National Burden of Disease Studies: Apractical Guide
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Better Together TNVR and Public Health APHA 11-13-18.Pdf
Better Together: TNVR and Public Health 11/13/2018 Presenter Disclosures Introduction Better Together TNVR and public health Peter J. Wolf and G. Robert Weedon • TNVR: trap-neuter-vaccinate-return G. Robert Weedon, DVM, MPH Clinical Assistant Professor and Service Head (Retired) Shelter Medicine, College of Veterinary Medicine University of Illinois • Emphasis on the “V” Peter J. Wolf, MS Research/Policy Analyst – Vaccination Best Friends Animal Society Have no relationships to disclose • Emphasizes the public health aspect of TNVR programs • Vaccinating against rabies as a means of protecting the health of the public Introduction TNVR TNVR • Why TNVR? • Why TNVR? – The only humane way to – More than half of impounded cats are euthanized deal with the problem of due to shelter crowding, shelter-acquired disease free-roaming (feral, or feral behavior animal welfareTNVR public health community) cats – TNVR, an alternative to shelter impoundment, – When properly applied, improves cat welfare and reduces the size of cat TNVR has been shown to colonies control/reduce populations rabies prevention of free-roaming cats Levy, J. K., Isaza, N. M., & Scott, K. C. (2014). Effect of high-impact targeted trap-neuter-return and adoption Levy, J. K., Isaza, N. M., & Scott, K. C. (2014). Effect of high-impact targeted trap-neuter-return and adoption of community cats on cat intake to a shelter. The Veterinary Journal, 201(3), 269–274. of community cats on cat intake to a shelter. The Veterinary Journal, 201(3), 269–274. TNVR TNVR TNVR • Why TNVR? • Why -

How to Measure the Burden of Mortality? L Bonneux
J Epidemiol Community Health: first published as 10.1136/jech.56.2.128 on 1 February 2002. Downloaded from 128 THEORY AND METHODS How to measure the burden of mortality? L Bonneux ............................................................................................................................. J Epidemiol Community Health 2002;56:128–131 Objectives: To explore various methods to quantify the burden of mortality, with a special interest for the more recent method at the core of calculations of disability adjusted life years (DALY). Design: Various methods calculating the age schedule at death are applied to two historical life table populations. One method calculates the “years of life lost”, by multiplying the numbers of deaths at age ....................... L Bonneux, Department of x by the residual life expectancy. This residual life expectancy may be discounted and age weighted. Public Health, Erasmus The other method calculates the “potential years of life lost” by multiplying the numbers of deaths at age University Rotterdam, the x by the years missing to reach a defined threshold (65 years or 75 years). Netherlands Methods: The period life tables describing the mortality of Dutch male populations from 1900–10 Correspondence to: (high mortality) and from 1990–1994 (low mortality). Dr L Bonneux, Department Results: A standard life table with idealised long life expectancy increases the burden of death more of Public Health, Erasmus if mortality is lower. People at old age, more prevalent if mortality is low, lose more life years in an ide- University Rotterdam, PO alised life table. The discounted life table decreases the burden of death strongly if mortality is high: Box 1738, 3000 DR Rotterdam, the the life lost by a person dying at a young age is discounted. -

Burden of Disease: What Is It and Why Is It Important for Safer Food?
Burden of disease: what is it and why is it important for safer food? What is ‘burden of disease’? Burden of disease is concept that was developed in the 1990s by the Harvard School of Public Health, the World Bank and the World Health Organization (WHO) to describe death and loss of health due to diseases, injuries and risk factors for all regions of the world.1 The burden of a particular disease or condition is estimated by adding together: • the number of years of life a person loses as a consequence of dying early because of the disease (called YLL, or Years of Life Lost); and • the number of years of life a person lives with disability caused by the disease (called YLD, or Years of Life lived with Disability). Adding together the Years of Life Lost and Years of Life lived with Disability gives a single-figure estimate of disease burden, called the Disability Adjusted Life Year (or DALY). One DALY represents the loss of one year of life lived in full health (see text box for more explanation and examples). Looking at burden of disease using DALYs can reveal surprises about a population’s health. For example, the Global Burden of Disease 2004 Update suggests that neuropsychiatric conditions are the most important causes of disability in all regions of the world, accounting for around 33% of all years lived with disability among adults aged 15 years and over, but only 2.2% of deaths.2 Therefore while psychiatric disorders are not traditionally regarded as having a major impact on the health of populations, this picture is completely altered when the burden of disease is estimated using DALYs. -

