceftazidime. -

Skin and Soft Tissue Infections Following Marine Injuries
CHAPTER 6 Skin and Soft Tissue Infections Following Marine Injuries V. Savini, R. Marrollo, R. Nigro, C. Fusella, P. Fazii Spirito Santo Hospital, Pescara, Italy 1. INTRODUCTION Bacterial diseases following aquatic injuries occur frequently worldwide and usually develop on the extremities of fishermen and vacationers, who are exposed to freshwater and saltwater.1,2 Though plenty of bacterial species have been isolated from marine lesions, superficial soft tissue and invasive systemic infections after aquatic injuries and exposures are related to a restricted number of microorganisms including, in alphabetical order, Aeromonas hydrophila, Chromobacterium violaceum, Edwardsiella tarda, Erysipelothrix rhusiopathiae, Myco- bacterium fortuitum, Mycobacterium marinum, Shewanella species, Streptococcus iniae, and Vibrio vulnificus.1,2 In particular, skin disorders represent the third most common cause of morbidity in returning travelers and are usually represented by bacterial infections.3–12 Bacterial skin and soft tissue infectious conditions in travelers often follow insect bites and can show a wide range of clinical pictures including impetigo, ecthyma, erysipelas, abscesses, necro- tizing cellulitis, myonecrosis.3–12 In general, even minor abrasions and lacerations sustained in marine waters should be considered potentially contaminated with marine bacteria.3–12 Despite variability of the causative agents and outcomes, the initial presentations of skin and soft tissue infections (SSTIs) complicating marine injuries are similar to those occurring after terrestrial exposures and usually include erysipelas, impetigo, cellulitis, and necrotizing infections.3 Erysipelas is characterized by fiery red, tender, painful plaques showing well-demarcated edges, and, though Streptococcus pyogenes is the major agent of this pro- cess, E. rhusiopathiae infections typically cause erysipeloid displays.3 Impetigo is initially characterized by bullous lesions and is usually due to Staphylococcus aureus or S. -

Clinical Dermatology Notice
This page intentionally left blank Clinical Dermatology Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The editors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the editors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of such information contained in this work. Readers are encouraged to confirm the information contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. a LANGE medical book Clinical Dermatology Carol Soutor, MD Clinical Professor Department of Dermatology University of Minnesota Medical School Minneapolis, Minnesota Maria K. Hordinsky, MD Chair and Professor Department of Dermatology University of Minnesota Medical School Minneapolis, Minnesota New York Chicago San Francisco Lisbon London Madrid Mexico City Milan New Delhi San Juan Seoul Singapore Sydney Toronto Copyright © 2013 by McGraw-Hill Education, LLC. -

Cutaneous Manifestations of Infection in the Immunocompromised Host
Cutaneous Manifestations of Infection in the Immunocompromised Host Marc E. Grossman • Lindy P. Fox • Carrie Kovarik Misha Rosenbach Cutaneous Manifestations of Infection in the Immunocompromised Host Second Edition Authors Marc E. Grossman, M.D. Carrie Kovarik, M.D. Professor of Clinical Dermatology Assistant Professor of Dermatology College of Physicians and Surgeons Dermatopathology, and Infectious Diseases Director, Hospital Consultation Service University of Pennsylvania New York Presbyterian Hospital Philadelphia, Pennsylvania, USA Columbia University Medical Center New York, New York, USA Misha Rosenbach, M.D. Assistant Professor of Dermatology Lindy P. Fox, M.D. and Internal Medicine Associate Professor of Clinical Dermatology Director, Dermatology Inpatient Consult Service Director, Hospital Consultation Service University of Pennsylvania University of California, San Francisco Philadelphia, Pennsylvania, USA San Francisco, California, USA ISBN 978-1-4419-1577-1 e-ISBN 978-1-4419-1578-8 DOI 10.1007/978-1-4419-1578-8 Springer New York Dordrecht Heidelberg London Library of Congress Control Number: 2011933837 Springer Science+Business Media, LLC 2012 All rights reserved. Th is work may not be translated or copied in whole or in part without the written permission of the publisher (Springer Science+Business Media, LLC, 233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection with reviews or scholarly analysis. Use in connection with any form of information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter devel- oped is forbidden. Th e use in this publication of trade names, trademarks, service marks, and similar terms, even if they are not identifi ed as such, is not to be taken as an expression of opinion as to whether or not they are subject to proprietary rights. -
Dermatology in the ER
DRUG ERUPTIONS and OTHER DISORDERS Lloyd J. Cleaver D.O. , F.A.O.C.D, F.A.A.D. Professor of Dermatology ATSU-Kirksville College of Osteopathic Medicine INTERNAL MEDICINE BOARD REVIEW COURSE I Disclosures No Relevant Financial Relationships DRUG ERUPTIONS Drug Reactions 3 things you need to know 1. Type of drug reaction 2. Statistics What drugs are most likely to cause that type of reaction? 3. Timing How long after the drug was started did the reaction begin? Clinical Pearls Drug eruptions are extremely common Tend to be generalized/symmetric Maculopapular/morbilliform are most common Best Intervention: Stop the Drug! Do not dose reduce Completely remove the exposure How to spot the culprit? Drug started within days to a week prior to rash Can be difficult and take time Tip: can generally exclude all drugs started after onset of rash Drug eruptions can continue for 1-2 weeks after stopping culprit drug LITT’s drug eruption database Drug Eruptions Skin is one of the most common targets for drug reactions Antibiotics and anticonvulsants are most common 1-5% of patients 2% of all drug eruptions are “serious” TEN, DRESS More common in adult females and boys < 3 y/o Not all drugs cause eruptions at same rate: Aminopenicillins: 1.2-8% of exposures TMP-SMX: 2.8-3.7% NSAIDs: 1 in 200 Lamotrigine: 10% Drug Eruptions Three basic rules 1. Stop any unnecessary medications 2. Ask about non-prescription medications Eye drops, suppositories, implants, injections, patches, vitamin and health supplements, friend’s medications -