Eye Disease 1 Eye Disease
Eye disease 1 Eye disease Eye disease Classification and external resources [1] MeSH D005128 This is a partial list of human eye diseases and disorders. The World Health Organisation publishes a classification of known diseases and injuries called the International Statistical Classification of Diseases and Related Health Problems or ICD-10. This list uses that classification. H00-H59 Diseases of the eye and adnexa H00-H06 Disorders of eyelid, lacrimal system and orbit • (H00.0) Hordeolum ("stye" or "sty") — a bacterial infection of sebaceous glands of eyelashes • (H00.1) Chalazion — a cyst in the eyelid (usually upper eyelid) • (H01.0) Blepharitis — inflammation of eyelids and eyelashes; characterized by white flaky skin near the eyelashes • (H02.0) Entropion and trichiasis • (H02.1) Ectropion • (H02.2) Lagophthalmos • (H02.3) Blepharochalasis • (H02.4) Ptosis • (H02.6) Xanthelasma of eyelid • (H03.0*) Parasitic infestation of eyelid in diseases classified elsewhere • Dermatitis of eyelid due to Demodex species ( B88.0+ ) • Parasitic infestation of eyelid in: • leishmaniasis ( B55.-+ ) • loiasis ( B74.3+ ) • onchocerciasis ( B73+ ) • phthiriasis ( B85.3+ ) • (H03.1*) Involvement of eyelid in other infectious diseases classified elsewhere • Involvement of eyelid in: • herpesviral (herpes simplex) infection ( B00.5+ ) • leprosy ( A30.-+ ) • molluscum contagiosum ( B08.1+ ) • tuberculosis ( A18.4+ ) • yaws ( A66.-+ ) • zoster ( B02.3+ ) • (H03.8*) Involvement of eyelid in other diseases classified elsewhere • Involvement of eyelid in impetigo -

In the Prevention of Occupational Diseases 94 7.1 Introduction
Report on the current situation in relation to occupational diseases' systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects ‘Report on the current situation in relation to occupational diseases’ systems in EU Member States and EFTA/EEA countries, in particular relative to Commission Recommendation 2003/670/EC concerning the European Schedule of Occupational Diseases and gathering of data on relevant related aspects’ Table of Contents 1 Introduction 4 1.1 Foreword .................................................................................................... 4 1.2 The burden of occupational diseases ......................................................... 4 1.3 Recommendation 2003/670/EC .................................................................. 6 1.4 The EU context .......................................................................................... 9 1.5 Information notices on occupational diseases, a guide to diagnosis .................................................................................................. 11 1.6 Objectives of the project ........................................................................... 11 1.7 Methodology and sources ........................................................................ 12 1.8 Structure of the report .............................................................................. 15 2 Developments -

The Role of Time Preference on Wealth
THE ROLE OF TIME PREFERENCE ON WEALTH _______________________________________ A Thesis presented to the Faculty of the Graduate School at the University of Missouri-Columbia _______________________________________________________ In Partial Fulfillment of the Requirements for the Degree Master of Science _____________________________________________________ by ANDREW MARK ZUMWALT Dr. Deanna L. Sharpe, Thesis Co-Supervisor Dr. Sandra J. Huston, Thesis Co-Supervisor December 2008 The undersigned, appointed by the dean of the Graduate School, have examined the thesis entitled THE ROLE OF TIME PREFERENCE ON WEALTH presented by Andrew Mark Zumwalt, a candidate for the degree of master of science, and hereby certify that, in their opinion, it is worthy of acceptance. Professor Deanna L. Sharpe Professor Sandra J. Huston Professor Thomas Johnson ad maiorem dei gloriam ACKNOWLEDGEMENTS All throughout my life, I have been supported by strong individuals. These people have been the pillars of my success, and without their influence and guidance, I would be nowhere near where I am now. I can only hope that I have, in turn, enriched their lives. I aspire to fulfill a similar role for the young men and women I meet. While I believe that my success has been caused by the cumulative efforts of many individuals, I would like to take this limited space to thank those that have helped with this part of my life. First, I would like to thank the members of my committee. Dr Thomas Johnson’s experience from agricultural economics provided insight into overlooked ideas in my research when viewed in a broader context. He has also been extremely understanding with regard to interesting timetables, and I’ve thoroughly enjoyed learning from him in both inside and outside the classroom. -