Abdominal Distension, 284 Abdominal Mass, Hydatid Disease, 287
Cambridge University Press 978-0-521-69761-3 - Case Studies in Pediatric Infectious Diseases Frank E. Berkowitz Index More information Index Abdominal distension, 284 perivenous, 240 Abdominal mass, hydatid disease, psoas 287 tuberculosis, 226 Abdominal pain, 12, 79, 112, 158, 169, 177, retropharyngeal, 100, 264, 318 257, 270, 273, 304, 308 tuberculosis, 226 acute HIV infection, 311 spinal epidural, 273 appendicitis, 253 spinal cat-scratch disease, 143 paraplegia, 262 hydatid disease, 287 subphrenic, 232 leptospirosis, 139 tubo-ovarian, 322 pelvic inflammatory disease, 319 Absidia, taxonomy, 347 peritonitis, 315 Acanthameba, taxonomy, 348 pneumonia, 248 Acetaminophen, 15, 54 pyelonephritis, 244 Acetylcholine, 129 typhus, 149 Acid-fast bacilli See Mycobacteria Abdominal tenderness, 257 Acidosis, diarrhea, 80 Abscess Acinetobacter, taxonomy, 342 appendix, 159, 255 Acquired immunodeficiency syndrome, 146, brain, 43, 66, 255 193, 210, 242 meningitis, 108 reportable, 336 seizure, 195 Actinobacillus actinomycetemcomitans, 153 Brodie’s, 282 taxonomy, 343 cerebellar, 327 infective endocarditis, 297 dental, 271 Actinomyces, 124, 127 epidural, 334 taxonomy, 344 eye, 314 Actinomyces israelii, 125 lateral pharyngeal, 264 Actinomyces odontolyticus, taxonomy, liver, 13, 174 344 amebic, 174 Actinomycosis, 125 lung, 249 Acute chest syndrome, sickle cell disease, 249, odontogenic See Abscess 324 dental Acyclovir, 42 pelvic, 306 Epstein–Barr virus, 39 peritonsillar, 100, 264 herpes simplex virus, 29 Lemierre syndrome, 332 varicella, 47 355 © Cambridge University -

Genital Psoriasis: a Systematic Literature Review on This Hidden Skin Disease
Acta Derm Venereol 2011 ; 91 ; 5-11 REVIEW ARTICLE Genital Psoriasis: A Systematic Literature Review on this Hidden Skin Disease Kim A. P. MEEUWIS'-^ Joanne A. DE HULLU^ Leon F. A. G. MASSUGER^ Peter C. M. VAN DE KERKHOF' and Michelle M. VAN ROSSUM' Departments of 'Dermatology and 'Obstetrics and Gynaecology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands It is well known that the genital skin may be affected by of inverse psoriasis (synonym: flexural or intertriginous psoriasis. However, little is known about the prevalence psoriasis) (2, 4, 5). and clinical appearance of genital psoriasis, and genital The external genital skin is generally classified as skin is often neglected in the treatment of psoriatic pa- flexural skin, although it forms a unique area compri- tients. We performed an extensive systematic literature sing different structures and types of epithelium. The search for evidence-based data on genital psoriasis with epithelium covering the different structures of the vulva respect to epidemiology, aetiology, clinical and histopat- changes from stratified, keratinised squamous cell epit- hological presentation, diagnosis and treatment. Three helium on the outer parts to mucosa on the innermost bibliographical databases (PubMed, EMBASE and the regions (5, 6). Similarly, the male genital epithelium Cochrane Library) were used as data sources. Fifty-nine has a different pattern of keratinisation throughout the articles on genital psoriasis were included. The results genital area. The prepuce forms the anatomical cover- show that psoriasis frequently affects the genital skin, ing of the glans penis and is the junction between the but that evidence-based data with respect to the efficacy mucosal surface of the glans and coronal sulcus and the and safety of treatments for genital psoriasis are extre- keratinised squamous cell epithelium of the remaining mely limited. -

Dermatological Indications of Disease - Part II This Patient on Dialysis Is Showing: A
“Cutaneous Manifestations of Disease” ACOI - Las Vegas FR Darrow, DO, MACOI Burrell College of Osteopathic Medicine This 56 year old man has a history of headaches, jaw claudication and recent onset of blindness in his left eye. Sed rate is 110. He has: A. Ergot poisoning. B. Cholesterol emboli. C. Temporal arteritis. D. Scleroderma. E. Mucormycosis. Varicella associated. GCA complex = Cranial arteritis; Aortic arch syndrome; Fever/wasting syndrome (FUO); Polymyalgia rheumatica. This patient missed his vaccine due at age: A. 45 B. 50 C. 55 D. 60 E. 65 He must see a (an): A. neurologist. B. opthalmologist. C. cardiologist. D. gastroenterologist. E. surgeon. Medscape This 60 y/o male patient would most likely have which of the following as a pathogen? A. Pseudomonas B. Group B streptococcus* C. Listeria D. Pneumococcus E. Staphylococcus epidermidis This skin condition, erysipelas, may rarely lead to septicemia, thrombophlebitis, septic arthritis, osteomyelitis, and endocarditis. Involves the lymphatics with scarring and chronic lymphedema. *more likely pyogenes/beta hemolytic Streptococcus This patient is susceptible to: A. psoriasis. B. rheumatic fever. C. vasculitis. D. Celiac disease E. membranoproliferative glomerulonephritis. Also susceptible to PSGN and scarlet fever and reactive arthritis. Culture if MRSA suspected. This patient has antithyroid antibodies. This is: • A. alopecia areata. • B. psoriasis. • C. tinea. • D. lichen planus. • E. syphilis. Search for Hashimoto’s or Addison’s or other B8, Q2, Q3, DRB1, DR3, DR4, DR8 diseases. This patient who works in the electronics industry presents with paresthesias, abdominal pain, fingernail changes, and the below findings. He may well have poisoning from : A. lead. B. -

B K B Ld I MD Brooke Baldwin, MD Private Practice, Lutz, Florida Chief
BBkrooke BBldialdwin, MD Private Practice, Lutz, Florida Chief of Dermatology James A Haley VA Hospital Adjunct Assistant Professor of Dermatology University of Florida What we are going to cover today Dermatologic Emergencies Common benign skin growths Malignant skin tumors Common Rashes Photoprotecti on and CiCosmetics Dermatologic Emergencies Erythroderma PlPustular psoriiiasis Pemphigus DRESS Syndrome SJS / TEN EEthdrythroderma Erythroderma Generalized redness and scaling of skin involving >90% BSA Systemic manifestations PihPeripheral edema & ffilacial edema Tachycardia Loss of fluids and proteins Disturbed thermoregulation Most common etiologies Atopic dermatitis, psoriasis, CTCL, drug reactions Despite intensive evaluation, the cause remains unknown in 25‐30% PPlustular psoriiiasis Pustular Psoriasis Generalized pustular psoriasis Unusual mani festation o f psoriasis Triggering factors Pregnancy (impetigo herpetiformis) Tapering of corticosteroids (Von Zumbusch reaction) HliHypocalcemia Infections Topical irritants Rarely treatment with TNF alpha blockers (palms and soles) Pemphigus Group of chronic autoimmune blistering diseases presenting with painful erosions IgG Autoantibodies are directed against the cell surface of keratinocytes Results in blistering in varying areas of the epidermis Diagnosi s is confirmed wihith direct iflimmunofluorescence on skin biopsy 3 ma jor forms P. vulgaris, P. foliaceus, paraneoplastic Do not confuse with Bullous pemphigoid which presents with tense bullae Pempgphigus