European Conference on Rare Diseases
EUROPEAN CONFERENCE ON RARE DISEASES Luxembourg 21-22 June 2005 EUROPEAN CONFERENCE ON RARE DISEASES Copyright 2005 © Eurordis For more information: www.eurordis.org Webcast of the conference and abstracts: www.rare-luxembourg2005.org TABLE OF CONTENT_3 ------------------------------------------------- ACKNOWLEDGEMENTS AND CREDITS A specialised clinic for Rare Diseases : the RD TABLE OF CONTENTS Outpatient’s Clinic (RDOC) in Italy …………… 48 ------------------------------------------------- ------------------------------------------------- 4 / RARE, BUT EXISTING The organisers particularly wish to thank ACKNOWLEDGEMENTS AND CREDITS 4.1 No code, no name, no existence …………… 49 ------------------------------------------------- the following persons/organisations/companies 4.2 Why do we need to code rare diseases? … 50 PROGRAMME COMMITTEE for their role : ------------------------------------------------- Members of the Programme Committee ……… 6 5 / RESEARCH AND CARE Conference Programme …………………………… 7 …… HER ROYAL HIGHNESS THE GRAND DUCHESS OF LUXEMBOURG Key features of the conference …………………… 12 5.1 Research for Rare Diseases in the EU 54 • Participants ……………………………………… 12 5.2 Fighting the fragmentation of research …… 55 A multi-disciplinary approach ………………… 55 THE EUROPEAN COMMISSION Funding of the conference ……………………… 14 Transfer of academic research towards • ------------------------------------------------- industrial development ………………………… 60 THE GOVERNEMENT OF LUXEMBOURG Speakers ……………………………………………… 16 Strengthening cooperation between academia -
Neurodegeneration in Accelerated Aging
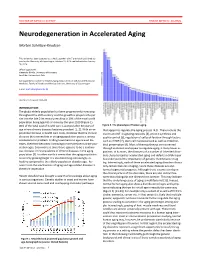
DOCTOR OF MEDICAL SCIENCE DANISH MEDICAL JOURNAL Neurodegeneration in Accelerated Aging Morten Scheibye-Knudsen This review has been accepted as a thesis together with 7 previously published pa- pers by the University of Copenhagen, October 16, 2014 and defended on January 14, 2016 Official opponents: Alexander Bürkle, University of Konstanz Lars Eide, University of Oslo Correspondence: Center for Healthy Aging, Department of Cellular and Molecular Medicine, Faculty of Health and Medical Sciences, University of Copenhagen E-mail: [email protected] Dan Med J 2016;63(11):B5308 INTRODUCTION The global elderly population has been progressively increasing throughout the 20th century and this growth is projected to per- sist into the late 21st century resulting in 20% of the total world population being aged 65 or more by the year 2100 (Figure 1). 80% of the total cost of health care is accrued after 40 years of Figure 2. The phenotype of human aging. age where chronic diseases become prevalent [1, 2]. With an ex- that appear to regulate the aging process [4,5]. These include the ponential increase in health care costs, it follows that the chronic insulin and IGF-1 signaling cascades [4], protein synthesis and diseases that accumulate in an aging population poses a serious quality control [6], regulation of cell proliferation through factors socioeconomic problem. Finding treatments to age related dis- such as mTOR [7], stem cell maintenance 8 as well as mitochon- eases, therefore becomes increasingly more pertinent as the pop- drial preservation [9]. Most of these pathways are conserved ulation ages. Even more so since there appears to be a continu- through evolution and appear to regulate aging in many lower or- ous increase in the prevalence of chronic diseases in the aging ganisms. -

Defining Malaria Burden from Morbidity and Mortality Records, Self Treatment Practices and Serological Data in Magugu, Babati District, Northern Tanzania
Tanzania Journal of Health Research Volume 13, Number 2, April 2011 Defining malaria burden from morbidity and mortality records, self treatment practices and serological data in Magugu, Babati District, northern Tanzania CHARLES MWANZIVA1*, ALPHAXARD MANJURANO2, ERASTO MBUGI3, CLEMENT MWEYA4, HUMPHREY MKALI5, MAGGIE P. KIVUYO6, ALEX SANGA7, ARNOLD NDARO1, WILLIAM CHAMBO8, ABAS MKWIZU9, JOVIN KITAU1, REGINALD KAVISHE11, WIL DOLMANS10, JAFFU CHILONGOLA1 and FRANKLIN W. MOSHA1 1Kilimanjaro Clinical Research Institute, P. O. Box 2236, Moshi, Tanzania 2Joint Malaria Programme, Moshi, Tanzania 3Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania 4Tukuyu Medical Research Centre, Tukuyu, Tanzania 5Tabora Medical Research Centre, Tabora, Tanzania 6Ngongongare Medical Research Station, Usa River, Tanzania 7St. John University of Tanzania, Dodoma, Tanzania 8Amani Medical Research Centre, Muheza, Tanzania 9Magugu Health Centre, Babati, Manyara, Tanzania 10 Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands Abstract: Malaria morbidity and mortality data from clinical records provide essential information towards defining disease burden in the area and for planning control strategies, but should be augmented with data on transmission intensity and serological data as measures for exposure to malaria. The objective of this study was to estimate the malaria burden based on serological data and prevalence of malaria, and compare it with existing self-treatment practices in Magugu in Babati District of northern Tanzania. Prospectively, 470 individuals were selected for the study. Both microscopy and Rapid Diagnostic Test (RDT) were used for malaria diagnosis. Seroprevalence of antibodies to merozoite surface proteins (MSP- 119) and apical membrane antigen (AMA-1) was performed and the entomological inoculation rate (EIR) was estimated. To complement this information, retrospective data on treatment history, prescriptions by physicians and use of bed nets were collected. -
National System for Recording and Notification of Occupational Diseases Practical Guide
InternationalInternational LabourLabour OfficeOffice GenevaGeneva National System for Recording and Notification of Occupational Diseases Practical guide Programme on Safety and Health at Work and the Environment (SafeWork) International Labour Organization Route des Morillons 4 CH -1211 Geneva 22 Switzerland TEL. + 41 22 7996715 FAX + 41 22 7996878 E-mail : safework @ ilo.org www.ilo.org / safework ILO National System for Recording and Notification of Occupational Diseases – Practical guide ISBN 978-92-2-127057-7 9 789221 270577 Programme on Safety and Health at Work and the Environment (SafeWork) National System for Recording and Notification of Occupational Diseases Practical guide International Labour Office, Geneva Copyright © International Labour Organization 2013 First published 2013 Publications of the International Labour Office enjoy copyright under Protocol 2 of the Universal Copyright Convention. Never- theless, short excerpts from them may be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or translation, application should be made to ILO Publications (Rights and Permissions), International Labour Office, CH-1211 Geneva 22, Switzerland, or by email: [email protected]. The International Labour Office welcomes such applications. Libraries, institutions and other users registered with reproduction rights organizations may make copies in accordance with the licences issued to them for this purpose. Visit www.ifrro.org to find the reproduction rights organization in your country. -

The Geographies of Soft Paternalism in the UK: the Rise of the Avuncular State and Changing Behaviour After Neoliberalism
The Geographies of Soft Paternalism in the UK: the rise of the avuncular state and changing behaviour after neoliberalism Rhys Jones, Jessica Pykett and Mark Whitehead, Aberystwyth University Forthcoming, Geography Compass Abstract Soft paternalism or libertarian paternalism has emerged as a new rationality of governing in the UK under New Labour, denoting a style of governing which is aimed at both increasing choice and ensuring welfare. Popularised in Thaler and Sunstein’s best-selling title, Nudge, the approach of libertarian paternalism poses new questions for critical human geographers interested in how the philosophies and practices of the Third Way are being adapted and developed in a range of public policy spheres, including the environment, personal finance and health policy. Focusing specifically on the case of the UK, this article charts how soft paternalism appeals to the intellectual influences of behavioural economics, psychology and the neurosciences, amongst others, to justify government interventions based on the ‘non-ideal’ or irrational citizen. By identifying the distinctive mechanisms associated with this ‘behaviour change’ agenda, such as ‘choice architecture’, we explore the contribution of behavioural geographies and political geographies of the state to further understanding of the techniques and rationalities of governing. 1 The Geographies of Soft Paternalism: the rise of the avuncular state and changing behaviour after neoliberalism 1. Introduction: The Chicago School comes to Britain Mark II. On March 24 2009, David Cameron stood next to the eminent behavioural economist Richard Thaler at the London Stock Exchange. David Cameron was in the City of London to deliver his keynote speech on banking reform and the Tory’s response to the credit crunch. -

Incidence, Mortality, Disability-Adjusted Life Years And
Original article The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013 Juanita A Haagsma,1,60 Nicholas Graetz,1 Ian Bolliger,1 Mohsen Naghavi,1 Hideki Higashi,1 Erin C Mullany,1 Semaw Ferede Abera,2,3 Jerry Puthenpurakal Abraham,4,5 Koranteng Adofo,6 Ubai Alsharif,7 Emmanuel A Ameh,8 9 10 11 12 Open Access Walid Ammar, Carl Abelardo T Antonio, Lope H Barrero, Tolesa Bekele, Scan to access more free content Dipan Bose,13 Alexandra Brazinova,14 Ferrán Catalá-López,15 Lalit Dandona,1,16 Rakhi Dandona,16 Paul I Dargan,17 Diego De Leo,18 Louisa Degenhardt,19 Sarah Derrett,20,21 Samath D Dharmaratne,22 Tim R Driscoll,23 Leilei Duan,24 Sergey Petrovich Ermakov,25,26 Farshad Farzadfar,27 Valery L Feigin,28 Richard C Franklin,29 Belinda Gabbe,30 Richard A Gosselin,31 Nima Hafezi-Nejad,32 Randah Ribhi Hamadeh,33 Martha Hijar,34 Guoqing Hu,35 Sudha P Jayaraman,36 Guohong Jiang,37 Yousef Saleh Khader,38 Ejaz Ahmad Khan,39,40 Sanjay Krishnaswami,41 Chanda Kulkarni,42 Fiona E Lecky,43 Ricky Leung,44 Raimundas Lunevicius,45,46 Ronan Anthony Lyons,47 Marek Majdan,48 Amanda J Mason-Jones,49 Richard Matzopoulos,50,51 Peter A Meaney,52,53 Wubegzier Mekonnen,54 Ted R Miller,55,56 Charles N Mock,57 Rosana E Norman,58 Ricardo Orozco,59 Suzanne Polinder,60 Farshad Pourmalek,61 Vafa Rahimi-Movaghar,62 Amany Refaat,63 David Rojas-Rueda,64 Nobhojit Roy,65,66 David C Schwebel,67 Amira Shaheen,68 Saeid Shahraz,69 Vegard Skirbekk,70 Kjetil Søreide,71 Sergey Soshnikov,72 Dan J Stein,73,74 Bryan L Sykes,75 Karen M Tabb,76 Awoke Misganaw Temesgen,77 Eric Yeboah Tenkorang,78 Alice M Theadom,79 Bach Xuan Tran,80,81 Tommi J Vasankari,82 Monica S Vavilala,57 83 84 85 ▸ Vasiliy Victorovich Vlassov, Solomon Meseret Woldeyohannes, Paul Yip, Additional material is 86 87 88,89 1 published online only.